
ABSTRACT
There is increasing recognition of the need for collaboration between oncologists, acute physicians and specialists to improve the quality of care and outcomes of acutely unwell patients with cancer. At The Christie, a tertiary oncology hospital, a model has been developed to deliver acute medical and specialty support services. This delivers, among many things, a consultant-led acute medical ward round on weekdays. There has been a significant increase in the number of patients admitted to the oncology assessment unit (OAU) since its introduction, in part due to an increased number of direct discharges from the unit. Collaborative working between oncologists and acute physicians with a shared vision for high-quality care for patients has ensured that this change has been implemented smoothly. This has included development of patient flow models to optimise bed usage, so that a higher number of patients can access these specialist services.
Introduction
In the UK, approximately 325,000 new cases of cancer are diagnosed each year, contributing to around 28% of UK deaths.1 In the UK, patients with cancer account for around 15% of all acute inpatient stays and these consume around half of the spending on patients with cancer.2,3
Cancer care has become increasingly specialised and advances in therapy have resulted in a larger number of patients receiving care as an outpatient. As a result of these advances in care and the increasing number of patients receiving cancer therapies, there has been a significant increase in the number of patients presenting with cancer-related emergencies.2,4
In the UK, there have been two strategies adopted to improve the care of acutely unwell cancer patients – the development of specialist admission units in tertiary cancer units and the evolution of acute oncology services to support patients admitted to non-cancer hospitals.5,6 There is an increasing recognition of the need for collaboration between oncologists, acute physicians and specialists to improve the quality of care and outcomes for patients with cancer.6,7
At The Christie, a tertiary oncology hospital in Manchester, a model has been developed to deliver acute medical and specialty support services in collaboration with a local university hospital – University Hospital of South Manchester.
Methodology
The Christie NHS Foundation Trust is a tertiary oncology hospital and is one of the largest in Europe. It has 250 beds, including a 21-bed oncology assessment unit (OAU) and a 7-bed critical care unit. It is the lead cancer centre for patients in Greater Manchester and Cheshire but provides many national services.
The OAU currently admits around 350 patients a month. Patients are admitted to the unit through three main routes:
via a hotline – all patients receiving treatment at The Christie have access to a specialist helpline, which is run by nurse specialists. Patients are advised that if they develop symptoms, such as fever post chemotherapy, to contact the hotline for advice and assessment. If they are triaged as having a condition related to the cancer or its treatment, they are admitted to the admissions unit for assessment. This is often facilitated by the hotline contacting an ambulance to transfer the patient to the hospital.
via inpatient clinics/chemotherapy/radiotherapy
via referrals from other hospitals – patients under the care of The Christie or with an acute cancer presentation at another hospital who need urgent chemotherapy/specialist inpatient care are referred to The Christie and transferred to the admissions unit.
The model commenced service delivery in October 2014. It delivers a consultant-led acute medical ward round on weekdays. Acute physicians work closely and collaboratively with oncology colleagues. Acute physicians perform a daily review on patients on the OAU, conduct a joint post-take ward round with a consultant medical oncologist and perform real-time consultant reviews of patients admitted to the OAU during the day. The initial cost of the delivery of the model is approximately £240,000 a year, including administration and trust-related expenditure.
The OAU admits patients with a variety of acute oncology presentations. There is a weekly cardio-oncology ward round with a visiting cardiology consultant. Alongside developing services on the OAU, there is an in-reach service for acutely unwell oncological and surgical ward patients. This delivers:
high-quality and safe patient care with immediate response to sick patients
guidelines and quality initiatives in acute medical care – such as the management of acute kidney injury and sepsis; this incorporates a nurse-led protocol for the administration of the first dose of intravenous antibiotics in patients with suspected sepsis post chemotherapy. This innovation has resulted in 96.4% of this cohort receiving intravenous antibiotic within 1 hour of arrival on the OAU8
education of junior doctors, students and multiprofessional colleagues in the management of acute cancer complications.
Junior doctors have formal teaching and direct supervision from acute physicians while on the OAU. Medical student projects and placements in this key area are supervised by acute physicians and other specialty doctors have attended the OAU for further clinical experience.
