
Acute on chronic liver failure (ACLF) is a common clinical entity, often complicated by multiple organ failure and associated with a poor prognosis. Clinical features include jaundice, hepatic encephalopathy (HE) and the hepatorenal syndrome (HRS). Common precipitants include variceal haemorrhage, sepsis, alcohol and drugs. Prompt resuscitation is key. Early pharmacological and endoscopic therapy influence outcome in variceal haemorrhage and empirical antibiotics should be given. Sepsis may present in an occult manner and spontaneous bacterial peritonitis (SBP) should be actively excluded. Patients with SBP are at higher risk of developing HRS. An early specialist opinion should be sought.
Acute liver failure (ALF) is also associated with multiple organ failure and a poor prognosis. Liver transplantation remains the only current effective treatment, therefore early identification of ALF and liaison with the local liver transplantation unit is crucial. Patients should be assessed and key parameters monitored regularly, in particular prothrombin time (PT), bilirubin (BR), creatinine, pH and presence of encephalopathy as these have prognostic relevance.
A comprehensive discussion of the pathophysiology and management of ALF and ACLF is outside the scope of this article. This review is intended to provide an overview of key aspects of initial assessment and management of patients with liver failure.
Acute on chronic liver failure
Definition
ACLF is defined as an acute deterioration in liver function over a period of 2–4 weeks usually associated with a precipitating event, leading to a severe deterioration in clinical status with jaundice and hepatic encephalopathy (HE) and/or HRS with a high SOFA/APACHE score.1
Epidemiology
