
ABSTRACT
The national picture of the comparative costs and diagnoses of hospitalised homeless patients are examined using the ‘no fixed abode’ flag in English hospital statistics. Comparable studies sample patients in single cities, eg New York and Toronto. The most common diagnosis is substance misuse; the share of homeless NHS patients with this diagnosis is rising, and now equals that found in North American cities. About half of the cost of homeless patients relates to diagnoses of mental illness, although these comprise a much smaller share of homeless patients than in North America. Hospital costs for homeless patients – both total and per admission – have fallen significantly in recent years, primarily because of fewer admissions and shorter lengths of stay for mentally ill patients. Aims to reduce NHS costs at the level of individual institutions have often shaped policy. Broader policy to prevent and reduce homelessness offers substantial long-term reductions in the cost of chronic care.
Introduction
Research has improved awareness of the extremely poor health of the homeless1–5 and given a better understanding of the effectiveness of community-based healthcare interventions.3,6–8 A more recent focus of reform, driven by the distinct morbidities and pre- and post-treatment circumstances of homeless patients, is the redesign of hospital services to offer cost-effective patient pathways that better address the needs of the homeless. Pioneering initiatives such as the Boston Health Care for the Homeless Program9 and Pathway10,11 signal international recognition of the patient value and cost savings that might result from more informed hospital service planning, including specialist staff and partnership with a range of external health and non-health services. However, with the exception of one city- and one hospital-level study carried out in New York12 and Toronto,13 respectively, little is known about the comparative use and cost of hospital services by the homeless. Other North American studies focus on the impact of particular interventions.14–18 Our purpose in this article is to outline the use and cost of hospital services for the homeless in England in order to increase strategic understanding of how best to deliver healthcare for the homeless and those vulnerable to homelessness.
Methods
We used England's NHS hospital episode statistics, giving national coverage between April 2007 and March 2011, in order to identify the use of hospital services by the homeless and to contrast this use with that of a comparative sample of the homed. The homeless are identified by the patient being recorded on admission as having ‘no fixed abode’ (NFA), and the relatively large number of admissions – 35,518 – suggests that this group consists of more than rough sleepers (for example, it likely includes some of those living in hostels for the homeless). To help ensure that the data is focused on the comparative experience of homeless patients, rather than, for example, non-homeless patients seeking anonymity, some cases were excluded: those outside of the age range 16–64 years inclusive, those with poor data quality, and those relating to pregnancy terminations, obstetrics, or neonatal care. This method of identifying homeless patients is inexact; for example, some homeless patients may provide the address of a hostel, and so will be placed in the comparison group. Nonetheless, various sample evidence is consistent with other evidence on the homeless population.19 The same exclusions were used to extract a comparison group of fixed abode episodes. NFA admissions over the period were 80% male, and had a mean age of 38.7 years. By contrast, the 23.7 million comparison admissions were 47% male and had a mean age of 44.6 years (mode = 63 years). The percentage of homeless patients that are male is almost identical in New York, Toronto and England (80–82%).
Results
Comparative diagnoses
Unsurprisingly and in common with existing evidence,3,5 the NFA and comparison case mixes differ markedly. Table 1 presents Healthcare Resource Groups (HRGs) that are common among the homeless. Thus, in 2010–11, four HRGs relating to alcohol, drugs and ‘poisoning, toxic, environmental and unspecified effects’ were more than 10 times more common in the homeless data, and mental health HRGs were over six times more common. Considerable change is also apparent: the share of the substance misuse HRGs rose between 2007–8 and 2010–11 from 20.9% to 27.7% of NFA episodes, with no such rise in the comparison group. Although HRG data does not distinguish between alcohol and drugs, this rise is consistent with data showing considerably increased rates of alcohol dependence between 2003 and 2009 in patients at a specialist primary care centre in Leicester.20 Other evidence from the Pathway initiative at University College London Hospital suggests common ‘tri morbidity’ of physical ill-health, mental ill-health and substance misuse.10 Other specific issues highlighted in a 2006 review3 include blood-borne virus infections (resulting from drug abuse), foot trauma, inflammatory skin conditions, skin infestations and respiratory illnesses, including pneumonia and (often latent) tuberculosis.
