
ABSTRACT
Background Perioperative optimisation can improve outcomes for older people having surgery. Integration with primary care could improve quality and reduce variability in access to preoperative optimisation.
Aim Our aim was to explore attitudes, beliefs and behaviours of general practitioners (GPs) regarding the perioperative pathway, and evaluate enablers and barriers to GP-led preoperative optimisation.
Methods Stakeholder interviews (n=38) informed survey development. A purposive sampling frame was used to target delivery of online and paper surveys. Results were analysed using descriptive statistics.
Results We had 231 responses (response rate 32.7%). Enablers included belief among GPs that optimisation improves postoperative outcomes (86%) and that they have a role discussing modifiable risk factors with patients (85%). Barriers included low frequency exposure to older surgical patients, minimal training in perioperative medicine and rare interaction with perioperative services.
Conclusion This survey illustrates the importance of interprofessional education, cross-sector training opportunities and collaboration to deliver integrated preoperative optimisation for older people undergoing surgery.
Introduction
Increasing numbers of older people are having surgery.1 The advent of perioperative medicine has highlighted the need for closer collaboration between primary and secondary care, particularly in the management of older surgical patients who often have chronic health problems. While older people have much to gain from surgery, they are at high risk of adverse patient-reported, clinician-reported and process-related outcomes.2–4 Multidisciplinary preoperative optimisation services are increasingly advocated to mitigate this risk, with a growing evidence base to support improved postoperative outcomes and increasing attention to the expanding role of geriatricians in the care of the older surgical patient.5–8 Current models for preoperative optimisation are based within secondary care. From a clinical perspective, this model does not fully harness the expertise of primary care clinicians in optimising chronic health disease and promoting patient-led behaviour change; central tenets of preoperative optimisation. From a patient perspective, the transition of care between primary and secondary care has been highlighted for improvement in studies of experience-based codesign.9,10
The development of multidisciplinary preoperative optimisation services is supported by national reports and guidance.11–13 The initial evaluation of such secondary care services has resulted in a research recommendation from the National Institute for Health and Care Excellence.14 However, while these models are often based within secondary care, the NHS Long Term Plan advocates a proactive, prevention-focused health service spanning community and secondary care.15 Important advances toward more integrated surgical services include the Royal College of Anaesthetists’ toolkit, Fitter Better Sooner, endorsed by the Royal College of General Practitioners (RCGP) as well as the Centre for Perioperative Care, in which the RCGP is a partner.16,17 The toolkit consists of patient resources and provides general practitioners (GPs) with an opportunity to use their expertise in empowering self-care, thus facilitating earlier preoperative optimisation in the surgical pathway.18
Potential benefits of early primary care-based optimisation for older people undergoing surgery include full utilisation of the preoperative optimisation window; patient-centred, place-based care; and continuity of care in chronic disease management, acknowledging the surgical episode as a punctuation in the longer-term patient journey. Additionally, faced with the forecasted surge in elective surgery following the COVID-19 pandemic, there is renewed urgency and opportunity for developing integrated models of place-based or virtual care that reduce reliance on hospital-based outpatient services.19
Despite these potential benefits, the perspective of primary care clinicians regarding perioperative medicine and their role in the surgical pathway has not been evaluated. This survey aimed to explore the attitudes, beliefs and behaviours of GPs pertaining to perioperative medicine. Specifically, the role of GPs in the surgical pathway, and interactions between primary and secondary care were examined. Additionally, the enablers and barriers to primary care-based optimisation of older surgical patients were described.
Methods
Ethics approval was not required for this study, as discussed with the lead trust research and development team.
A survey (supplementary material S1) was developed based on themes identified through 38 stakeholder interviews with healthcare professionals from primary and secondary care, ensuring representation from relevant specialties and disciplines. See supplementary material S2 for details of professional groups included.
The survey included multiple-choice, ranking, Likert, dichotomous and open-ended questions. It was reviewed for readability, non-ambiguity and validated by 12 expert raters from primary and secondary care. Content validity, calculated using Lawshe’s method, was 0.79 which is above the validated threshold of 0.62 for 10 expert raters.20 The validated survey was piloted by a convenience sample of five GPs.
