
Abstract
Typhoid fever should be considered in the diagnosis of any patient with a fever from the Asian community even in the absence of a travel history to an endemic region. Blood cultures taken prior to antibiotics are the best way of making the diagnosis early and preventing the complications that arise from a prolonged bacteraemia.
Lesson
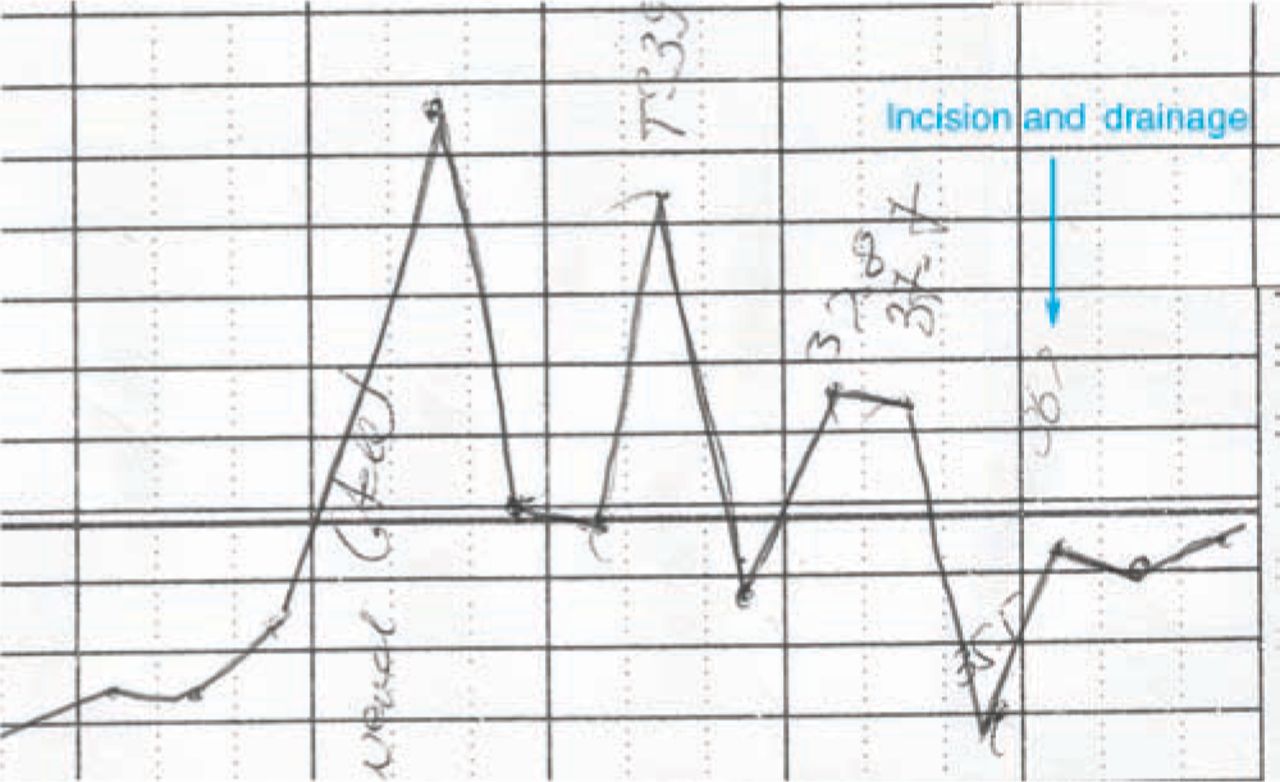
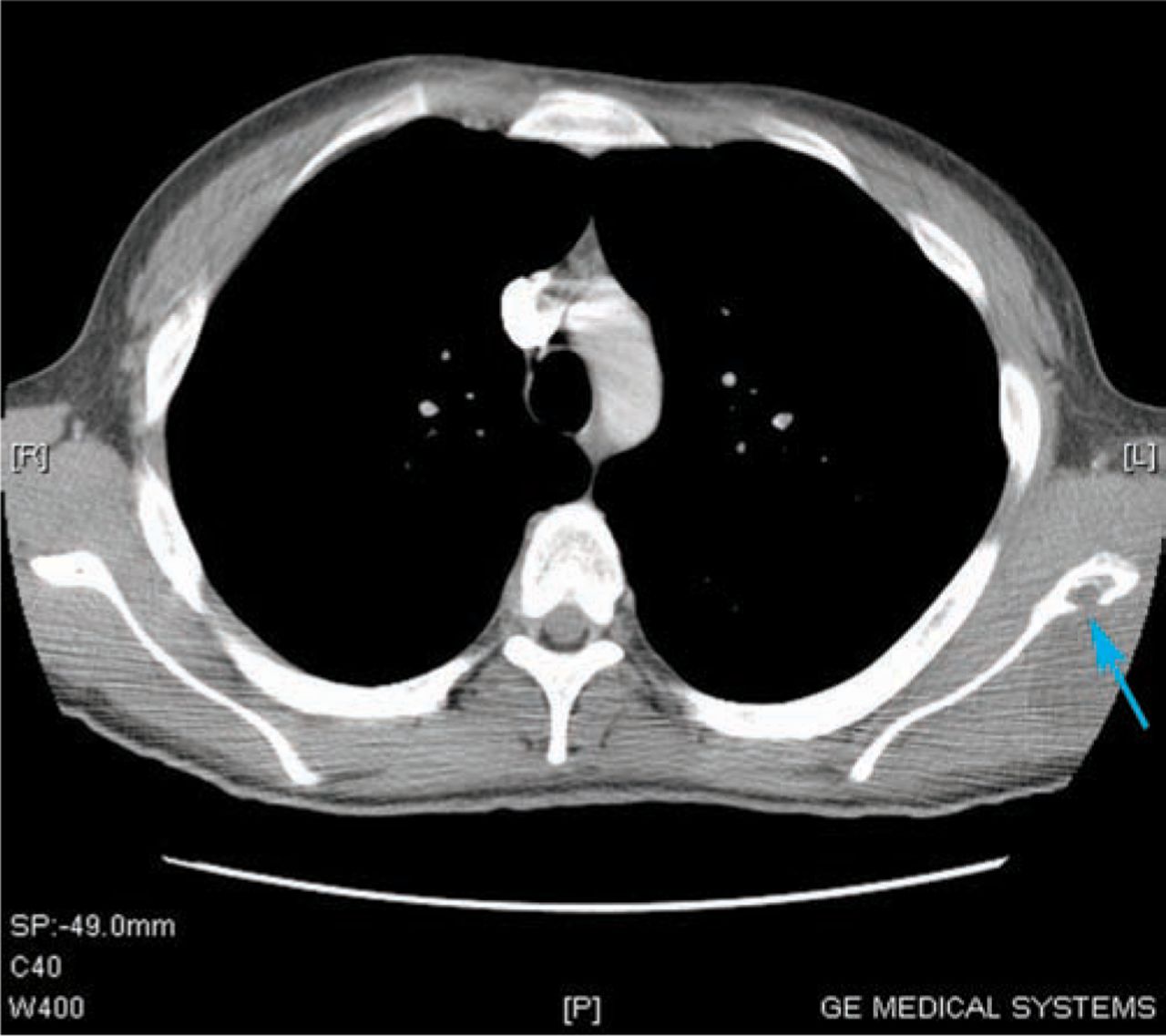
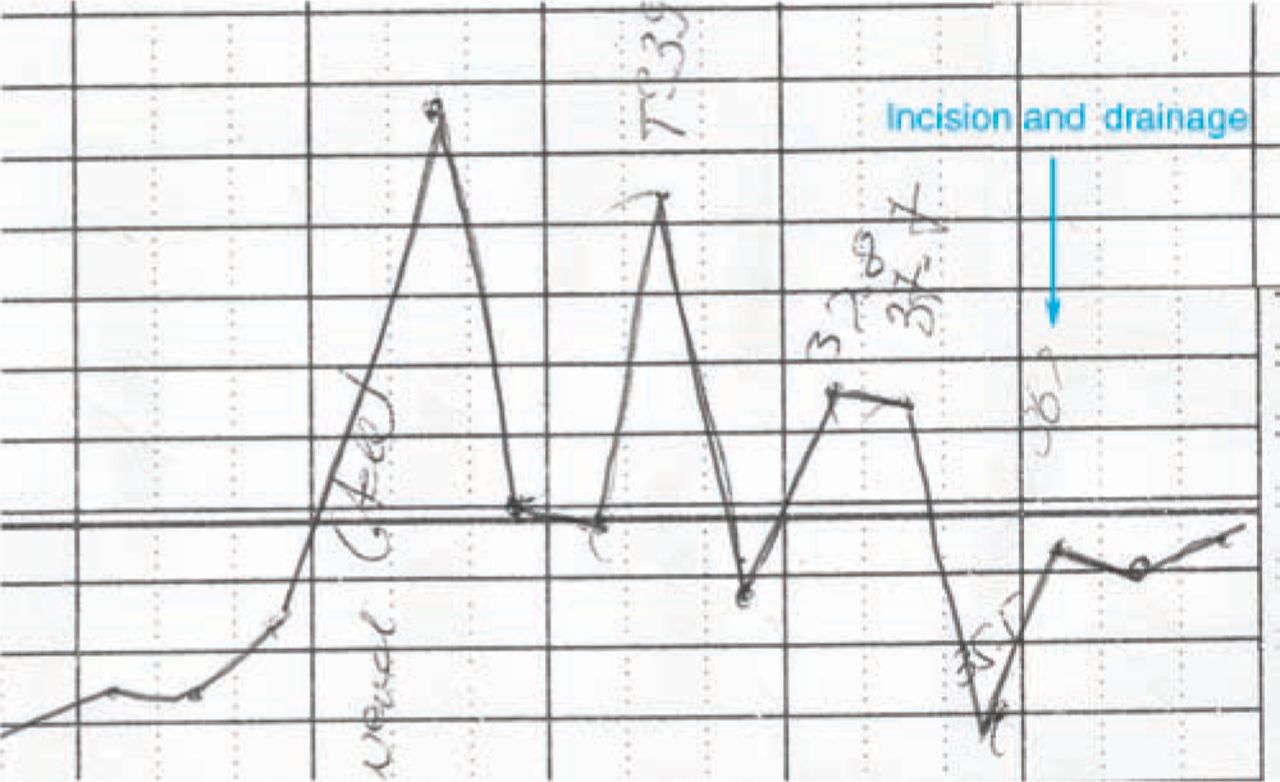
A 21-year-old Asian baggage handler at Heathrow airport presented to hospital in diabetic ketoacidosis. He was acutely unwell, with a fever (39°C), leucocytosis (16.8 ∗109/L) and raised C-reactive protein (268 mg/l). He had no recent travel history and on clinical examination there was no apparent focus of infection. He responded well to initial resuscitation, including empirical co-amoxiclav but his fever persisted for three weeks. Thorough investigations including computed tomography (CT) scans were reported as normal. One