Admission by nature of diagnosis
The diagnoses of English NFAs resemble those reported for US and Canadian urban homeless hospital admissions.12,13 Comparisons with homeless patients in 1992–93 in New York12 suggest an almost identical fraction – approximately a quarter – of homeless patients are diagnosed with substance abuse. However, the percentage of English homeless with mental health diagnoses is just under half that found in both the New York and Toronto patient samples. This may reflect professional differences in mental health diagnosis, or health insurance coverage and social policy in England that diminishes the risk of the mentally ill becoming homeless. The recent US health reforms, which extend coverage, may lead to fewer mentally ill patients becoming homeless.
Fluctuations in activity (2007–11)
Admissions and bed days in the NFA and comparison patient groups covering the 4-year period are summarised in Table 2; these data are of particular interest because they cover the 2008–9 recession, its aftermath, and the April 2009 removal of ring-fencing for the ‘supporting people’ budget used by local authorities to fund hostel and other homelessness services.
Comparison of cost and activity
The number of NFA bed days and admissions first started to rise with the onset of the ‘great recession’ in 2008–9, but fell by 24% between 2008–9 and 2009–10, which coincided with the removal of the ring-fence of homeless hostel funding. It also coincided with available evidence on declining rough sleepers: there was a fall, 2008–9 to 2009–10, of about 