The UK incidence of cirrhosis is approximately 17 per 100,000 (prevalence 76 per 100,000) in adults over 25 years, although the exact figures are unknown. This represents an increase over a 10-year period of 45% and 68%, respectively. Mortality from cirrhosis has increased by over 400% since 1970. More than 80% of liver-related deaths in the UK are due to cirrhosis secondary to alcohol.
Background
Cirrhosis
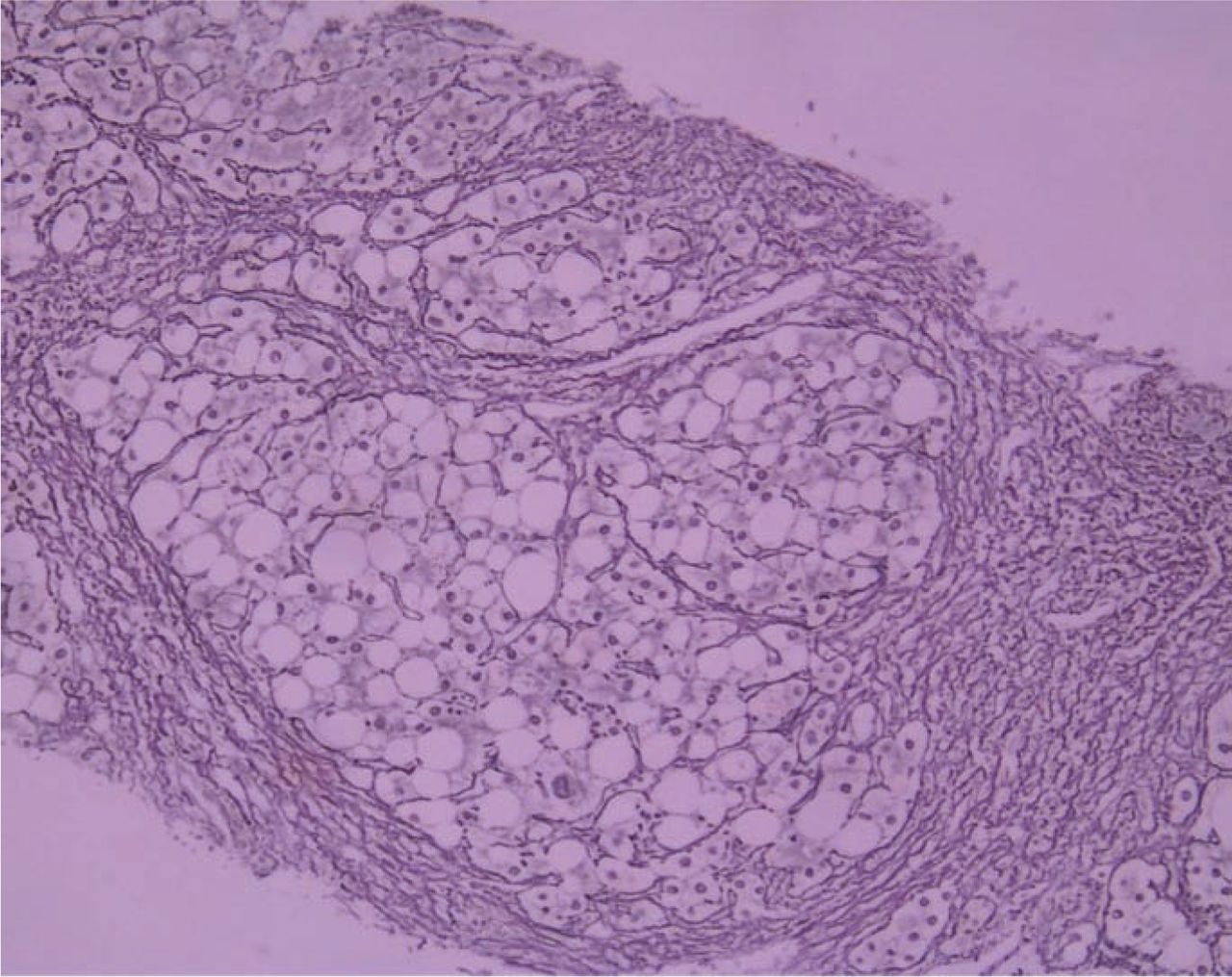
The gold standard diagnosis of cirrhosis is histological. It is characterised by extensive fibrosis, resulting in architectural distortion with nodule formation (Fig 1), leading to portal hypertension and end-stage liver disease (ESLD). The epidemic of heavy alcohol consumption in the UK is reflected in the rising rates of alcoholic liver disease and is the leading cause of cirrhosis in the UK. Other aetiologies include viral hepatitis, autoimmune liver diseases, metabolic liver diseases and alpha-1 antitrypsin deficiency (Table 1).
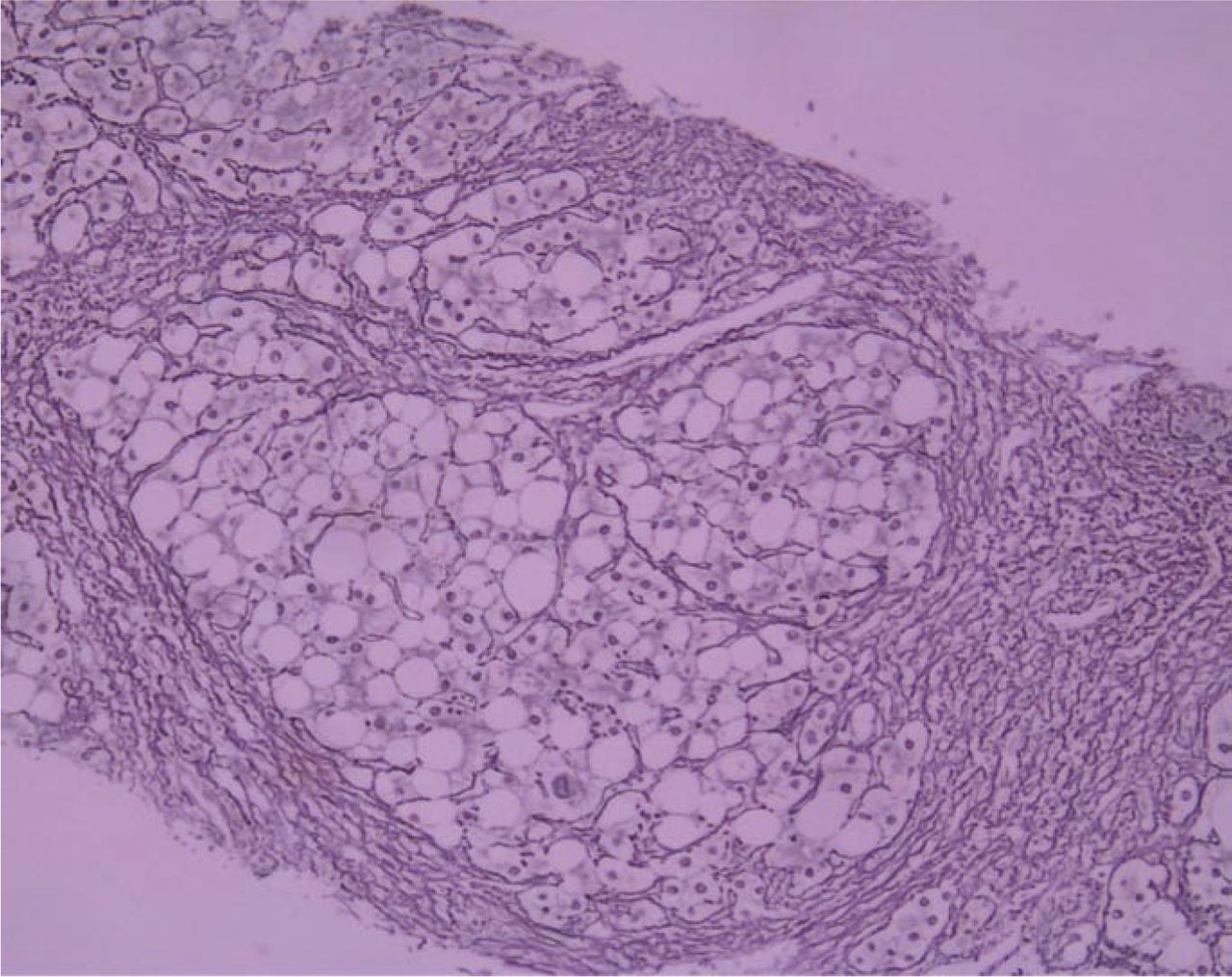
Cirrhosis.
Causes of cirrhosis.
Functional status can be expressed by the Child-Turcotte-Pugh or the UK Model for End-Stage Liver Disease (UK ELD) scoring systems, both of which have prognostic relevance. Patients with cirrhosis may develop liver failure either as a function of chronic disease progression or secondary to an acute precipitant (ACLF). The latter may be due to variceal bleeding, sepsis, ischaemia or direct liver injury relating to alcohol, hepatotoxic drugs or viral hepatitis.
Pathophysiological mechanisms
The pathophysiological mechanisms of ACLF are incompletely understood. The natural history of chronic liver disease involves the development of portal hypertension, ascites and progression to HRS. Against this natural history an acute insult may result in ACLF. Inflammation seems to play a key role in pathogenesis.
Oesophageal varies. These develop as a consequence of portal hypertension. A hepatic venous pressure gradient (HVPG) greater than 12 mmHg is strongly associated with a risk of variceal bleeding. Other contributory factors include variceal grade, severity of liver disease and coagulation status.