Outcomes
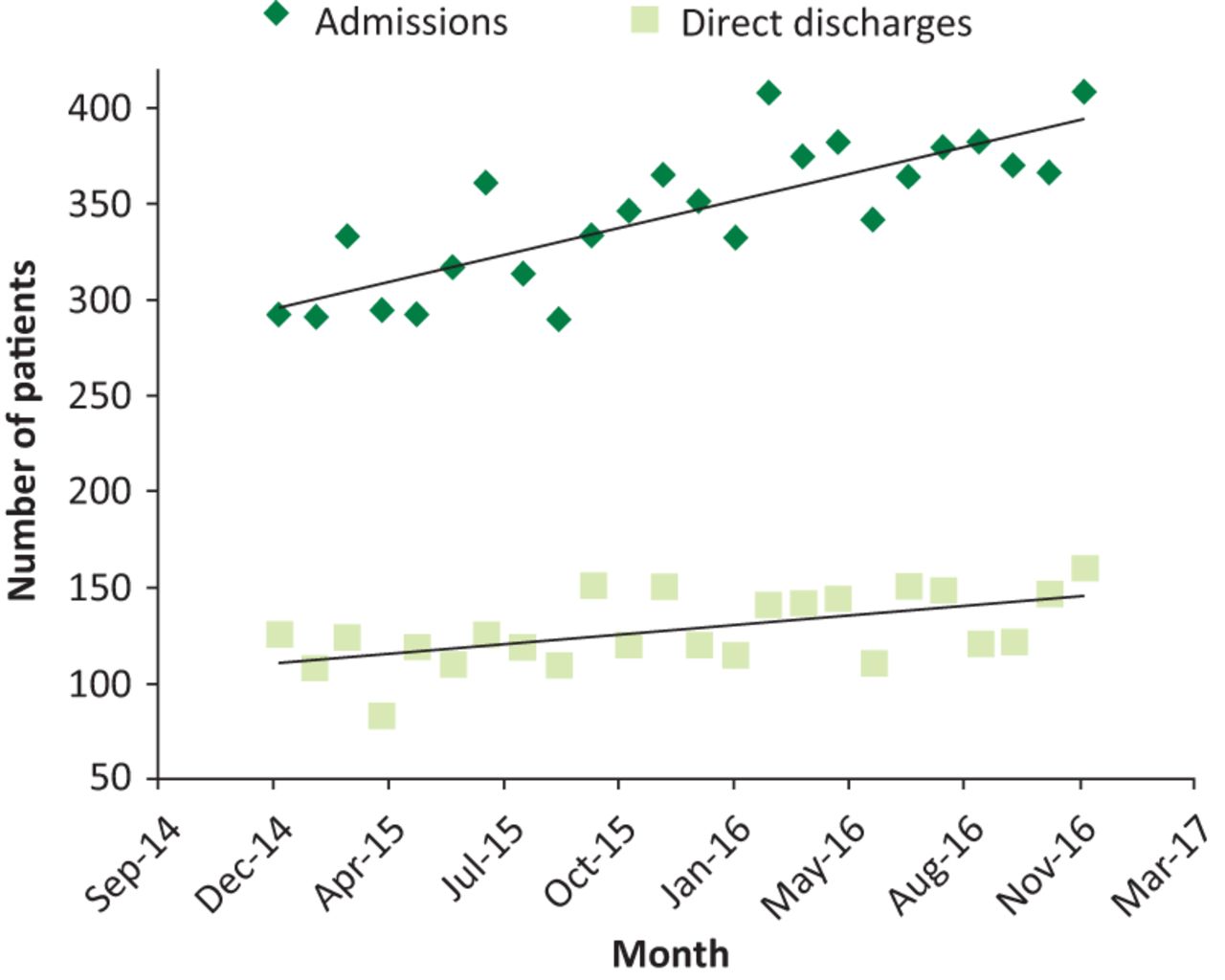
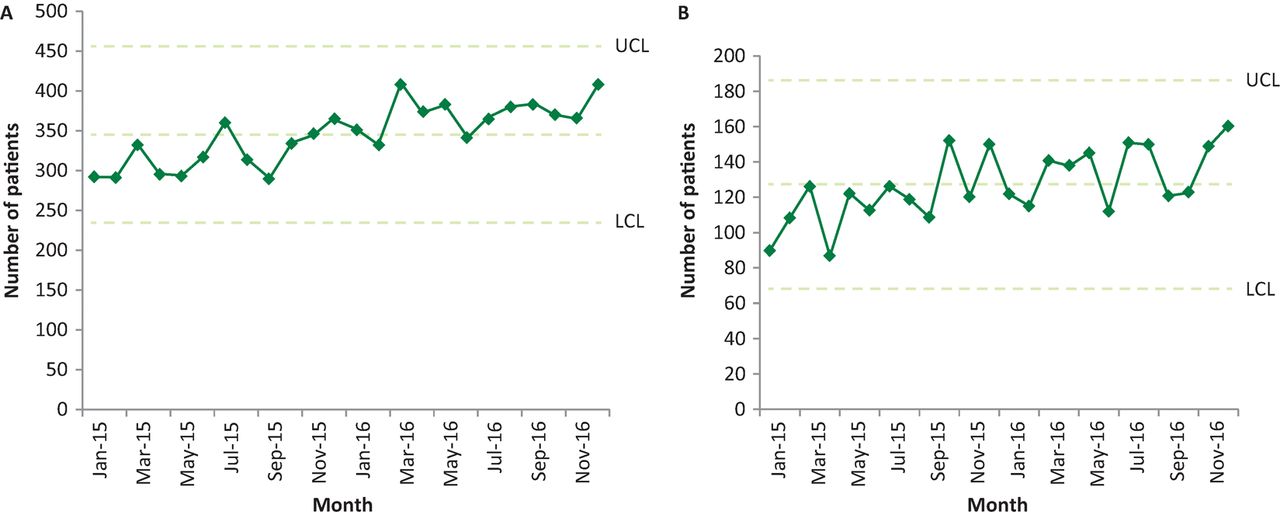
There has been a significant increase in the number of patients admitted to the OAU since the introduction of the model in part due to an increased number of direct discharges from the unit (Fig 1). Fig 2 shows statistical process charts demonstrating the effect of the new model. In the past, patients have regularly been diverted to local hospitals because of a lack of bed availability. With the new care model in place, there has been a 50% improvement in the last 12 months in the ability to admit patients to The Christie through the patient hotline. This can help mitigate the potential pitfalls, and the impact on patient experience, of remote shared care alongside reducing pressure on emergency and acute medical services at local hospitals.