15% in the number of rough sleepers in London that were not migrants from eastern Europe.19 Those homeless following international migration are likely to have differentiated health, inpatient needs and eligibility. Statutory homeless acceptances also declined from 135,590 in 2003 to 41,780 in 2010, and then increased to 53,410 by 2014.21
In-hospital mortality among homeless patients
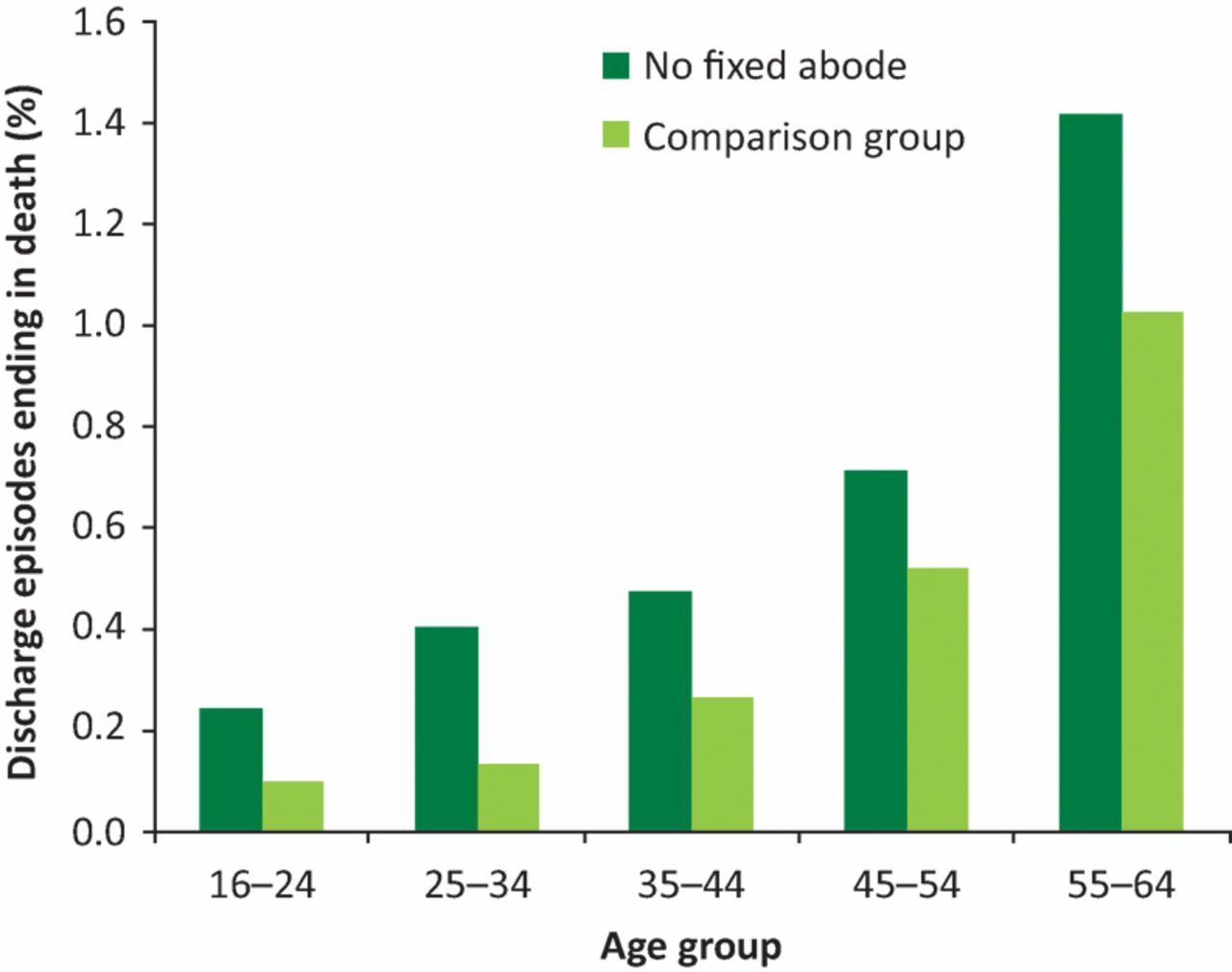
As well as being a key outcome, in-hospital mortality indicates whether homelessness is primarily a problem of early death or of chronic sickness. Across all 4 years, there were a total of 214 deaths recorded in the NFA sample (0.578% of all NFA discharge episodes). There were 125,455 deaths (0.52% of discharge episodes) in the comparison group. The overall NFA in-hospital mortality rate was therefore approximately 10% higher. However, when the mortality rates are broken down by age (as in Fig 1), the NFA group has a 37% higher rate in those aged 45–54 years and 55–64 years, rising to 80% higher in the 35–44 age group, 205% in the 25–34 age group and 145% in the 16–24 age group (although these youngest groups represent a smaller share of deaths). The NFA group therefore have a markedly higher age-corrected in-hospital death rate. GPs in England, surveyed by the Department of Health,22 have shown admission rates that are at least twice as high for homeless patients, which in turn suggests that the homeless are more than three times as likely to die in hospital than comparators. This is consistent with the findings from a 2009 