Cirrhotic ascites. The formation of cirrhotic ascites occurs due to portal hypertension and salt and fluid retention resulting from stimulation of the renin-angiotensin system. The contribution from the reduced oncotic pressure of hypoalbuminaemia is much less significant.
Hepatorenal syndrome is a functional disorder in which renal failure (serum creatinine >133 mmol/l) develops in the context of advanced liver failure, ascites and structurally normal kidneys. While an oversimplification, Fig 2 demonstrates the sequence of pathophysiological mechanisms which result in activation of vasoconstrictor systems and renal vasoconstriction. HRS is associated with a poor prognosis and represents the later pathophysiological stages in ESLD. HRS may be classified into two forms:
type I HRS occurs with a 50% reduction in creatinine clearance to a <20 ml/min within two weeks and is associated with a worse prognosis
type II HRS has a more chronic onset.

Pathophysiology of hepatorenal syndrome.
Hepatic encephalopathy. Hyperammonaemia and inflammation are implicated in the development of HE in ACLF. Certainly, ammonia has been shown to induce neutrophil dysfunction in animal models.2
Clinical presentation
Clinical features of cirrhosis include the classical peripheral stigmata, jaundice, organomegaly, ascites and encephal-opathy. Patients with ACLF may present in a number of ways, including with clinical features relating to portal hypertension, hepatic synthetic dysfunction and a systemic inflammatory response syndrome.
Variceal haemorrhage
Variceal bleeding may present with large or initially small volume haematemesis, melaena or rectal bleeding and often significant haemodynamic compromise. Patients with known varices may not mount a tachycardic response if established on beta-blockers. Care should be taken to assess for evidence of aspiration pneumonia.
