
Abstract
Intermediate care (IC) has been government policy for implementation in the UK for almost 10 years. It was hoped that it would help free up acute hospital resources. However, admission rates continue to rise and are rising fastest in those over the age of 75. Many different models of IC have been tried. Typically, outcomes are very similar to traditional hospital care and they tend to be met with high patient satisfaction. Yet there is no evidence that they reduce acute hospital use or that they are cost efficient. Maybe it is time to rethink our national strategy on this issue?
Introduction
Intermediate care (IC) is subject to a variety of definitions,1 but can be simply described as healthcare occurring somewhere between traditional primary (community) and secondary (hospital) care settings. There is, however, wide variation in the structure and function of services labelled as IC across the country.2 These services have been proposed as an alternative to standard acute hospital care for selected groups of patients. The benefit may be to free up some acute beds for patients requiring longer lengths of stay (sometimes referred to as ‘bed blockers'), for example for rehabilitation. This group is often considered to include many older people. The intention is that IC could meet the patients' needs to a similar standard as acute hospital care, but would have some other advantage to the healthcare system, for example be cheaper. Additionally there may be qualitative benefits to the individual patient, possibly as a result of providing care closer to the patient's home.3
In 2000 the UK government announced a plan to modernise the NHS, including creating 5,000 new beds in the IC sector and providing rapid response teams which, in combination with other steps, was hoped to reduce unnecessary hospital admissions by around 70,000 per year by 2004.4 Despite evidence that many of these changes have been developed as planned, the number of adults aged 75 years and over being admitted to acute hospitals in the UK continues to increase.5 In the year 1998/9 in England this figure was 2.22 million and has risen year on year to 3.31 million in 2007/8 (an increase of 49% – larger than any other age group).6 Increasing hospital usage is thought to be due to a steady growth in the number of patients living with long-term conditions in the UK, and these people are more likely to utilise healthcare services.7 This rise in demand without a proportionate rise in bed capacity has been met by a reduction in length of stay (Fig 1). A concern is that people may be discharged too soon from hospital, and there are data that readmission rates are increasing.8 One study has suggested that approximately 20–25% of patients admitted to elderly care wards with an acute illness are thought to have a need for post-acute rehabilitation once their condition is stable.9
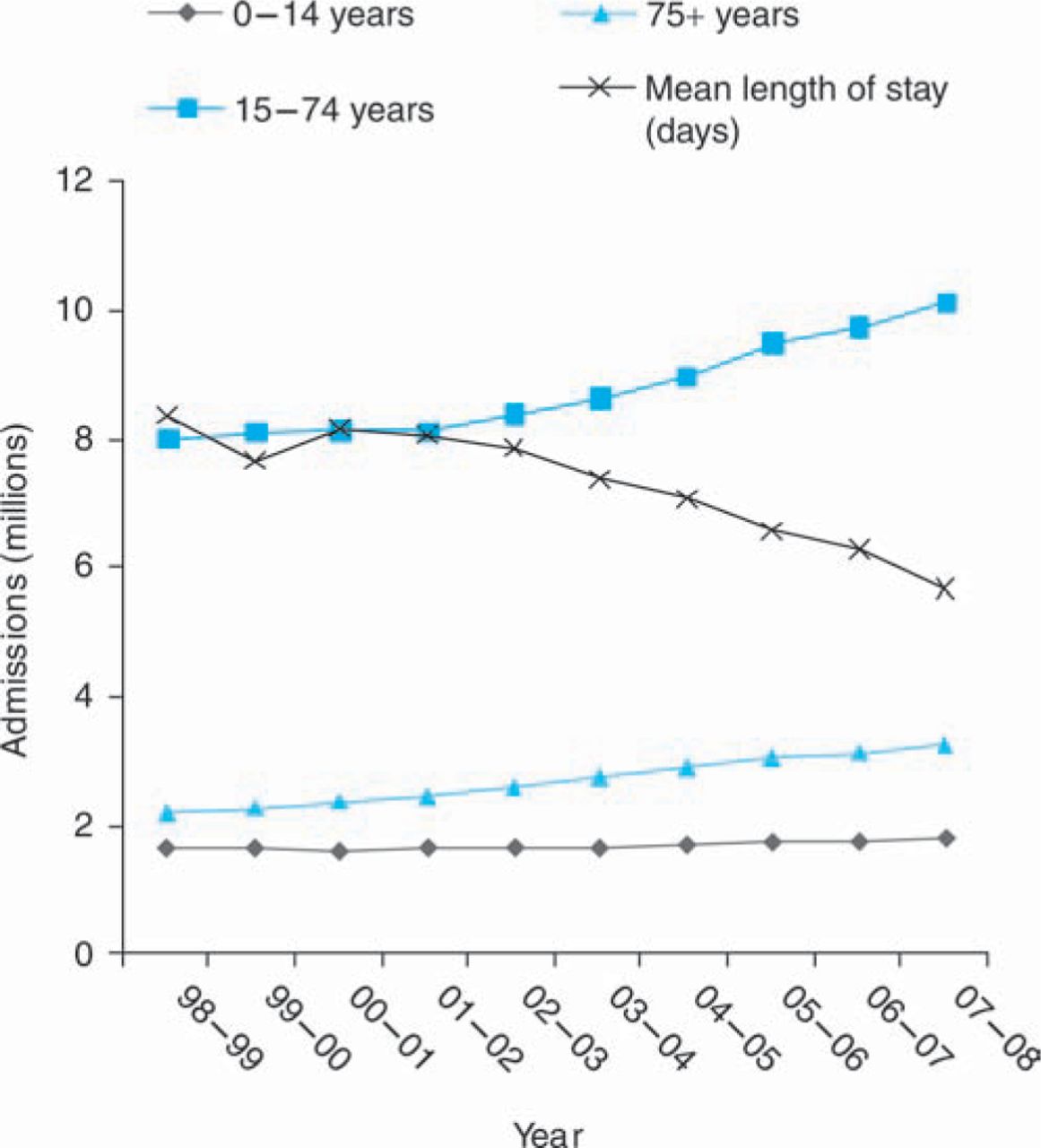
Change in hospital use over time in England.
