
Abstract
Transient ischaemic attack (TIA) is the sudden onset of focal neurological dysfunction of presumed vascular origin that, by definition, resolves within 24 hours (usually much sooner). Its importance as a predictor of completed stroke has only recently been recognised. Updated guidance on the recognition and management of TIA has recently been published as part of the National Clinical Guideline for Stroke.1 This is a concise version of the TIA component of the full guideline that recommends an urgent response to TIA to prevent subsequent stroke.
Introduction and aims
It is only relatively recently that the importance of transient ischaemic attack (TIA) as a predictor of stroke has been defined. Agreed standards for the management of TIA were first published in the UK in the 2001 National Service Framework, identifying the importance of ‘rapid access TIA clinics’ for diagnosis and management. It was not until the publication of data from the OXVASC studies that the very high early risk (within hours or days) of stroke after TIA was appreciated, and with it the realisation that 14- or even seven-day assessment targets would mean that those patients at highest risk might have a stroke before they had the opportunity to attend a TIA clinic.2 This new evidence suggested that a guideline for the management of TIA would be of value to clinicians, service providers, commissioners and patients. Information in this concise guidance has been extracted from the full guideline. Please refer to the full guidance for details of the methodology and members of the guideline development group.
Aims of the guideline
The aim of this guidance is to provide updated recommendations in the following areas:
pre-hospital recognition of the symptoms of TIA
assessment of those at highest risk of stroke
appropriate referral for specialist assessment.
Pre-hospital recognition of the symptoms of TIA
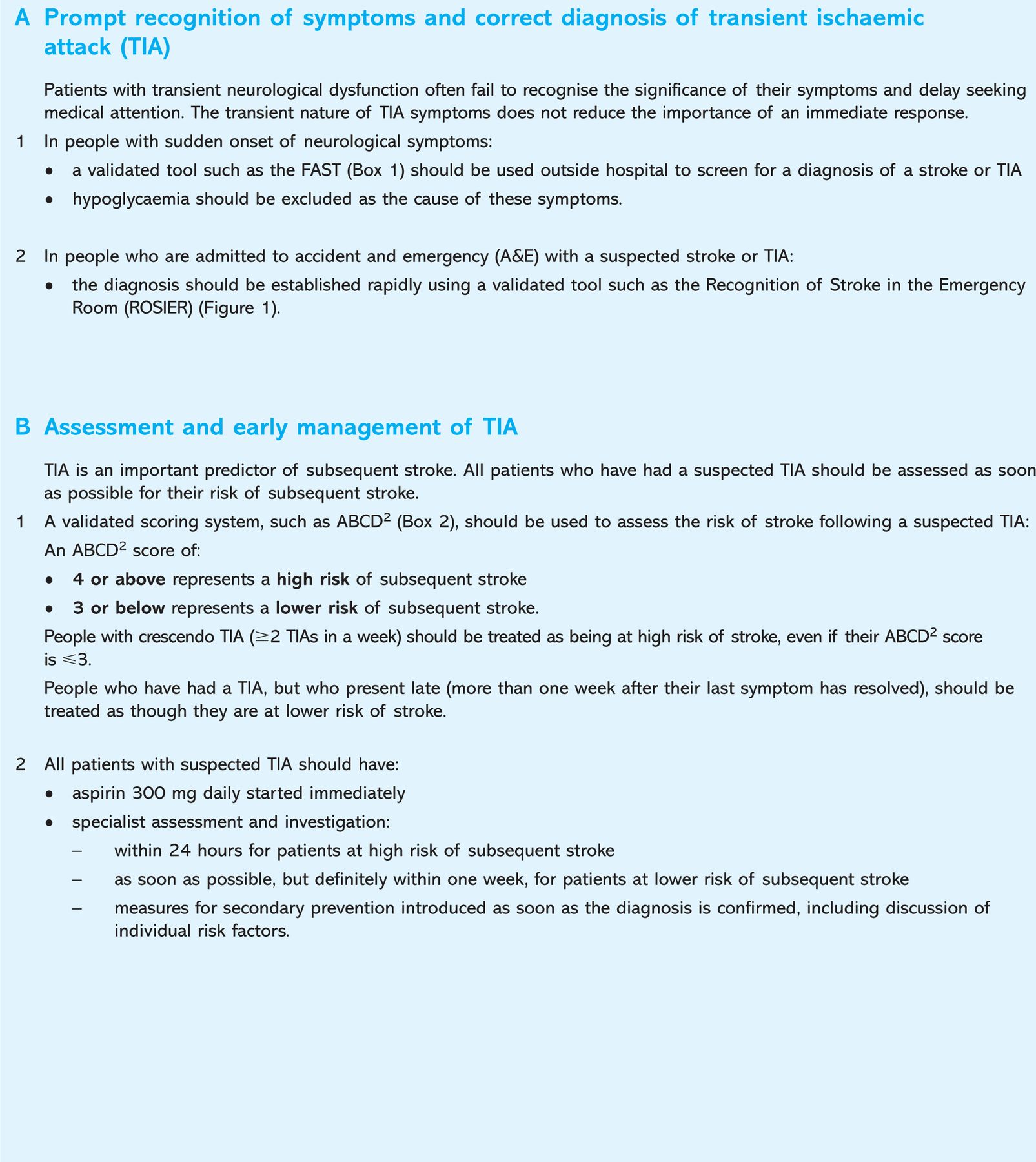
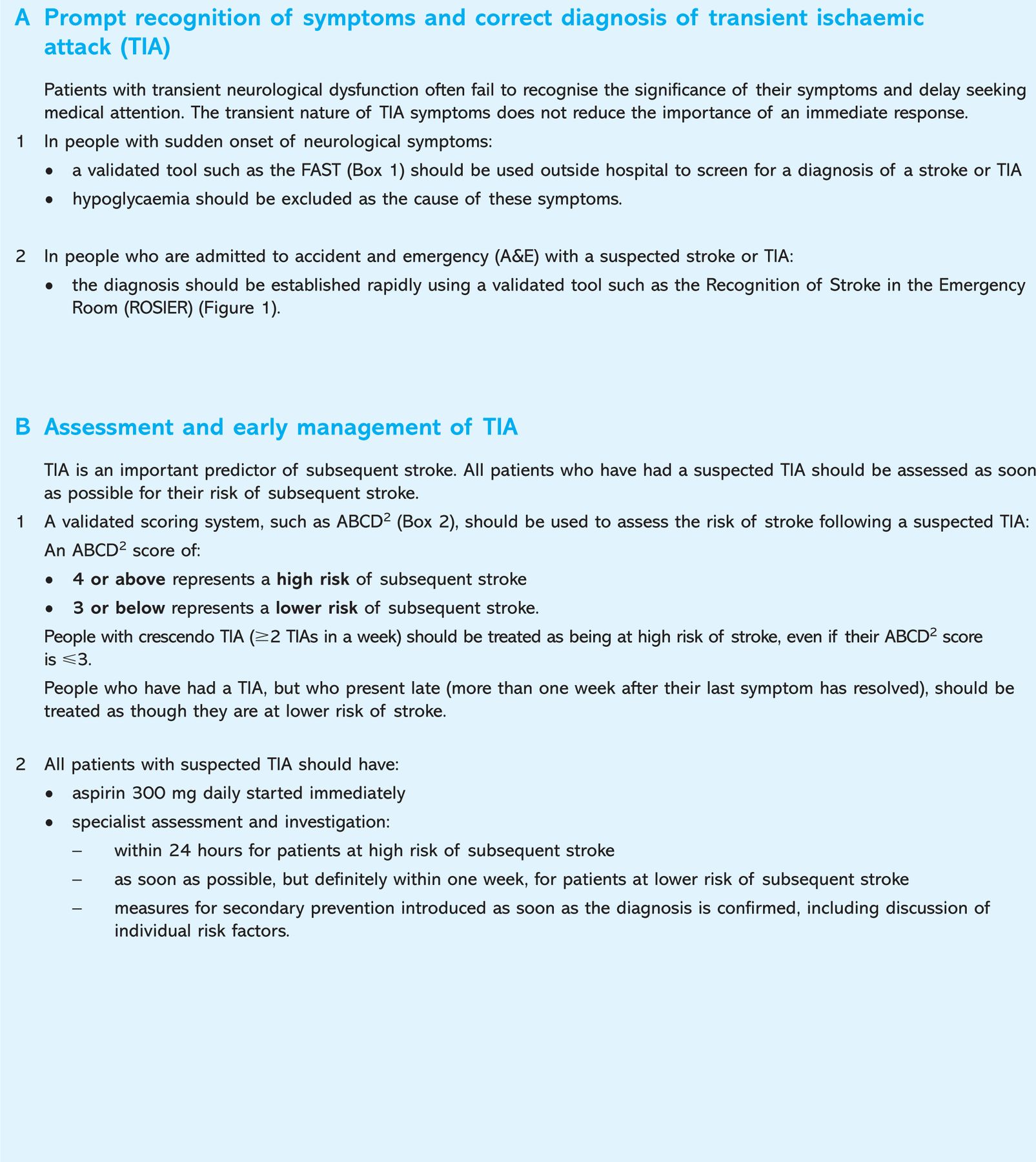
A simple recognition tool can be used to determine the symptoms of stroke; part of the education programme involves the understanding that these symptoms require urgent action, even if they only last a few minutes. The Face Arm and Speech Test (FAST) can be used by healthcare professionals and members of the public as a quick assessment (Box 1). First responders need to be aware that hypoglycaemia is an important stroke mimic and blood sugar should be checked at the earliest opportunity.