Data from NHS Digital were used to create a distribution curve of practice size, allowing definition of small, medium and large practices according to number of GP partners. Small practices were single-handed, medium practices had two to five GP partners, large practices had six to 10 GP partners and mega practices employed more than 10 GP partners. A purposive sampling frame ensured that practices of different sizes were represented in each of five geographical regions: the north; the midlands and the east; London; the south east; and the south west. Practices were then selected at random within each group. This approach to sampling aimed to deliver generalisable results in terms of practice size and location.
A bimodal delivery strategy was used, employing both online surveys and paper surveys between 15 January 2019 and 31 July 2019. Only fully trained GPs were targeted. A statement of participant information was provided via email invitation for online surveys, and on the covering page of paper surveys, with implied consent assumed on survey completion. SurveyMonkey was used to distribute online surveys through email invitation via practice managers, practice partners and direct to individual GPs, according to the preference of the GP practice. Three reminders were sent via email. To maximise response rates, paper surveys were also distributed at primary care meetings and educational events, where information regarding the size of the practice was available, in order to maintain fidelity to the sampling frame.
Survey results were analysed using basic descriptive statistics and reported by themes. It was beyond the scope of this work to formally analyse free text respondent views using qualitative methodology, but illustrative quotes are provided. See supplementary material S3 for all full text responses.
Results
Response rate
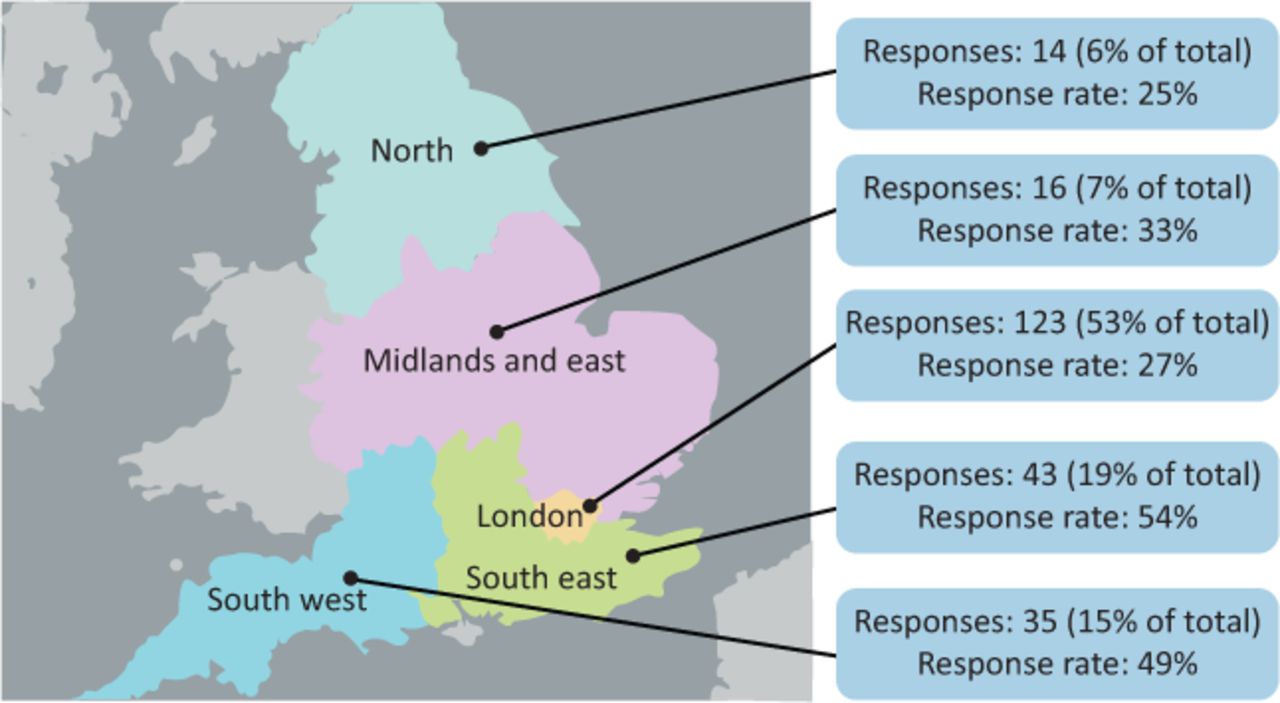
The survey was distributed to 706 GPs, with responses received from 231 (response rate of 32.7%). Online surveys accounted for 187 responses (81%), with a total of 44 paper survey responses (19%). Clinicians from the London region comprised 53% of total respondents, and response rate varied by region (Fig 1). Most of the respondents were practice partners (59%) followed by salaried GPs (28%). Locum GPs made up 8% of respondents and the remaining 5% of respondents included GP registrars, one retainer GP and one nurse practitioner.