study in Glasgow.2 This relative hospital mortality, although very high, nevertheless suggests that only a small fraction of NFA cases end in death during the homeless phase, and indicates that for many more cases, there is a likelihood of years of chronic illness before premature death.
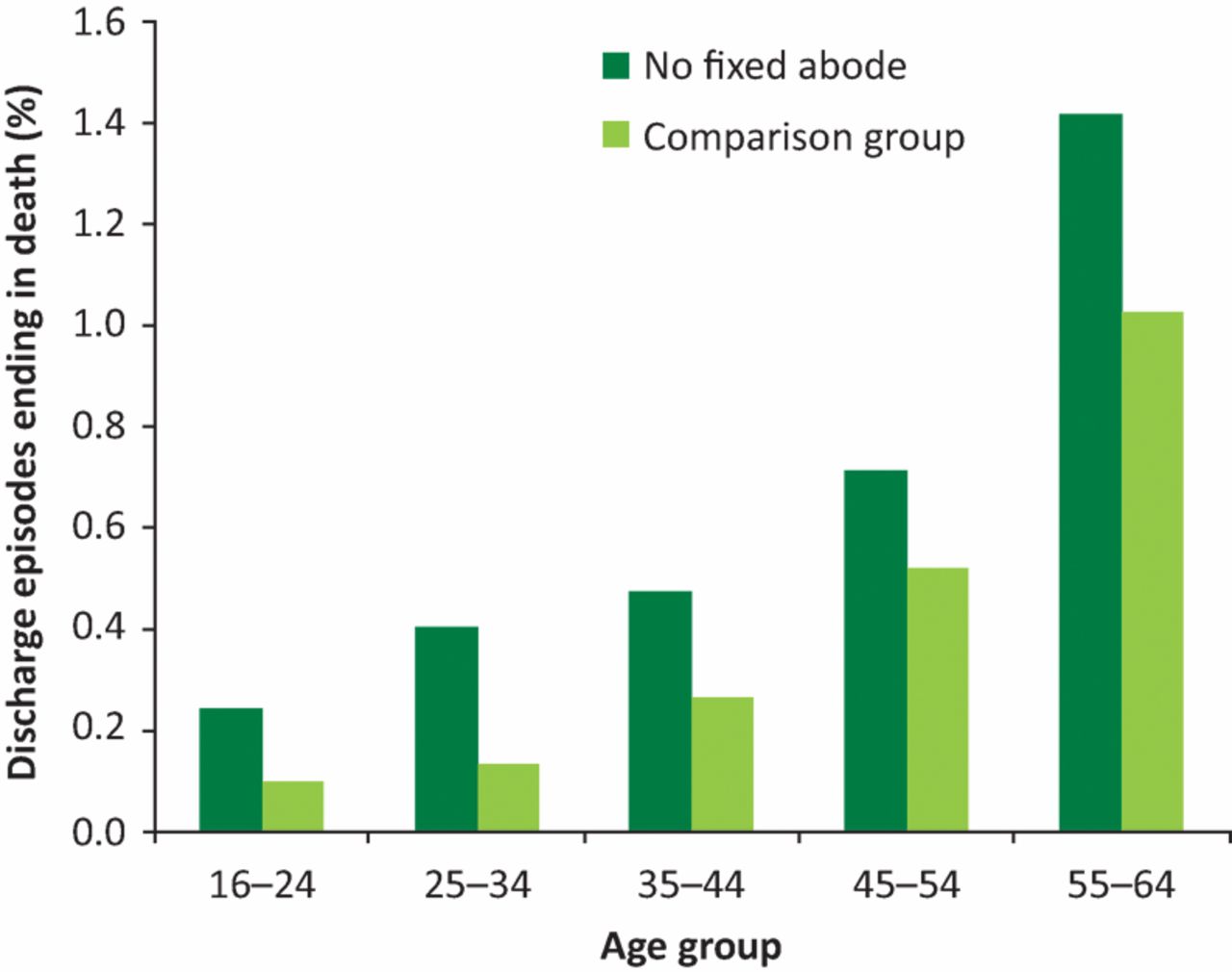
In-hospital mortality rates.
Self-discharge and emergency readmission
There appears to be significant scope for improving the discharge process to reduce the rate of emergency readmission: 12–15% of the NFA episodes end in self-discharge, notably higher than the 1.5–1.75% in the comparison group. A 2011 retrospective study23 showed that the establishment of a discharge coordinator (aimed at ensuring that patients are not discharged back onto the street) reduced emergency NFA readmissions by one third relative to no previous provision. Better discharge planning was also a key element of a 2016 randomised controlled trial at the Royal London Hospital.24
To identify the extent to which the higher rate of self-discharge for NFA episodes is driven by their HRG mix, a calculation was made of the number of NFA self-discharges that would occur if the NFA group had the same HRG-specific self-discharge rates as the comparison group. The resulting self-discharge rate is 5.4%. This is notably less than the actual NFA self-discharge rate of 12–15%, but more than the comparison group figure of 1.5–1.75%, which implies that while the NFA case mix partly explains their higher rate of self-discharge, it is by no means the whole explanation.