The Face Arm and Speech Test (FAST) can be used by healthcare professionals and members of the public. Adapted from reference 3. Reproduced with permission from Wolters Kluwer. TIA ? transient ischaemic attack.
The Recognition of Stroke in the Emergency Room (ROSIER) score is a more detailed version of the FAST test that is used to identify patients with likely stroke or TIA in the emergency department (Fig 1).
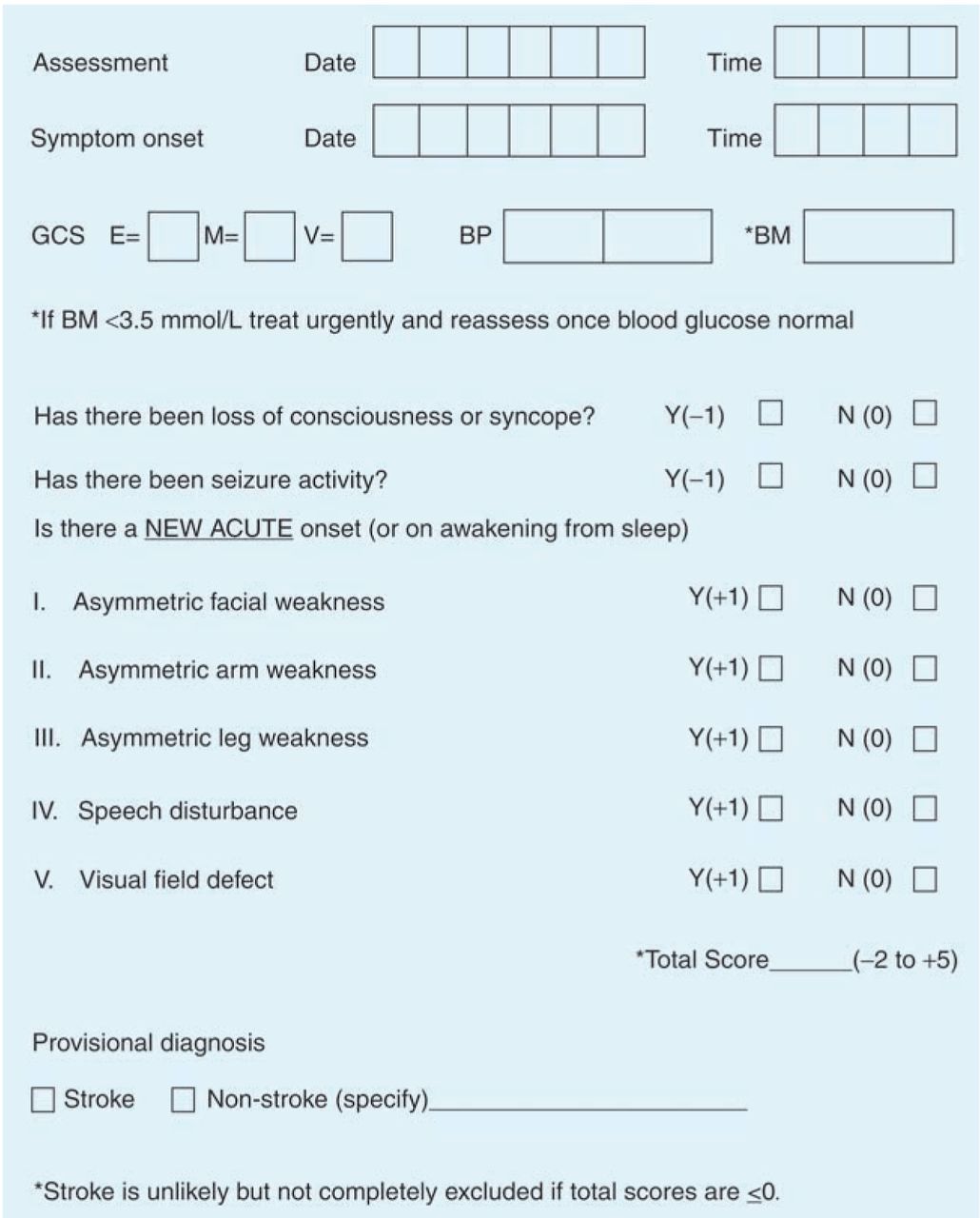
Proforma for application of the Recognition of Stroke in the Emergency Room (ROSIER) tool. Adapted from reference 4. Reproduced with permission from Elsevier. BM = blood sugar level; BP = blood pressure; GCS = Glasgow Coma Score.
Assessment of those at highest risk of stroke
Epidemiological studies of patients with TIA identified very early after symptom onset have demonstrated the clinical features associated with highest risk. These include older people (over 60 years), those with high blood pressure, diabetes, longer duration of symptoms and those with speech problems or motor weakness.
The ABCD2 score is a simple scoring system that can be used to stratify those patients who need urgent specialist assessment (within 24 hours) and those who need assessment within one week (Box 2). It can be used in primary care or by trained paramedics to determine which patients may need immediate transfer to hospital:
a score of ⋛4 is considered high risk (>4% risk of stroke over the next seven days)
those patients with low ABCD2 (<4) should receive aspirin 300 mg immediately, specialist assessment (including referral for imaging where appropriate) as soon as possible but certainly within a week, and secondary prevention as soon as the diagnosis is confirmed and risk factors discussed.