The UK has now had almost a decade of implementation of IC policies. The aim of this paper is to review the available data regarding their impact on care services for older adults with a mix of medical conditions, ie not those for specific problems such as stroke or postoperative care. A Medline search was performed to identify relevant articles using the search terms ‘intermediate care’, ‘admission avoidance’, ‘case management’, ‘community hospital’, ‘rapid response team’, ‘nurse-led unit’, ‘supported discharge’, ‘early discharge’ and ‘hospital at home’. Other articles were obtained by searching relevant reference lists.
Admission avoidance
Hospital at Home
Hospital at Home (HaH) means the provision of healthcare within patients' own homes in a way similar to the services available within a hospital environment, ie in the absence of this service they would need to be admitted. Typically this would include nursing, physiotherapy, social work and occupational therapy staff input. Medical support may be provided either as outreach from the hospital or via the patient's own general practice. It has been used in both admission avoidance and early discharge schemes.
A recent Cochrane review identified 10 trials involving the use of an HaH scheme to avoid hospital admission.10 Overall, the authors concluded that there was no evidence to suggest that outcomes were different between the two groups. Just three of the included trials recruited older patients with a mix of acute medical conditions, the others were designed around specific diagnoses (mainly stroke and chronic obstructive pulmonary disease).
In the first of these trials, 197 older adults (median age 84 years) were randomised from a community setting.11 No significant differences were detected in either mortality (relative risk (RR) 0.82, 95% confidence interval (CI) 0.52–1.28) or functional ability (median Barthel index score 16 in both groups) for HaH compared to standard care at three months. They also found a lower total number of days of care in the HaH group at three months (median 9 v 16 days, p=0.031). However, 29 (15%) refused their allocated treatment group, and data were incomplete for 39 (20%) patients. Further analysis suggested that costs were similar between the two groups,12 but patient satisfaction was higher in the HaH arm.13 The second, Australian, trial randomised 100 patients, just 69 of whom were aged 65 or above, to HaH or standard admission from an emergency department.14 A significant number of the patients had conditions that would not normally be managed as in patients in the UK (eg 17% had a deep vein thrombosis) and 25% lived in care homes. Adverse event rates were similar between groups. Patient satisfaction was higher in the HaH arm, but length of stay was longer (average 10.1 v 7.4 days). The most recent of these trials randomised 285 older adults (mean age 80) from an acute hospital setting.15 However, the trial included both admission avoidance (76 (27%)) and early discharge patients (209 (73%)). Again they found that outcomes were similar between groups and a higher degree of patient satisfaction with the HaH group. However, the costs were significantly higher in the HaH group.