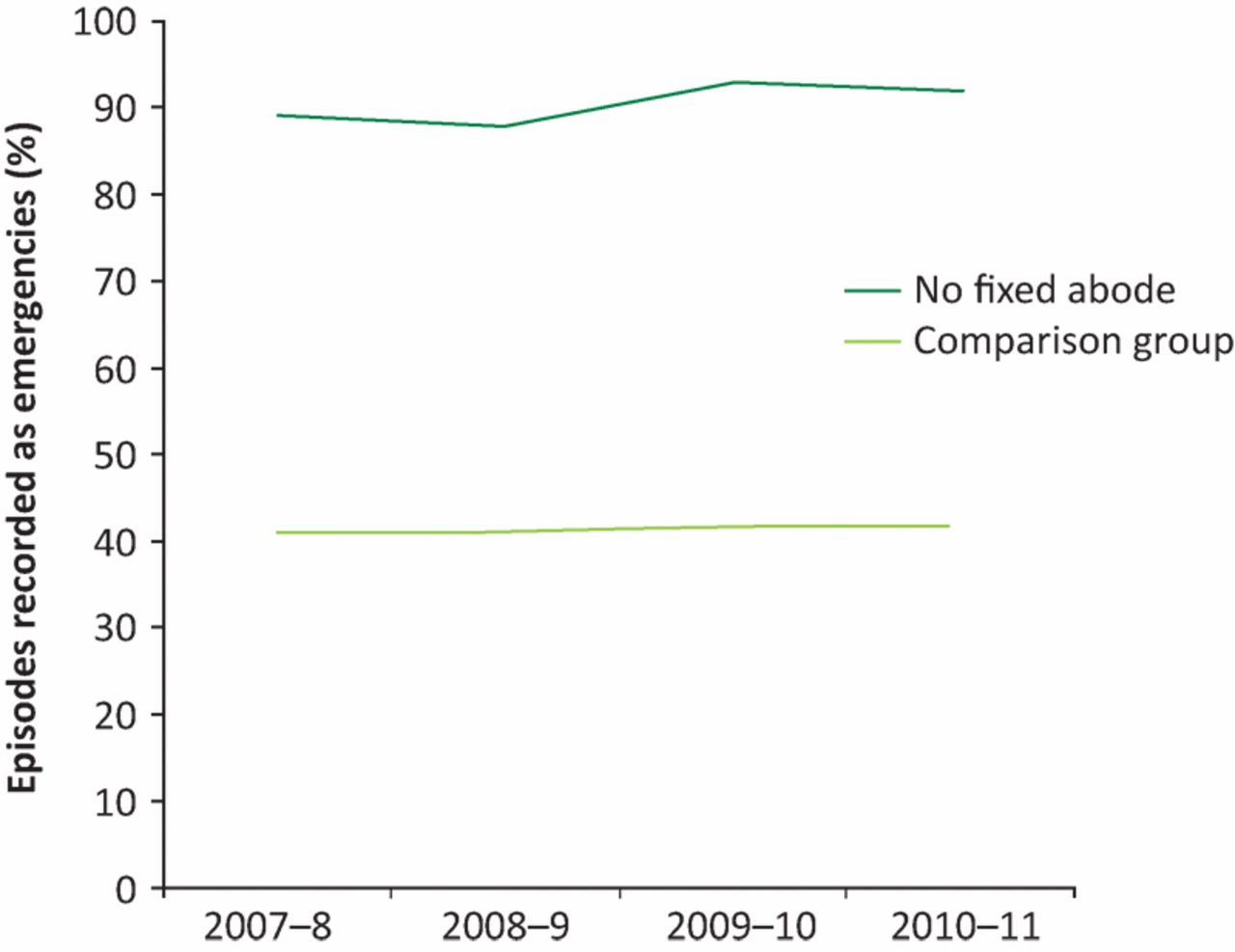
No less than 87% of NFA episodes are recorded as emergencies versus 42% in the comparison population (Fig 2). Furthermore, the percentage of NFA emergency readmissions increased from 88.9% in 2007–8 to 91.9% in 2010–11, a trend that is indicative of little progress in engagement with primary care, and highlights the value of revisiting the potential role of specialist GP practices for the homeless.

Percentage of episodes recorded as emergencies.