Sepsis
Patients with cirrhosis are immunocompromised and sepsis may present in an occult manner. There should be a low threshold for considering sepsis, in particular SBP. Up to 50% of cases of SBP are asymptomatic and may be complicated by HRS.
Encephalopathy
Encephalopathy may be low grade at presentation and manifest only as mild confusion, reversed sleep cycle or detectable clinically as asterixis. High-grade encephalopathy presents with a Glasgow Coma Scale of 8 or below. Acute precipitants such as sepsis, variceal bleeding, constipation and electrolyte disturbance should be excluded. Care must be taken to avoid sedating medication. Patients with cirrhosis often have an associated coagulopathy and a potential differential diagnosis of intracerebral bleed should be considered.
Other precipitants of ACLF include alcohol and drugs. Common hepatotoxic agents include non-steroidal anti-inflammatory drugs (NSAIDs) and antibiotics.
Investigations
Laboratory investigations
The chief prognostic laboratory parameters are PT, BR, creatinine and albumin as these are markers of hepatic synthetic function. Transaminases, gGT and alkaline phosphatase may provide information about the nature of liver injury. Alcoholic hepatitis often presents with an aspartate aminotransferase to alanine aminotransferase ratio above 2. A full blood count may demonstrate thrombocytopenia and leukopenia, features of hypersplenism and thus portal hypertension. Blood cultures should be taken as the risk of sepsis is high in these patients. If the patient is presenting de novo, a non-invasive liver screen should be requested (Table 2). Additional investigations relevant to ALF are shown in Table 3.
Non-invasive liver screen for causes of cirrhosis.
Additional investigations in acute liver failure.
Diagnostic ascitic tap
Patients with ACLF and ascites should undergo a diagnostic ascitic tap and the fluid sent for urgent microscopy, culture and biochemical analysis. Fluid should be inoculated into blood culture bottles to increase diagnostic yield. A polymorphonuclear cell count greater than 250 cells/mm3 is diagnostic of SBP. The most commonly isolated organism is a Gram-negative single enteral bacterial species. Mixed growth is suggestive of perforation.
Radiological investigations
An abdominal ultrasound with Dopplers plays an important role in initial evaluation of these patients. Imaging can be helpful to confirm features of chronic liver disease. Assessment of hepatic and portal vein patency is important to exclude an acute Budd-Chiari syndrome and portal vein thrombosis.
Management of variceal bleeding
Resuscitation
Patients with variceal haemorrhage should be managed in a high dependency environment. Prompt resuscitation is key. Airway management is vital as the aspiration risk is often high and significantly affects outcome. Large bore and central access should be established. Volume resuscitation with fluid, blood and blood product support is a priority. The aim should be to transfuse to a haemoglobin of 10 g/dl and correct coagulopathy. Intravenous vitamin K should also be given, but is unlikely to influence the coagulation status in the initial period.
Pharmacological therapy
Vasoactive drugs which cause splanchnic vasoconstriction, and thus reduce portal pressures, play a key role in stabilising patients with variceal bleeding. Drugs currently available include terlipressin, somatostatin and octreotide. Terlipressin, a derivative of vasopressin, is highly effective. Clinical studies have shown that terlipressin achieves control of active variceal bleeding in 75–80% of cases at 48 hours without endoscopic therapy3 and is the only drug shown to improve survival.4 It is also thought to have a renoprotective role. Terlipressin is associated with a small risk of coronary and peripheral arterial vasospasm and arrhythmias. For this reason, an ECG should be performed prior to commencing therapy and patients should undergo cardiac monitoring. Vasoactive drug therapy should be continued for 2–5 days.
Broad-spectrum antibiotics should also be given to reduce the risk of sepsis which has been identified as an independent prognostic factor of failure to control bleeding or early rebleeding.5,6
Key Points

Endoscopy
Any cirrhotic patient with symptoms of an upper gastrointestinal (GI) bleed (however stable on presentation) should undergo an early upper GI endoscopy. Endoscopic options include variceal ligation (‘banding’) and sclerotherapy for bleeding oesophageal varices. Variceal ligation is superior to sclerotherapy with regard to safety and efficacy when used in combination with vasoactive drugs.7 Gastric varices are a somewhat greater endoscopic challenge and options include histoacryl ‘glue’ or thrombin injection. Patients in whom haemostasis is not achieved by endoscopic means require Sengstaken tube placement and consideration for a transjugular intrahepatic portosystemic stent shunt (TIPSS) placement.