In summary, the total number of older patients with a mix of medical conditions randomised to evaluate HaH for admission avoidance to date is very small. This would appear to make the available evidence insufficient to reliably inform health policy. From current data it would appear that HaH offers similar outcomes for carefully selected groups of patients, and is associated with high patient satisfaction, but is unlikely to result in significant cost savings.
Case management
Case managers are people who help to coordinate and manage care for people with complex chronic conditions. This role can be performed by a number of professionals including those involved in health and social care. In the USA a case management system for patients in long-term nursing facilities (Evercare) had suggested lower rates of hospital admission and significant financial benefits.16
In 2004, the UK government proposed an NHS improvement plan, which included introducing community matrons.17 This role was designed for senior nurses, and proposed as that of case manager with the additional skills to diagnose and treat clinical conditions.18 The aim being to try and prevent deteriorations in health of those with complex chronic conditions and thus avoid hospitalisation, with an expectation that older people would be more likely to fall into this category. The report found that 5% of patients admitted to hospital accounted for 42% of occupied bed days across the NHS. The government proposed that over 3,000 community matrons would be in post by 2008, caring for over 250,000 patients (ie approximately 80 patients each). The hope was that emergency bed day use would be reduced by 5% by 2008.19
One problem with this approach is identifying those patients who would benefit from being case managed. A common reason for case managing a patient is having had two or more unplanned hospital admissions over a one-year period. However, an analysis found that although these patients accounted for 38% of admissions in the index year, they accounted for just 10% of admissions in the following year and 3% of admissions five years later.20 This suggests that the population at highest risk of admission is constantly changing, which may be at least partly due to high mortality rates among those with severe disability. Bearing this in mind, it is unsurprising that several non-controlled studies have suggested that those patients under the care of a community matron have lower rates of hospital admission than in the preceding period.21,22 However, an evaluation of the admission rates of practices within an Evercare pilot (n=64) to all other practices in the UK (n=6,000) found no significant reduction.23 The reasons why the results from the USA were different may relate to the nursing home based design or the use of incentive payments.
In summary, at present there is no reliable evidence that case management is effective at reducing hospital admissions. However, it may improve quality of patient care.24
Paramedic assessment service
As an alternative approach to admission avoidance, it has been proposed that ambulance crews could be trained to deliver treatment of minor conditions in the community in response to emergency calls.25 This could reduce the need for emergency department attendances and some subsequent hospital admissions. A trial randomised 3,018 older patients (mean age 82.5 years) to a specially trained paramedic service (n=1,549) or standard ambulance care (n=1,469).26 The vast majority of patients were assessed following a fall (88.9%). The rate of hospital admission over the following 28 days was lower in the intervention arm (40.4% ν 46.5%, p=0.001). Patient satisfaction levels were high and no differences in mortality rates were detected over this time period. Unfortunately the study does not tell us what treatment or referral for further assessment the patients received. Clearly the paramedic crews could not be expected to deliver a multidisciplinary assessment, which has been proven to be of value.27 Previous data have suggested that many non-conveyed fallers are at high risk of future deterioration.28 As such it is unclear if this strategy would be clinically or cost-effective in the longer term. The concern would be that patients who would benefit form multidisciplinary assessment might be denied appropriate access.
Early discharge schemes
Patients who were traditionally kept in hospital until they were able to manage at home may be able to be discharged sooner if appropriate services were available to support them in their own home.