Cost of homeless hospital admission
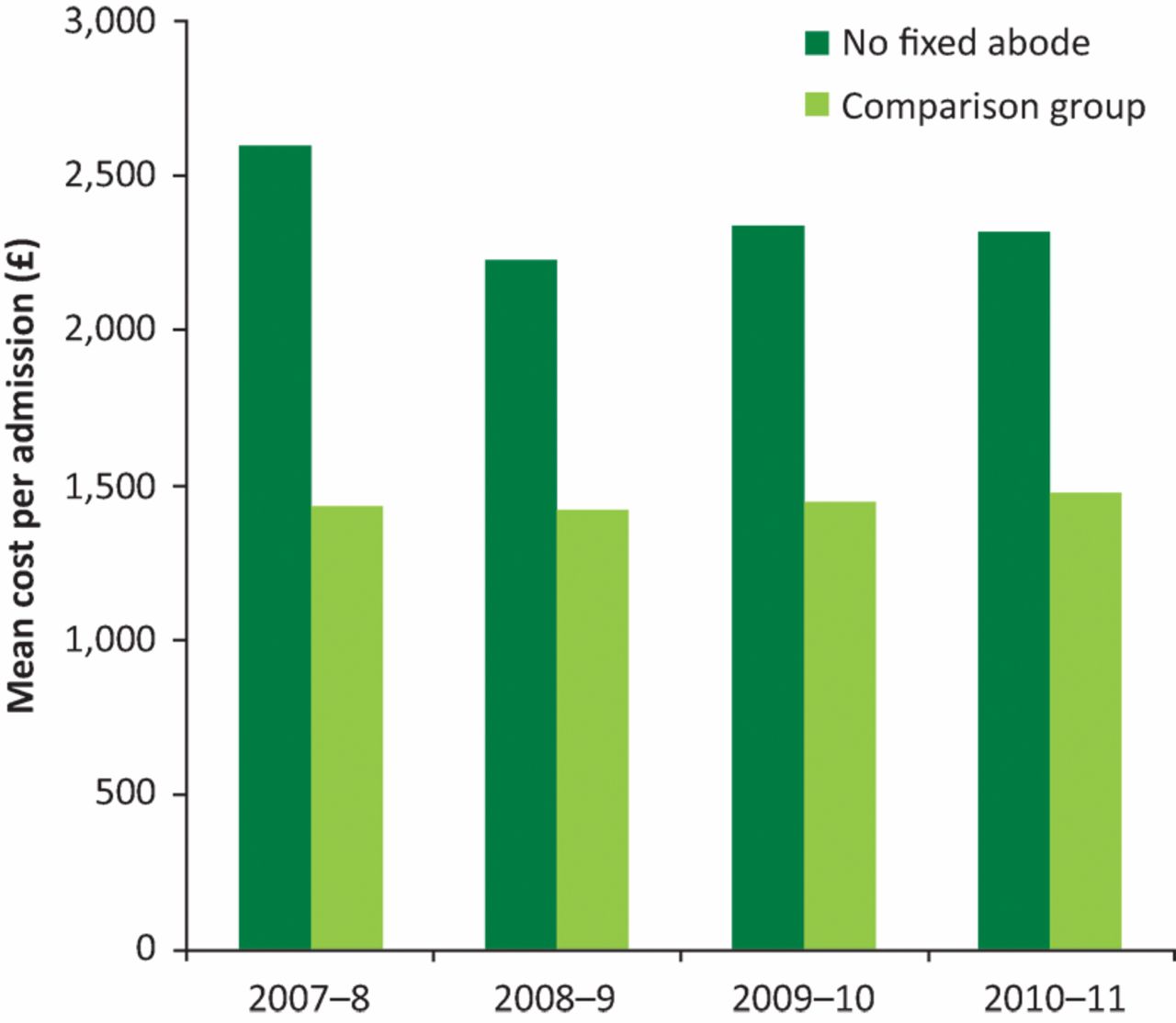
The potential to reduce the cost of homeless admissions while improving patient care has been a key argument for new pathway approaches. There are several reasons why homeless patients may experience longer (and more expensive) hospital stays. Many will rely upon hostel or other forms of public accommodation that may not always be available at the time of discharge. The multiple morbidities of homeless patients may also take added time to resolve. In addition, their substantially different case mix is likely to have an impact on both length of stay and cost. Table 2 includes a broad costing for both the NFA and comparison groups to highlight the differences in their resource use. A unit cost per bed day is applied to mental health episodes (ie those in Chapter T of HRG version 3.5), with other HRGs costed using the national tariff (without adjusting for short or long stays, using underlying tariff data where tariff estimates are not available). Table 2 and Fig 3 show that over this period, the cost per NFA admission was 60–80% higher than for the comparison group, partly because the length of stay for NFA patients was three times longer.