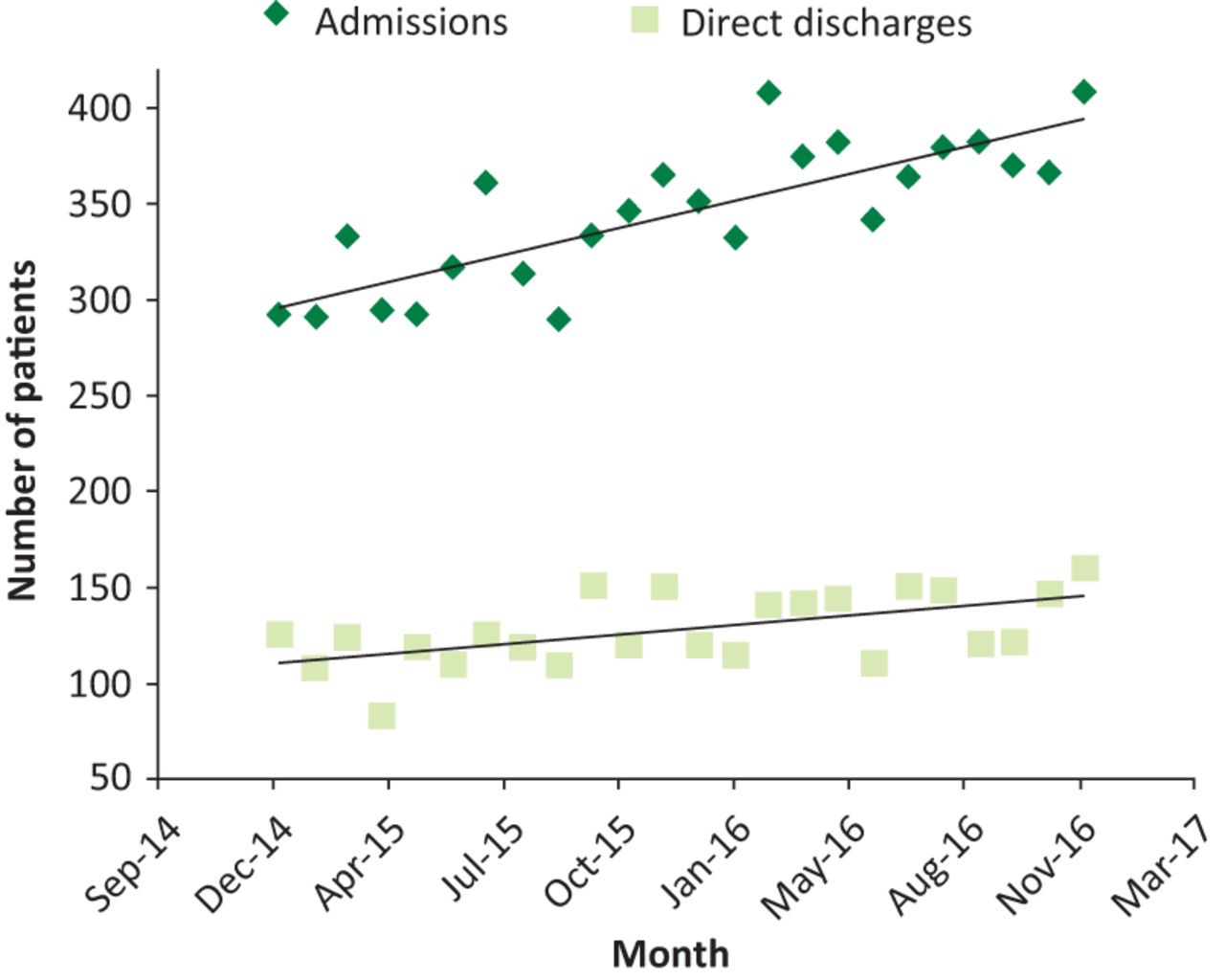
Trends for admissions to, and direct discharges from, the oncology assessment unit since commencement of acute medical and specialty support at The Christie.