week into his admission he complained of left shoulder pain, thought to be from an occupational injury sustained while loading baggage. Shoulder joint examination and plain shoulder X-rays were normal. A fluctuant swelling developed over his left scapula and the previous chest CT scan was reviewed. A hypodense area surrounding the left scapula with abnormality of the bone was noted (Fig 1). Frank pus was aspirated from the abscess (Fig 2) and the shoulder pain and fever resolved following incision and drainage (Fig 3).


Culture of the pus yielded Salmonella enterica serovar Typhi from enrichment broth and he was successfully managed with six weeks of ciprofloxacin. It transpired he had contracted typhoid fever aged nine following a visit to Pakistan. Although the recent and historical isolates were the same phage type (E1), resistance typing revealed significant differences. The shoulder osteomyelitis was due to re-infection rather than recurrence of his previous infection.
Discussion
Given the absence of a travel history, S. Typhi was almost certainly acquired from a carrier or an asymptomatic case in the local community. All household contacts were negative on screening. The recent Health Protection Agency enhanced surveillance study of enteric fever reported that 6.5% (26/399) of enteric fever patients did not travel outside the UK before their illness.1 Lack of a travel history therefore does not preclude a diagnosis of typhoid fever. This case highlights several other aspects of Salmonella enterica serovar Typhi infection; not least the importance of taking blood cultures prior to empirical antibiotics but also its potential to cause osteomyelitis and a subsequent abscess.
Acknowledgements
Laboratory of Enteric Pathogens at the Centre for Infections, Health Protection Agency, 61 Colindale Avenue, London, NW9 5EQ (Elizabeth de Pinna and John Wain).
- © 2010 Royal College of Physicians
Reference








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.