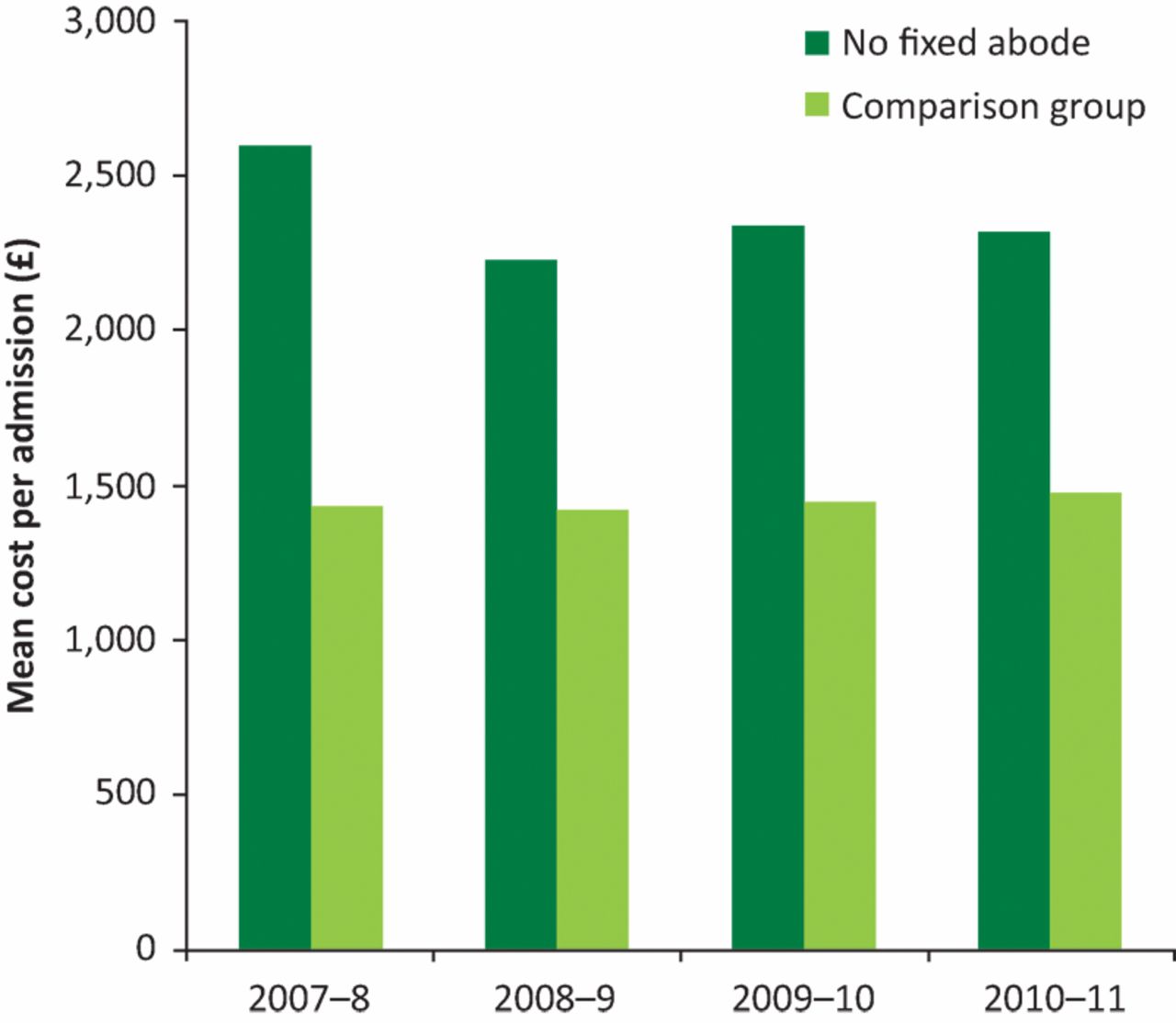
Cost per admission. Costs are calculated using 2007–8 prices.
Impact of mental health on cost
Approximately half of the cost of hospital stays for the homeless relates to mental health (excluding substance misuse), compared with 8–9% in the comparison group. This high share of cost is due, in both groups, to a high average length of stay for the mental health category – 30 days. Mental health only represents approximately 10% of all NFA episodes and 1–2% of comparison group episodes, but amounts to 50–60% of NFA bed days and 20% for the comparison group. It is nonetheless important to note that the total cost and number of NFA mental health bed days declined by approximately one third between 2007–8 and 2010–11. During this period – following the financial crisis – the health service sought to make economies in anticipation of (at best) flat real health spending post-2010. Strikingly, the comparison group does not show a similar decrease, which raises the question of whether economies have been found among this especially dependent population.
