
Lesson
A 78-year-old lady with no cardiac history presented to the emergency department with an episode of chest pain at rest. Her only risk factor for ischaemic heart disease was of mild, medication-controlled hypertension. There was no family history of any cardiac problems or sudden cardiac death.
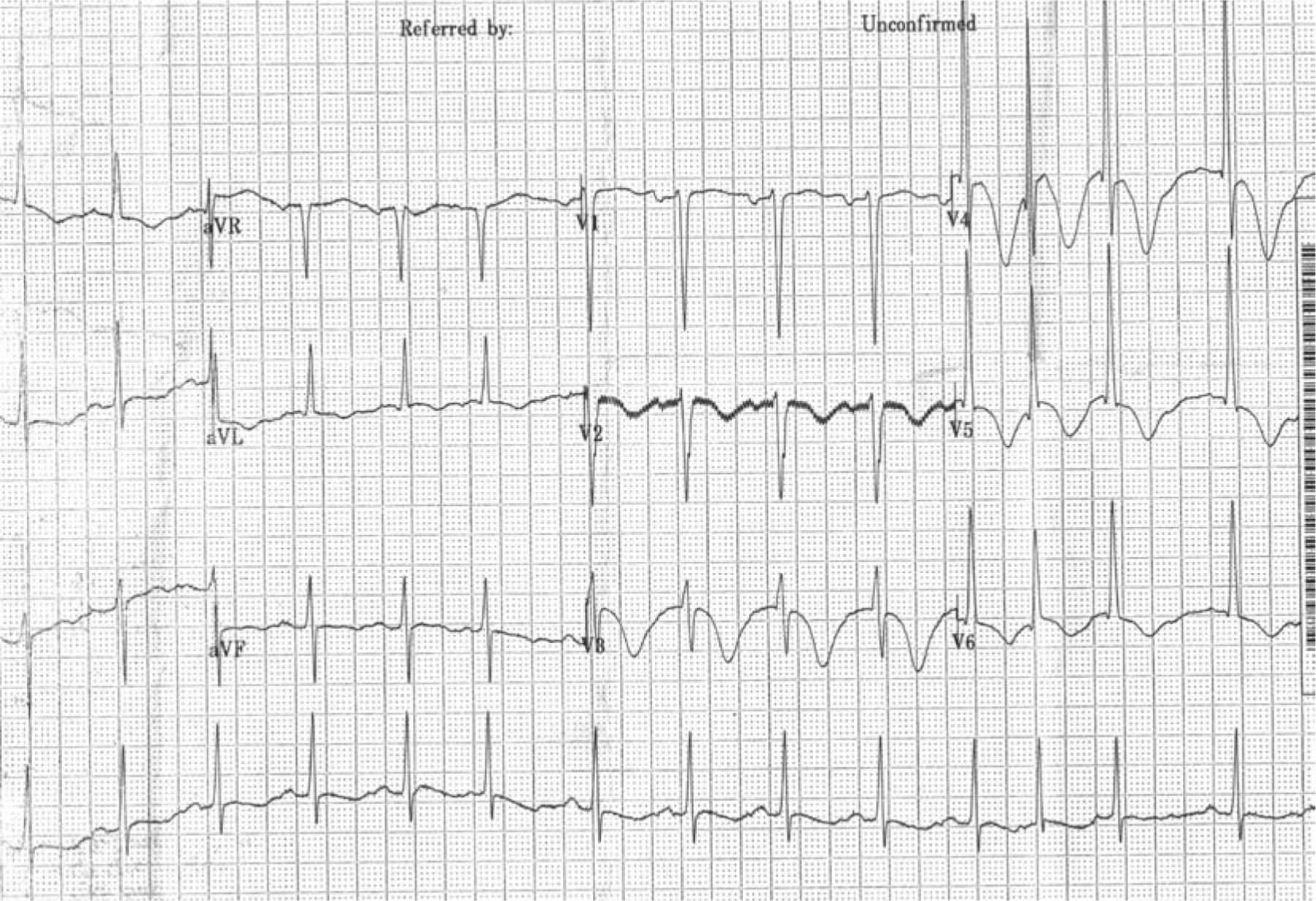
Clinical examination revealed an ejection systolic murmur. A 12-hour troponin was positive at 3.46. The admission electrocardiogram (ECG) shows voltage criteria for left ventricular hypertrophy (LVH) with marked anterolateral repolarisation changes (Fig 1). ECG monitoring over the next two days did not show any arrhythmia.