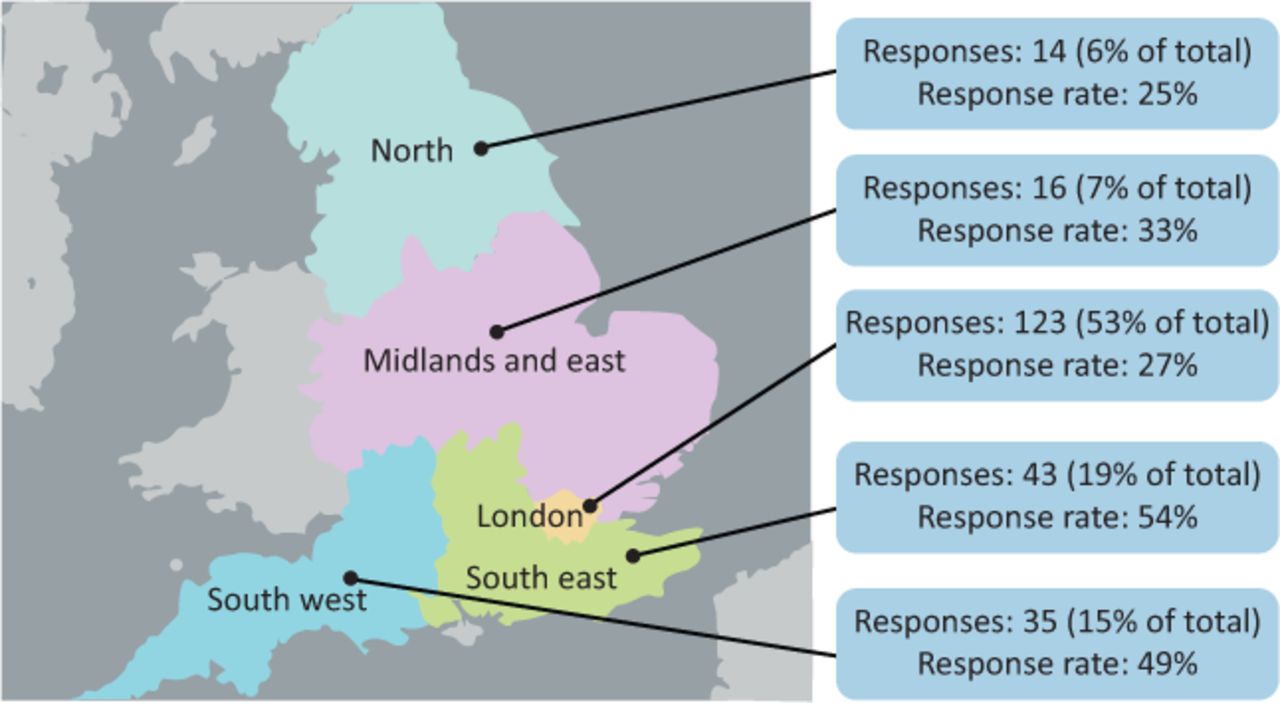
Survey response rate by region of England.