Looking at the overall costing (including non-mental-health HRGs), the cost per NFA admission has decreased by 11% while that for the comparison group has increased by 3. This relative change largely reflects the larger decline in the number and cost of NFA mental health episodes.
To identify the extent to which case mix explains the higher NFA length of stay (and, by extension, cost), we standardised by HRG: we calculated the NFA average length of stay per episode assuming this length of stay were the same as the comparison group for each HRG. Before adjustment, average NFA lengths of stay were 178% longer. After correcting for HRG, the NFA lengths of stay were only about 7.3% longer than would be expected for the homed, therefore, the higher length of stay per episode for NFA patients is largely explained by case mix. Notably, however, spell lengths and estimated costs per admission for 2010–11 were about 18% higher for homeless mental health patients.
Homeless patients appear to have a longer average length of stay (and, by extension, higher cost) than the comparator group. However, this largely reflects the mental health diagnoses rather than homelessness per se. By contrast, the New York study12 found a 36% longer length of stay for homeless patients after adjusting for diagnosis, as well as coexisting illnesses and demographic characteristics. While length of stay for the homeless in England was only 7.3% higher after controlling for diagnosis and leaves little acute resource to be saved by pathway initiatives, this may nonetheless be possible – as found by the Pathway initiative at University College London Hospital (UCLH).10 The UCLH Pathway responds to 300–500 admissions each year and coordinates care with a range of external organisations, inside and outside of healthcare, to resolve the problems in each patient's life. The service consists of two specialist nurses, four GP sessions, as well as a care navigator supervisor and several care navigators.11 The care navigators are formerly homeless people trained to help those being treated by the service. The evidence that the NHS provides a less generous incremental length of stay for the homeless than the North American acute services that have been studied is disconcerting, if not surprising, given that universal coverage has been recently accompanied by a focus on hospital cost reductions.
Conclusion
Health policy influences the health of the homeless, the incidence of homelessness and the demand of the former homeless for services such as social care, housing and the police, as well as health. It is important to be mindful that the acute services offered to the homeless will carry long-term consequences for both patient health and public expenditure, which are likely to amount to a far greater sum than the cost of a typical brief hospital spell. It is worth emphasising that although the homeless incur a loss of expected life of 10–20 years,4 this implies that an immediate death during or shortly after becoming homeless is not typical, with most homeless patients continuing to live with chronic illnesses for many years. The long-term cost–benefit implications of many acute services for the homeless contrast with a policy environment in which it has been commonplace for policy initiatives for acute services to demonstrate how reform would reduce short-term hospital costs. Further analysis is needed of the various long-term costs that result from alternative approaches to treating homeless patients in the acute phase.
Reform in the acute and post-acute treatment of homeless patients may draw from studies of the development of acute and post-acute accommodation for patients who are too frail to recover on the streets but are not ill enough to be in a hospital, as suggested by US ‘respite care’.25 Better management of healthcare for the homeless (through interventions such as improved discharge or better management in the community), and better policy to address the causes of homelessness offer potential long- as well as short-term cost savings, together with health benefits. At this time of financial ‘austerity’, short-term expenditure on hospital care has been contained by reducing mental health inpatient treatment but with only modest attention to the consequence for longer term costs or to policies which, by addressing homelessness before and at its inception, could mitigate the long-term cost of community and NHS chronic care.
Further refinement of hospital episode statistics to broaden the address options that healthcare providers can enter, together with guidance on the definition of homelessness, could increase coverage and consistency of the data, giving a greater insight into overall levels of activity and how they are changing.
Conflicts of interest
The authors declare no conflicts of interest.
Author contributions
JW and BM drafted the manuscript. JW prepared the data. JW and BM conducted the statistical analysis. BM is the guarantor.
Acknowledgements
The late Aidan Halligan encouraged this project from its inception and we would like to dedicate the paper to his memory.
- © Royal College of Physicians 2016. All rights reserved.








{kind=link}
{kind=link}
{kind=link}