The ABCD2 score. Adapted from reference 5. Reproduced with permission from Elsevier. TIA = transient ischaemic attack.
Clinicians should also be aware that scoring systems such as ABCD2 exclude certain populations who may be at particularly high risk (eg recurrent events and those on anticoagulation) who may need urgent evaluation. They may not be relevant to those who present late.
Acute management
Staff who see and assess patients acutely (paramedics and doctors and nurses in the accident and emergency department and in general practice) need to know how to make a provisional diagnosis of TIA, assess risk, and make the appropriate referral for specialist assessment (either within 24 hours or within a week). If there are no contraindications aspirin should be provided. Key steps in management are:
-
1. confirm that there is no residual neurological deficit (exclude stroke)
-
2. check:
bloods: glucose, fasting lipids, renal function, platelets
electrocardiogram: exclude atrial fibrillation
-
3. start aspirin (unless contra-indicated)
-
4. decide whether the TIA is ‘high’ or ‘low risk’:
do they need the specialist assessment this week or within 24 hours?
get the patient to the specialist at the appropriate time.
Referral for specialist assessment
The specialist assessment will include:
confirmation of diagnosis
assessment of risk factors, lifestyle and secondary prevention advice
early pharmacological management
referral for timely brain (where appropriate) and carotid imaging, and for carotid intervention within two weeks.