Referral frequency to surgical specialties from primary care
Over half of GP respondents had referred either zero (26%) or one (27%) patient over 65 years old to a surgical specialty in the past month. Forty per cent of respondents had referred two to five patients and 7% had referred six or more patients in the last month. Twenty per cent of GPs who had referred at least one patient to a surgical specialty in the past month reported that they perceived the risks of surgery to outweigh the benefits. Fifty-seven per cent reported having referred a patient for whom they could identify potentially modifiable risk factors for postoperative complications.
Self-perceived role of primary care in the perioperative pathway
Thirty-seven per cent of respondents reported that they had an important role in the surgical pathway. Eighty-seven per cent reported their role as a gatekeeper for referrals, with over 70% reporting a role in advocating for patients whom they felt would benefit from surgery (73%) or from a non-operative alternative (71%).
Eighty-five per cent of respondents believed it was their role to discuss modifiable risk factors for adverse perioperative outcome with patients. When faced with a hypothetical, high-risk, older surgical patient, 58% of GPs reported that they would assess for modifiable risk factors that could be optimised before referring to a surgical team. Forty-four per cent of respondents reported that they would develop an optimisation plan for the patient. Lack of time was reported as a barrier to medically optimising patients by 45% of respondents. Fig 2 illustrates the varied views of respondents regarding whether it is the role of secondary care or primary care to preoperatively optimise patients for surgery.
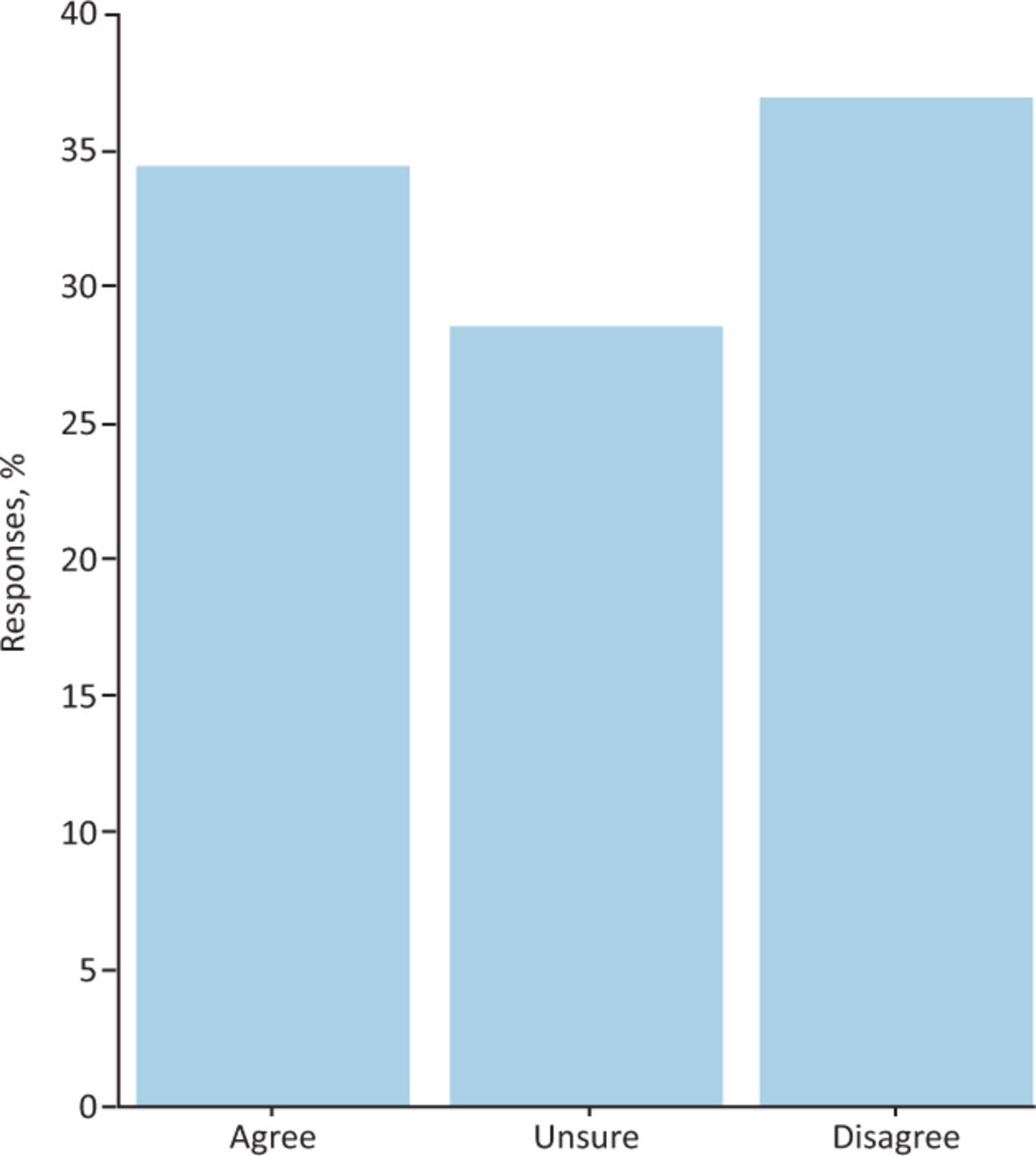
General practitioner responses to the statement: ‘It is the role of secondary care to optimise patients for surgery.’