Hospital at Home
A recent Cochrane review identified 26 trials involving the use of an HaH scheme to facilitate early discharge from hospital.29 The majority of the trials recruited patients with a specific diagnosis (eg stroke or COPD) or following surgical intervention. Seven of the trials were comprised of older adults with a mix of medical conditions (n=1,652). The following summary is limited just to this latter group.
As would be expected, length of stay in hospital was reduced in the intervention group. Unfortunately due to heterogeneity between the studies designs the authors were unable to combine data. The average reductions achieved varied between trials from less than one day to 22 days. But the total duration of care was longer in the HaH group (mean additional duration 6.43 days, 95% CI 2.84–10.03). No significant differences in mortality (HR 1.06, 95% CI 0.69–1.61), or functional ability as measured by the Barthel index (weighted mean difference 0.14, 95% CI =0.02–0.30) were detected between the intervention and control groups. However, there was an increased rate of readmission in the HaH group (HR 1.57, 95% CI 1.10–2.24). Data from three of the trials showed that HaH was associated with a lower rate of admission to residential care at one year (RR 0.69, 95% CI 0.48–0.99) and some of the studies reported increased levels of patient satisfaction (not quantified). Cost analyses varied across the trials depending on how they were calculated, making it impossible to formulate any general conclusions.
In summary, there is no strong evidence that HaH for early discharge is any cheaper than standard care, but it appears to offer similar rates of mortality and disability. There may be a lower chance of admission to residential care at one year, but offset by a higher risk of readmission to hospital. Patients generally seem to like HaH schemes.
Alternatives to standard hospital wards
A number of novel approaches have been attempted to release standard acute hospital beds.
Nurse-led units
A trial randomised 240 hospital inpatients (mean age 70.7 years) following an acute illness either to a nurse-led unit or to conventional post-acute care.30 Although outcomes were broadly similar, the length of stay within the acute hospital was on average 14.3 days longer for those in the nurse-led unit (95% CI 7.8–20.7 days). In addition, a financial analysis of this trial found significantly higher mean costs at six months in the nurse-led unit (mean excess £2,710 per patient, 95% CI £518 to £4,903).31 A further similar trial randomised 175 patients (mean age 78.3 years) to a nurse-led unit or standard care.32 Again, lengths of stay were longer in the intervention arm (mean excess stay 10.9 days, 95% CI 1.1–20.7 days), and costs were greater but this did not reach statistical significance (mean excess £1,044, 95% CI −£382 to £2,471). No differences were seen in functional ability or discharge destination. A Cochrane review of this topic was unable to reach any firm conclusions.33 In summary, there are no reliable data that nurse-led units would either release hospital beds or save money.
Community hospitals
A trial randomised 490 patients (median age 86 years) to a period of post-acute care within a community hospital or continuing standard care in an acute hospital.34 After six months of follow up there was a small but statistically significant mean improvement in Nottingham extended activity of daily living score (range 0 to 66) favouring the community hospital arm (mean difference 3.27, 95% CI 0.26–6.28), other outcomes were similar. An economic evaluation of this study found that costs were non-significantly higher in the community hospital group (mean excess £720 per patient, 95% CI −£532 to £1,964).35 A smaller randomised study (n=142) conducted in Norway actually found a lower mortality rate in the community hospital cohort compared to standard hospital care.36 The reasons for this finding are unclear. Interpreting the generalisability of studies of this type may be difficult due to the heterogeneous nature of community hospital design and staffing. During these trials the clinical staff are not blinded to patient allocation, which may introduce some bias.
Care homes
Care home beds have been utilised as transitional units for patients whose discharge has been delayed due to awaiting a permanent care home place. It has been hoped that, by providing additional rehabilitation, some of this group of patients may be able to return home after all.