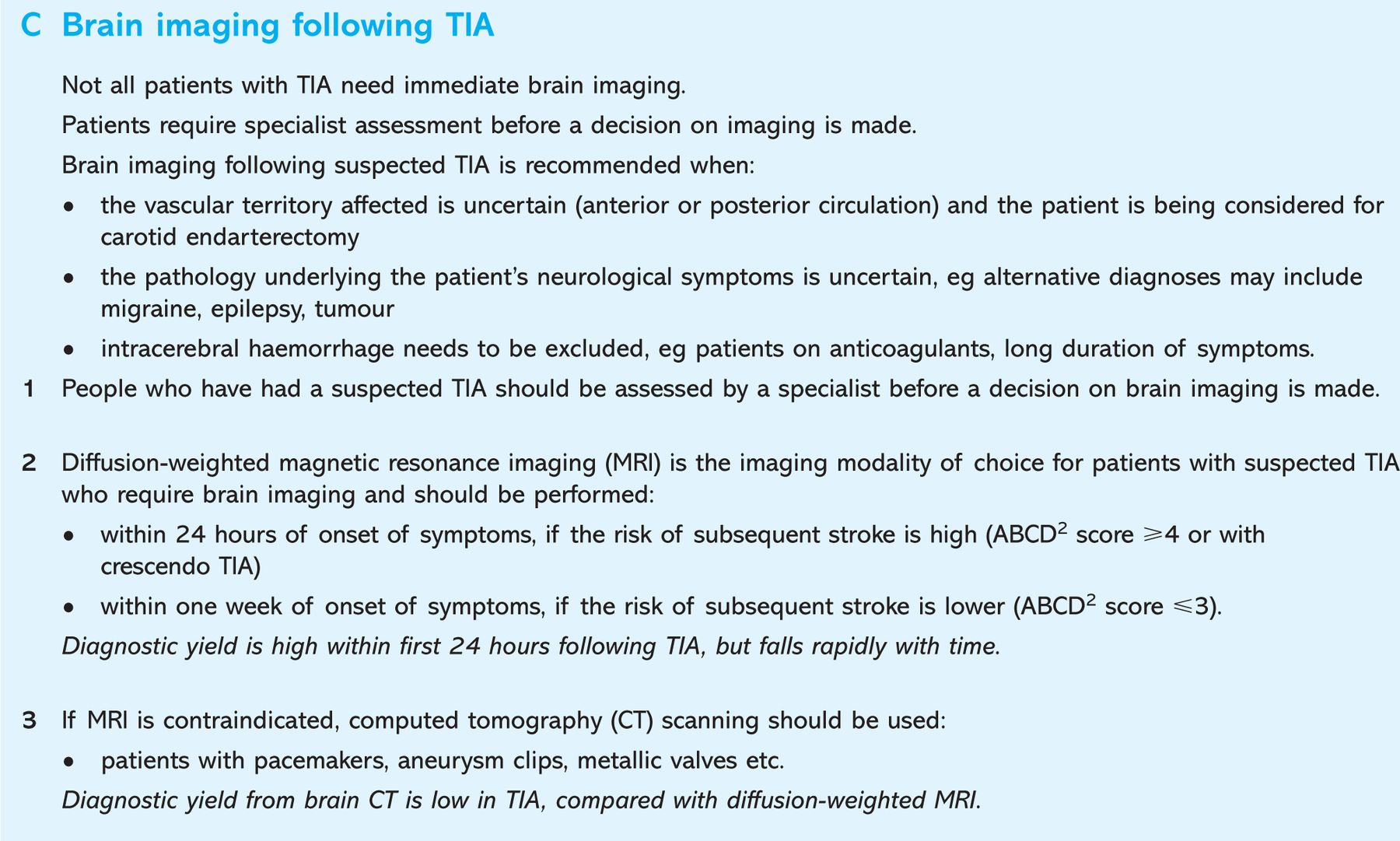
Brain imaging (ideally with diffusion weighted imaging) is valuable in those cases of diagnostic doubt (eg where there may be a differential diagnosis, for example migraine) or where the specialist is uncertain whether the ischaemic event was in the anterior or posterior circulation. Those people with anterior circulation events who are considered appropriate for carotid intervention should be referred within one week for carotid imaging. When stenosis is reported it is important that the criteria for measurement (European Carotid Surgery Trial or North American Symptomatic Carotid Endarterectomy Trial) is stated to avoid confusion. Patients with significant carotid stenosis should undergo surgery within two weeks of symptom onset. All patients with TIA need immediate management of risk factors. The results of the EXPRESS and TIA-SOS studies underline the importance of immediate treatment and lifestyle advice to reduce the risk of stroke following TIA.6,7
Footnotes
Concise Guidance to Good Practice editors: Lynne Turner-Stokes and Bernard Higgens. Guest editor: Tabitha Turner-Stokes
- © 2010 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}