Respondents reported that it was the role of the GP to engage in elements of shared decision making, including discussing alternatives to surgery (66%), what would happen if they did not have surgery (67%) and the perceived benefits of surgery (70%). Despite this, fewer GPs reported enacting these behaviours in practice, with 61% discussing alternatives to surgery, 47% discussing what would happen if the patient did not have surgery and 54% discussing the perceived benefits of surgery. Some respondents reported that a lack of knowledge about surgical alternatives was a driver for this discrepancy (Box 1). GPs also reported that the necessary information to lead these conversations was not communicated from surgical specialties, with 73% reporting that alternatives to surgery were not clear from the surgical correspondence, with 64% reporting that decision making was not clearly communicated. GPs were asked if they explained the risks, benefits and alternatives to surgery with respect to the last patient they referred to a surgical specialty; Box 1 provides illustrative free-text answers.
Discussion of factors important to shared decision making for surgery in the primary care setting: free text responses from general practitioners
Interaction with surgical specialties and perioperative medicine
Twenty-four per cent of GPs perceived that their assessment and evaluation of the patient was valued by the secondary care team. Respondents reported a lack of clarity in communication from surgical specialties. In particular, 88% reported that the plan for preoperative management was not clear, with 84% reporting an unclear overall plan.
The majority of respondents agreed that preoperative medical optimisation of older patients can improve postoperative outcomes (86%). Sixty-two per cent were unaware of perioperative medical services, although only 15% were aware that they may have access to geriatrician-led perioperative medicine services. A regional difference was noted in response to awareness of perioperative medical services; 4% of GPs from outside of London reported awareness of geriatrician-led perioperative medical services, compared with 27% of GPs from the London area. Additionally, 22% of GPs reported that they did not understand the role of perioperative medicine services. Again, a regional difference was apparent; 26% of GPs from outside London compared with 14% from London were unclear regarding the scope of perioperative medicine services.