A study randomised 165 older people (median age 81 years), who wished to return home but were thought to be at high risk of care home placement, to either have a period of rehabilitation within a care home environment or to continue standard hospital care following an acute hospital admission.37 Patients in the intervention arm spent less time in the acute hospital (mean reduction 8.5 days) for the index admission, but more time overall as inpatients (hospital or rehabilitation unit) over a 12-month period (mean excess 19.1 days). There were no significant differences in functional ability, mortality or care home placement rates after 12 months. Another study randomised 320 patients (mean age 83 years) to transfer of care to a transitional unit (n=212) or continued waiting within a standard hospital (n=108).38 The intervention group had on-going routine input from physiotherapy and weekly multidisciplinary team meetings, whereas the control arm did not. As might have been expected, the duration of stay within the acute hospital was shorter in the intervention arm (median 11 days), but the total time before placement was increased (median 21 days). Other outcomes were similar, only 7% of the intervention group and 9% of the controls were ultimately able to return home.
This strategy may increase access to acute hospital beds, but is unlikely to be cost effective given the increase in overall time in care. For these groups of patients it seems that an additional period of rehabilitation has no significant sustained benefit in functional ability. It would probably be better to invest additional funding into care home provision to release hospital beds sooner, rather than develop this new model of continued hospital care.
Discussion
The available data have not shown any IC scheme to be effective at reducing acute hospital use. Although measuring outcomes and costs in complex services by conventional techniques may be too insensitive to detect genuine gains,39 and the patients currently being admitted to IC services may not be the people most likely to benefit.40 Some designs may have a small advantage in functional outcomes and patient satisfaction, but may be more expensive than traditional inpatient care. The evaluation of cost-effectiveness may depend on whether it is assessed from the perspective of primary care, acute hospitals, or society as a whole. The current UK Payment by Results (PbR) system typically gives a standard tariff for an inpatient episode depending on the primary diagnosis, almost irrespective of length of stay. Primary care organisations stand to benefit financially by admission avoidance, secondary care by reduced length of stay.
Additional factors that lead to current rising rates of hospital admission may include the use of general practitioner on-call deputising and NHS Direct telephone services (meaning patients are unlikely to be initially assessed in the community by a doctor who knows them). Some IC services may also be subject to design flaws. For example, they may not be able to be accessed out of office hours at the time that an acute illness occurs. To date, implementation has been patchy and not accurately powered in each region to produce a specified effect. Their staffing may draw experienced people away from their previous job within the NHS (eg district nursing), without equivalent replacement.
The gold standard of care for older adults with an acute illness is the acute geriatric unit within an acute hospital. A recent metaanalysis found that specialist geriatric units offering multidisciplinary assessment were associated with a lower risk of functional decline by the time of discharge (combined odds ratio 0.82, 95% CI 0.68–0.99), a higher rate of discharge to their own home (1.30, 95% CI 1.11–1.52) with no significant difference in mortality rates.41 This is at least partly due to undertaking comprehensive geriatric assessment, which has been shown in a meta-analysis to be effective at promoting independent survival (three more patients per 100 alive and in their own home (95% CI 1–6) compared to standard care) especially when performed within a specialised ward environment.42 In many of the studies of intermediate care the control arm is ‘standard hospital care’. Exactly what this entails may vary. In overcrowded hospitals older patients may be cared for in non-specialist areas. As such it is unclear if IC has been compared to known best practice within every study.
Intermediate care services are unlikely to meet the needs of all. In an evaluation of a city-wide IC service within the UK, older patients (n=848, median age 85 years) presenting with falls, confusion, incontinence or immobility to an elderly medicine department were compared to historical controls.43 Only 29% of these patients received any IC service (mainly HaH). Functional outcomes, institutionalisation rates and mortality were similar between groups. However, compared to matched controls, those receiving IC spent longer in hospital over a 12-month period (mean excess eight days, 95% CI 3.1–13.0).
In conclusion, the evidence to support a move towards any form of IC service is still weak, even after 10 years of implementation. There are no reliable data that suggest acute hospital use will be reduced, and costs could even be increased. Bearing this in mind, should the NHS be investing in such new services that may benefit a small proportion of older patients, or should it continue investing in the more traditional system that has been shown to benefit all? This question is particularly relevant when entering an economic phase where NHS expenditure is likely to be reduced and health choices need to be made.
- © 2010 Royal College of Physicians








{kind=link}