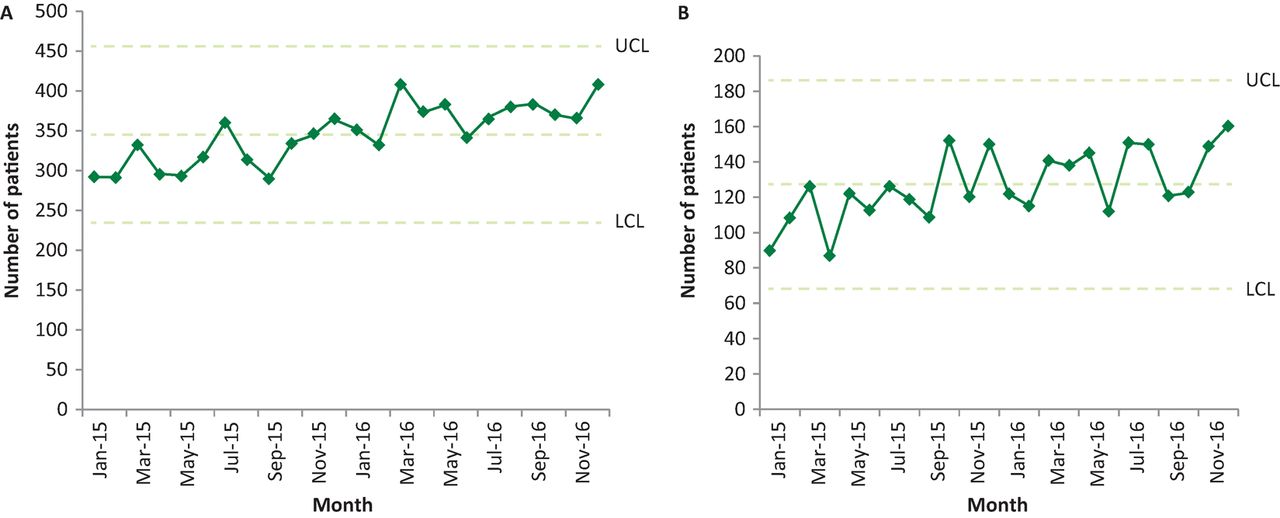
Statistical process charts for admissions (A) and direct discharges (B) to the oncology assessment unit. LCL = lower control limit; UCL = upper control limit
Ambulatory care clinics have been initiated in collaboration with supportive care colleagues; these commenced in January 2017. These clinics, known as Enhanced Supportive Care 2 (ESC 2), are the first of their kind in Europe and are facilitating ambulatory management of patients with low-risk febrile neutropenia,9 acute pain and chemotherapy-induced nausea and vomiting alongside early access to specialists in supportive care in cancer. This is a further innovation that is enabling a greater number of patients to have their cancer complications managed at their cancer treating centre.
The model has developed collaborative working with other colleagues, including respiratory, gastroenterology and infectious disease, developing rapid access to services, such as endoscopy and endoscopic retrograde cholangio-pancreatography. Eight sessions of echocardiography are provided per week. The majority of scans performed are for chemotherapy screening but a slot a day is reserved for emergency inpatient scans for patients with acute presentations such as suspected pericardial effusion, massive pulmonary embolism and myocarditis. This earlier access to specialist advice and interventions is another key aspect of improving flow through the hospital and facilitating increased admissions to the OAU.
Conclusions and next steps
Collaborative working between oncologists and acute physicians with a shared vision for high-quality care for patients has ensured that this change has been implemented smoothly. This has included the development of patient flow models to optimise bed usage so that a higher number of patients can access these specialist services.
The innovative model is improving the quality of acute medical care for inpatients at The Christie. It is already gaining a reputation of delivering high standard, specialist and quality care for this cohort of patients.
Teamworking is the essence of acute care. This multidisciplinary, multispeciality working with continued adaptation to the demands of the service means this model is likely to become a flagship and standard setting model for the delivery of acute cancer care.
The short- and long-term plans largely involve expanding the service to 7 days and increasing the ESC 2 clinics. The main barrier to achieving these plans is the availability of senior clinical staff with appropriate skills to implement the changes. This reflects the national challenge of recruitment and retention of acute medical specialties.
Conflicts of interest
The authors have no conflicts of interest to declare.
Author contributions
All authors contributed to development of the service level agreement and final manuscript.
- © Royal College of Physicians 2017. All rights reserved.








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.