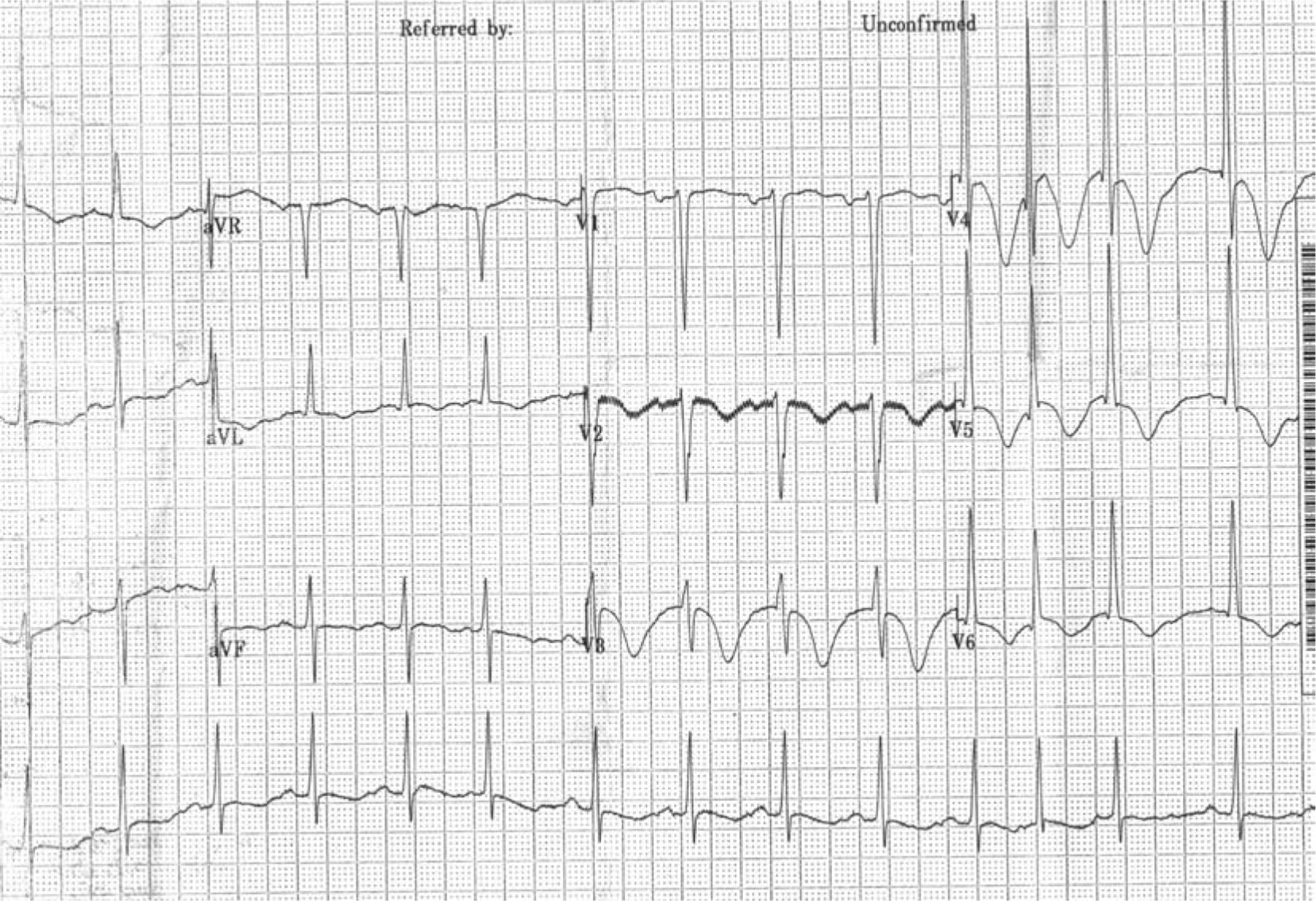
The admission 12-lead electrocardiogram.
A percutaeneous coronary angiogram was normal. Transthoracic echocardiography revealed severe (2.1 cm) asymmetric hypertrophy of the proximal anteroseptal wall of the left ventricle with systolic anterior motion of the anterior mitral valve leaflet and an eccentric jet of mitral regurgitation. The pressure gradient measured in the left ventricular outflow tract at rest was 123 mmHg (Fig 2).

Transthoracic echocardiogram showing a four chamber apical view. Severe asymmetrical hypertrophy of the intraventricular septum is shown. LA = left atrium; LV = left ventricle; RA = right atrium.
These echocardiographic findings are classical of hypertrophic cardiomyopathy (HCM), with the pressure gradient suggesting severe left ventricular outflow tract obstruction. Treatment was commenced with a beta blocker. The patient has been asymptomatic since admission. The son and daughter of the patient were advised to undergo screening for HCM with an ECG and echocardiography via their local cardiology department.
Although systemic hypertension can result in LVH, this is usually less severe and concentric rather than asymmetric in nature. It rarely causes such severe outflow tract gradients. Furthermore the ECG changes seen in Fig 1 would be extremely atypical for purely hypertensive heart disease.
Discussion
HCM is a genetic disorder that can present at any age, but is often overlooked in older patients due to the perception of it being a disease of only the young.1 Anginal symptoms are sometimes described by patients with HCM. This is likely to occur due to abnormal microvasculature in the left ventricle.2 Therefore angiography of the epicardial arteries is often unremarkable. The positive troponin in this case could be explained by either small vessel disease, HCM itself or possibly by an arrhythmic process.
Left ventricular outflow tract obstruction (LVOTO) has been reported to be more common in older patients with HCM.3 Current guidelines suggest treatment of LVOTO should begin with medical therapy.4 This is usually with beta blockade, although verapamil or disopyrimide are alternatives. If the patient continues to have symptoms despite optimal medical therapy, alcohol septal ablation or surgical myectomy can be considered, although neither of these interventions has been shown to confer any prognostic benefit.5,6 A detailed discussion of these two procedures is beyond the scope of this report.
Sudden death risk stratification in HCM can be complicated. This can make it difficult to decide which patients should be fitted with an implantable cardioverter defibrillator (ICD) to try to prevent sudden cardiac death. The patient discussed in this report has no high-risk features to suggest that this might occur (Table 1). Of note, a treadmill test to investigate blood pressure response to exercise was not performed due to the request of the patient.
Risk factors for sudden cardiac death in hypertrophic cardiomyopathy.4 ECG ? electrocardiogram.
In some studies, LVOTO has been linked with sudden cardiac death, however, there remains some doubt about the strength of this association.4 As the risk of sudden cardiac death for this patient was low, an ICD was not indicated.
Conclusions
HCM can present in patients of any age. An ECG showing voltage criteria for LVH with severe repolarisation changes should alert the physician to this possibility. In such a scenario, a past history of hypertension should not be used to explain the ECG changes without further investigation. Transthoracic echocardiography will make the diagnosis in most patients.
- © 2010 Royal College of Physicians








{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.