Transjugular intrahepatic portosystemic stent shunt
TIPSS insertion is used as salvage therapy for variceal bleeding refractory to endoscopic therapy. By shunting blood from the portal to the hepatic vein the HVPG is reduced and thus the risk of variceal bleeding. A transjugular approach is used and the hepatic vein cannulated. The portal vein is then punctured and a shunt deployed from the hepatic to the portal vein. If the resultant HVPG is less than 12 mmHg, the risk of variceal bleeding is significantly diminished. Once portal access is established, variceal coil embolisation can be achieved. TIPSS insertion results in haemostasis in 90% of these endoscopic refractory patients. TIPSS-related complications include encephalopathy in up to 30% of patients, pulmonary hypertension and worsening liver function. Patients presenting with variceal haemorrhage and TIPSS in situ should undergo Doppler studies to assess shunt patency.
Surgery
The need for surgery is rare due to the success of other therapies. Surgical portosystemic shunts are associated with a high risk of encephalopathy and mortality. Patients with more advanced disease may be more suitable for transplantation.
Ascites (including spontaneous bacterial peritonitis)
Patients with features of ACLF or pyrexia in the context of ascites require a diagnostic ascitic tap. Management includes broad-spectrum antibiotics such as a third-generation cephalosporin. In 30% of cases SBP will be complicated by renal impairment, although studies have demonstrated this can be reduced with administration of salt-poor human albumin solution (HAS). The regimen used in the original studies was 1.5 g/kg of albumin on day 1 and 1 g/kg on day 38 and can be given to patients with a rising creatinine or established renal impairment. Therapeutic paracentesis should be deferred in an acute presentation of SBP, again due to the risk of renal failure.
Hepatorenal syndrome
Patients with HRS have a significant risk of mortality. In the cirrhotic patient, serum creatinine underestimates the degree of renal impairment and renal failure should be managed with particular care. HRS should be differentiated from coincident intrinsic renal disease. Patients with HRS have features of salt and fluid overload and are hyponatraemic. They should be rendered euvolaemic and, once this is achieved, may require low-dose terlipressin to maintain an adequate urine output. HRS commonly complicates SBP but, as previously discussed, HAS replacement can reduce the risk. Pentoxifylline can play a role in patients with alcoholic hepatitis complicated by HRS.9
Encephalopathy
As discussed above, airway protection is a priority. Precipitants such as sepsis, variceal haemorrhage, sedating drugs, constipation, alcohol and electrolyte disturbance should be addressed individually as appropriate.
Specific therapies
Therapies directed at specific hepatological insults precipitating ACLF should be initiated under specialist supervision and rarely play a role in the immediate management of these patients. Alcoholic hepatitis is an important cause of ACLF. Maddrey's discriminant factor (Box 1) or Glasgow alcoholic hepatitis score can be calculated to give an estimate of the potential benefit of steroid therapy.
Maddrey's discriminant factor (DF).

Histological confirmation is often required and the risk of sepsis with these therapies should be considered. Steroids can also play a role in a flare of autoimmune liver disease. ACLF due to hepatitis B can be managed with low-dose lamivudine but antiviral therapy plays no role in the acute setting in patients with hepatitis C.
General therapies
Nutritional support is key and early involvement of a dietician crucial. Patients with an alcohol history should be prescribed pabrinex, oral thiamine and B vitamins, and intravenous vitamin K. Glycaemic control should be monitored – of particular importance in alcoholic and diabetic patients, but a failure of gluconeogenesis is a feature of end-stage liver failure.
Future therapies
Artificial and bioartificial liver support systems are a key area of research interest, particularly in the context of ACLF. Data to date are limited and further studies required before these systems can be routinely used.
Prognosis
Mortality from a first-presentation variceal bleed is about 50% and heavily influenced by the severity of underlying liver disease. Child-Pugh class is a good predictor of survival, with one-year mortality rates from subsequent variceal haemorrhage for class A, B and C of 5%, 25% and 50%, respectively. Patients with SBP have an inhospital mortality of 20%. Survival is highly influenced by the presence or absence of HRS. Once patients develop SBP, cumulative recurrence rates are 70% with a median survival of nine months. Patients with type I HRS have a prognosis of less than two weeks, with fewer than 10% surviving their hospital admission.