GP training in perioperative medicine
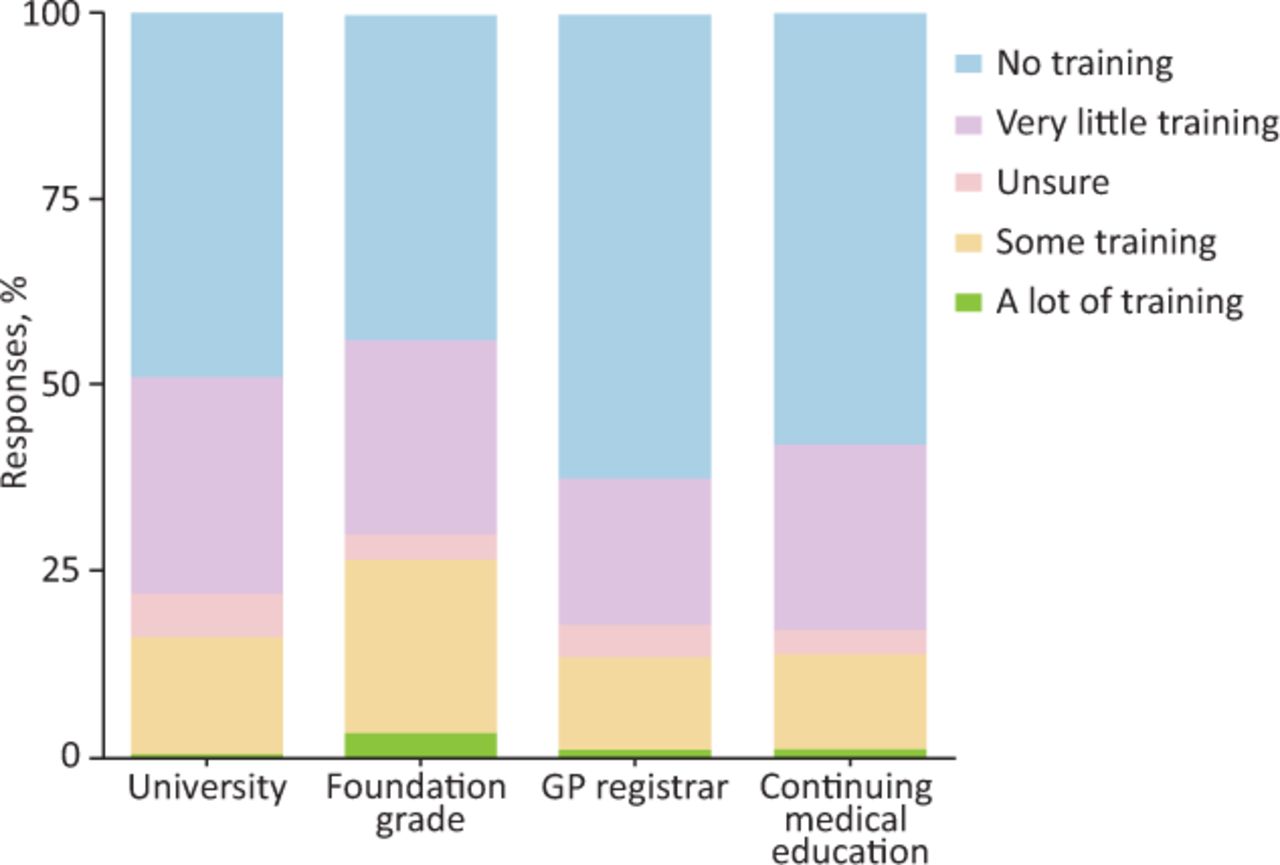
Respondents reported a lack of training in perioperative medicine as a major barrier to GP-led preoperative optimisation, with just 12% of GPs reporting adequate training to deliver preoperative optimisation. Training in perioperative medicine was infrequent at all career stages, with most training undertaken at foundation level and the least training undertaken as GP registrars (Fig 3).
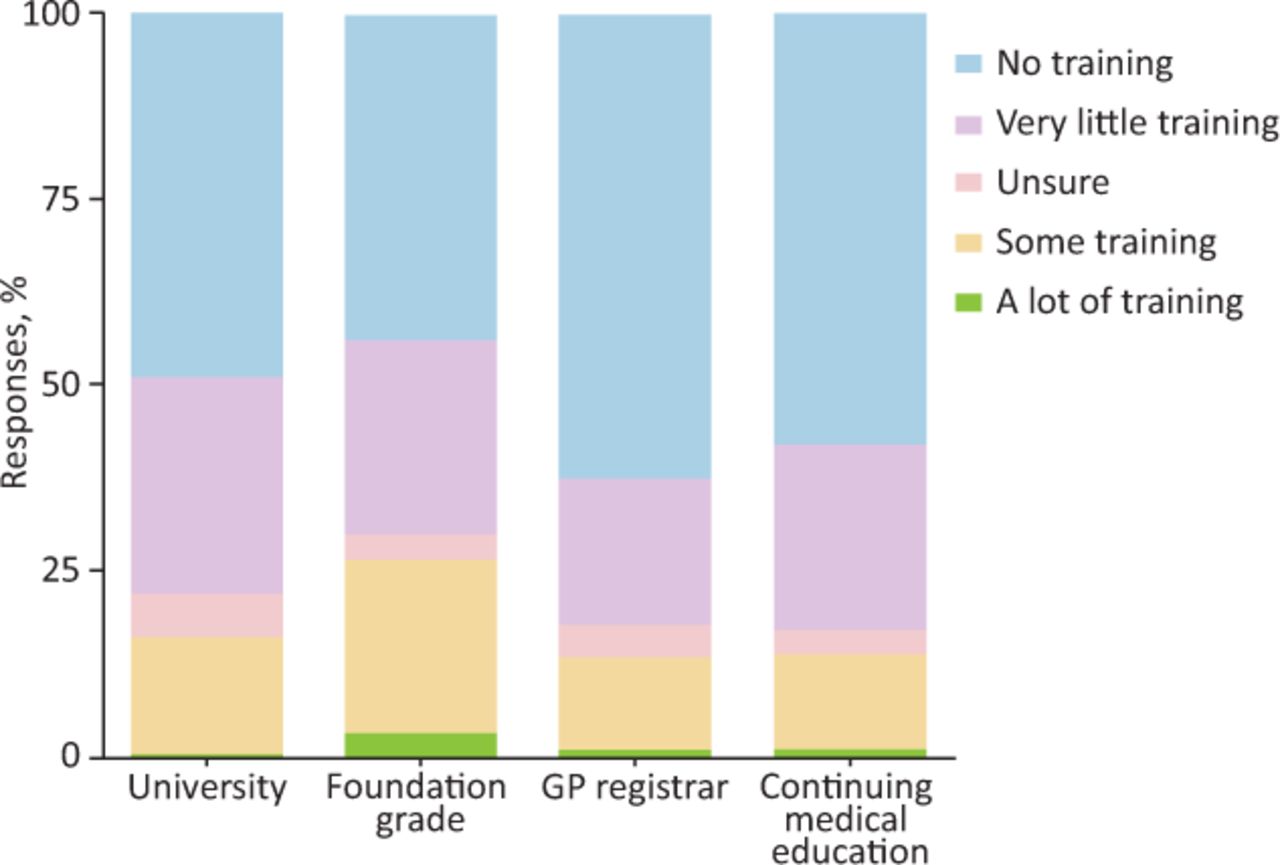
Perioperative medicine training at different stages of the general practitioner career span. GP = general practitioner.
Enablers and barriers
Key enablers and barriers to GP-led preoperative optimisation were described and grouped according to themes in Table 1.
Key enablers and barriers to general practitioner-led preoperative optimisation
Discussion
This is the first survey to explore the attitudes, beliefs and behaviours of GPs in England regarding perioperative medicine for older people, and to describe enablers and barriers to GP-based preoperative optimisation of older people undergoing surgery. The results showed that, although GPs overwhelmingly agree that preoperative optimisation of older patients can improve postoperative outcomes, there are significant cross-boundary clinical, process-related and professional barriers to implementing preoperative optimisation based in primary care. The COVID-19 pandemic has demonstrated how traditional barriers to innovative ways of working can be rapidly overcome. As health services adapt to the ‘new normal’, the opportunity to collaborate and integrate across the surgical pathway, from contemplation of surgery through to recovery, should be embraced by primary and secondary care providers.