Acute liver failure
Definition
ALF is characterised by jaundice, coagulopathy and encephalopathy in patients with previously normal liver function. The chronicity to onset of jaundice and/or encephalopathy is used to classify patients into the following groups:
hyperacute liver failure: less than 7 days
ALF: 7–28 days
subacute liver failure (SLF): 5–12 weeks.
Background
The main cause of ALF is viral- or drug-induced hepatitis. Non-prescription medication such as paracetamol, NSAIDs and herbal medicines are important potential aetiological factors. Wilson's disease, autoimmune and ischaemic hepatitis may also cause ALF.
Clinical presentation
The time interval to onset of liver failure is important. Patients with ALF and hyperacute liver failure are more likely to present with HE and haemodynamic compromise. Patients with SLF are less likely to develop encephalopathy and may even have ascites. HE may manifest only with subtle neuropsychiatric disturbance, but early detection and referral are key. Rarely will there be clinical features of underlying aetiology. A thorough history, particularly in reference to use of prescribed and non-prescribed medication, is important. Kayser-Fleisher rings are an important finding and pathognomonic of Wilson's disease. It is clearly important to ascertain if there are any clinical features which may suggest chronic liver disease. The possibility of acute fatty liver of pregnancy in women in the third trimester of pregnancy should be considered because it is thought to be part of a spectrum with the HELLP syndrome and pre-eclampsia.
Investigations
Initial investigations will include routine laboratory tests. The most important of these are BR, PT and serum creatinine. pH is of particular prognostic importance in the context of paracetamol toxicity, yet is frequently omitted in routine assessment of these patients. A routine non-invasive liver screen should be processed early and the patient have urgent imaging of the liver and hepatic and portal vessels. A transjugular liver biopsy may be required. Patients with ALF should be discussed with a liver transplant unit, and investigations and clinical assessment continued at frequent intervals until recovery or transfer to a transplant unit.
Management
Patients with ALF should be managed in the context of a high dependency unit (HDU)/intensive therapy unit environment (full review of management in the latter is outside the scope of this article). Encephalopathy is a particular concern in these patients. Severe encephalopathy warrants intubation and appropriate supportive management. Intracranial pressure monitoring may be required. As with all critical care patients, attention should be given to optimising volume status although fluid type is not crucial. Noradrenaline may be used if circulatory support is required and adrenal insufficiency should be considered as a contributing factor. Empirical antibacterial and antifungal cover is often given and there should be a low threshold for considering N-acetylcysteine to cover the possibility of paracetamol toxicity. Care should be taken to correct electrolyte disturbances and achieve good glycaemic control. Good nutrition is important and gastric protection should be prescribed.
Criteria for referral
Referral to specialist centre in paracetamol hepatotoxicity
day 2: arterial pH<7.3, international normalised ratio (INR)>3, encephalopathy, Cr>200, hypoglycaemia
day 3: arterial pH<7.3, INR>4.5, encephalopathy, Cr>200
day 4: any rise in INR, encephalopathy, Cr>250.
King's College Hospital criteria for transplantation
Paracetamol overdose
pH<7.3, irrespective of degree of encephalopathy
PT>100 sec, serum creatinine >300 mmol/l if in grade III/IV encephalopathy.
Non-paracetamol
PT>100 sec regardless of degree of encephalopathy, or
any three of the following:
aetiology: non-A, non-B, idiosyncratic drug reactions, halothane hepatitis
age <10 or >40 years
interval from jaundice to encephalopathy >7 days
PT >50 sec
BR>300 mmol/l.
Prognosis
SLF is associated with a worse prognosis; patients with ALF and hyperacute liver failure have higher rates of spontaneous recovery. The King's College Hospital criteria reflect the adverse prognostic groups in this cohort of patients. Patients who satisfy these criteria have a survival of 10–15% without transplantation.
Summary
Patients with ALF or ACLF frequently develop multiple organ failure and should be managed by senior physicians in a high dependency or intensive care environment (Table 4).
Summary of the management of patients with acute on chronic liver failure (ACLF).
- © 2010 Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.