It is widely acknowledged that the surgical population is ageing faster than the general population and surgical specialties are managing increasingly higher numbers of older, multimorbid patients.1,21 The role of primary care physicians in preoperative optimisation of longer-term conditions is frequently discussed given the contribution of such conditions to the perioperative risk profile in older patients undergoing surgery.22 Key potential advantages of GP-led optimisation include continuity in chronic disease management, GP expertise in empowering patient self-care and maximal use of lead time prior to surgery for time-sensitive optimisation.22,23
However, the results of this survey illustrate the infrequency with which GPs refer older people to surgical specialties and the fact that this patient group represents a relatively small proportion of the vast primary care workload. Involvement of GPs in certain surgical pathways is likely reduced through direct surgical referrals from screening programmes (such as the national abdominal aortic aneurysm screening programme) and specialist community services (such as musculoskeletal pathways) that may bypass referral by GPs. Thus, managing the preoperative period can be an infrequent event for GPs and represents a small contributor to the daily workload in primary care. This may pose a limitation to quality improvement and process change, as both rely on regular exposure to a given event, to facilitate rapid feedback and change mechanisms.24
Perhaps, related to this low volume of exposure, training in perioperative medicine is relatively lacking throughout a career in general practice. Respondents reported feeling inadequately trained to provide preoperative medical optimisation for older patients, and believed a lack of knowledge was a barrier to engaging in shared decision making regarding the risks, benefits and alternatives to pursuing surgical treatment. Although perioperative medicine training programmes are emerging across the UK, these are targeting trainees from surgical, anaesthetic and general medicine backgrounds, with no targeted training opportunities for GP trainees.13,25–28 Furthermore, respondents reported minimal day-to-day interaction with perioperative medicine services and a lack of awareness of available services and the activities undertaken by such services. There is, however, geographical disparity in these findings, suggesting that there is an opportunity to reduce national variation. In addition, as virtual working becomes more commonplace following the COVID-19 pandemic, earlier involvement of GPs in perioperative optimisation may occur, thus increasing the opportunity for training and for collaborative care.
Finally, this survey revealed persistent professional barriers to GP-based preoperative optimisation. Respondents reported feeling that their assessment and evaluation of the patient was not valued by the secondary care team. Fragmentation between primary and secondary care may have resulted in professional silos, with less robust relationships and less effective communication between healthcare settings. As such, shared interprofessional learning and relationship-building may be a key step in delivering integrated healthcare, mindful of a multimorbid population where acute admissions punctuate a patient journey shaped by long-term conditions. A good example of this, the Centre for Perioperative Care (CPOC) is a newly established cross-specialty organisation, with representation from all relevant colleges. CPOC aims to promote, advance and develop perioperative care through collaborative working.17 Such an approach with representation from the Royal College of General Practitioners is critical to address the challenges and embrace the opportunities described through this survey.
Study limitations
This study provides new knowledge regarding the role for GPs in perioperative care. A better understanding of the attitudes, beliefs and behaviours of GPs, and the barriers and enablers to GP-based preoperative optimisation can be used to develop collaborative integrated perioperative pathways. GPs were surveyed across all regions of England which allows a country-wide perspective of the challenges faced by GPs. However, this study is inherently limited as any survey of a large and heterogeneous group of clinicians, and should be interpreted as a first step to guiding further qualitative research and quality improvement initiatives. GP response rates to surveys are typically lower than those from the general medical professional population, with the overall response rate to this survey being consistent with other published surveys in primary care.29,30 The relatively small number of respondents (231) and variable regional response rate limits examination of differences between GPs’ experience across regions. Of the five regions of England, 53% of responses were from clinicians in London, thus other regions were less well represented. There is a possibility of response bias with respondents to the survey more likely to have an interest in, or experience of perioperative medicine services. Ambiguity of respondent interpretation of survey questions must be considered, although this was mitigated through piloting among GPs and validation with a group of expert raters.
Additionally, while this work focused on interprofessional factors, future work would benefit from patient and public representation to ensure that surgical pathways are patient-centred.
Conclusion
GP-based preoperative optimisation of older people could benefit patients and the health service, in line with the principles of the NHS Long Term Plan. Encouragingly, this survey has shown that GPs agree that preoperative optimisation can improve postoperative outcomes for older people, and that they have a role in identifying and managing modifiable risk factors. Future work should focus on interprofessional education, cross-sector training opportunities, relationship-building and clear role delineation in order to deliver quality integrated perioperative care for older people having surgery.
Supplementary material
Additional supplementary material may be found in the online version of this article at www.rcpjournals.org/clinmedicine:
S1 – Perioperative care of older people having surgery survey.
S2 – Professions of stakeholders interviewed in the development of the GP survey.
S3 – All free-text responses to questions with the option for a free-text entry.
- © Royal College of Physicians 2021. All rights reserved.
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.