
Abstract
Pressure on working hours has led to a decrease in opportunities for training in invasive medical procedures for junior doctors. The effect of a structured course on immediate and medium-term changes in self-reported confidence was investigated. A one-day model-based practical course was run on two separate occasions teaching central venous line placement, lumbar puncture, Seldinger-technique chest drain insertion and knee joint aspiration. Attendees were asked to indicate their confidence in each procedure on a 10-point Likert scale before, immediately after and three months after the course. Significant improvements in self-reported confidence were seen for all procedures which were sustained at three months. Feedback was universally positive. Practical pre-clinical training may be a useful adjunct to patient-based training in invasive procedures. The course was particularly popular with foundation year trainees: ideally this training should be available before trainees' first exposure in the clinical setting.
Introduction
Reductions in the working hours of junior medical trainees over recent years have resulted in a contraction of the time available for training in the emergency setting. One of the consequences of this is a relative loss of training opportunities in emergency interventional procedures, with junior doctors potentially taking longer to achieve the competence to perform these techniques independently. Despite the critical role of these skills, formal training is rarely routinely available and therefore the first exposure to these procedures is usually the opportunistic setting with the acutely unwell patient. This situation is less than ideal for the first exposure to such interventions: it can be intimidating, is often carried out under considerable pressure and an adverse outcome has the potential to undermine the confidence of the trainee.
Healthcare providers and institutions are obligated to take steps to minimise risk in patient care. Invasive procedures are a significant potential cause of such risks during inpatient care: for instance, more than 15% of patients undergoing central venous (CV) line placement will experience complications.1 Emphasis on minimising the risk of invasive procedures is reflected in recent National Institute for Health and Clinical Excellence (NICE) guidelines, which have recommended the routine use of ultrasound guidance during CV line placement in light of clear evidence that this reduces complication rates.2 Despite these issues, the provision of training still relies largely on the ‘see one, do one, teach one’ approach which is increasingly at odds with the needs of trainees.3 Medical students and junior doctors are now frequently trained to perform simple procedures such as phlebotomy and cannula insertion on models. Although many trusts provide training sessions in ultrasound-guided CV line placement, this is by no means ubiquitous, and non-patient based training in other interventional procedures is infrequently available. Here, findings following a structured course in invasive procedures designed for junior medical trainees in a district general hospital (DGH) are described.
Methods
A one-day course was designed and implemented providing small group training in central venous cannulation (CVC) (ultrasound and landmark guided), lumbar puncture (LP), chest drain (CD) insertion (Seldinger technique) and knee joint (KJ) aspiration. Each station was run by a medical registrar with extensive experience of the procedure. A brief talk outlining the indications, up-to-date guidelines, risks, issues of informed consent, technique and complications of each procedure was given prior to practical instruction in the technique. For this, anatomical models were used and trainees were given one-to-one instruction with ample time to practise. Particular emphasis was also given to familiarisation with the equipment, preparation of the patient and strict aseptic technique. The emphasis of the course was on improving confidence and for this reason there was no formal assessment of competence. The course was run on two separate occasions at a DGH with a busy acute medicine department: places were offered to all doctors in training on a first-come-first-served basis.
Attendees were asked to complete an anonymous questionnaire before, immediately after and three months after the course to rate their confidence in the skills taught on a scale of one (none) to 10 (excellent). For the three-month questionnaire respondents were contacted by email and asked to complete an anonymous web-based survey containing the same questions as the two previous written questionnaires. Non-respondents were emailed again on two further occasions. Significance was tested using the Friedman analysis of variance test with Dunn's post-test and set at p<0.05.
Results
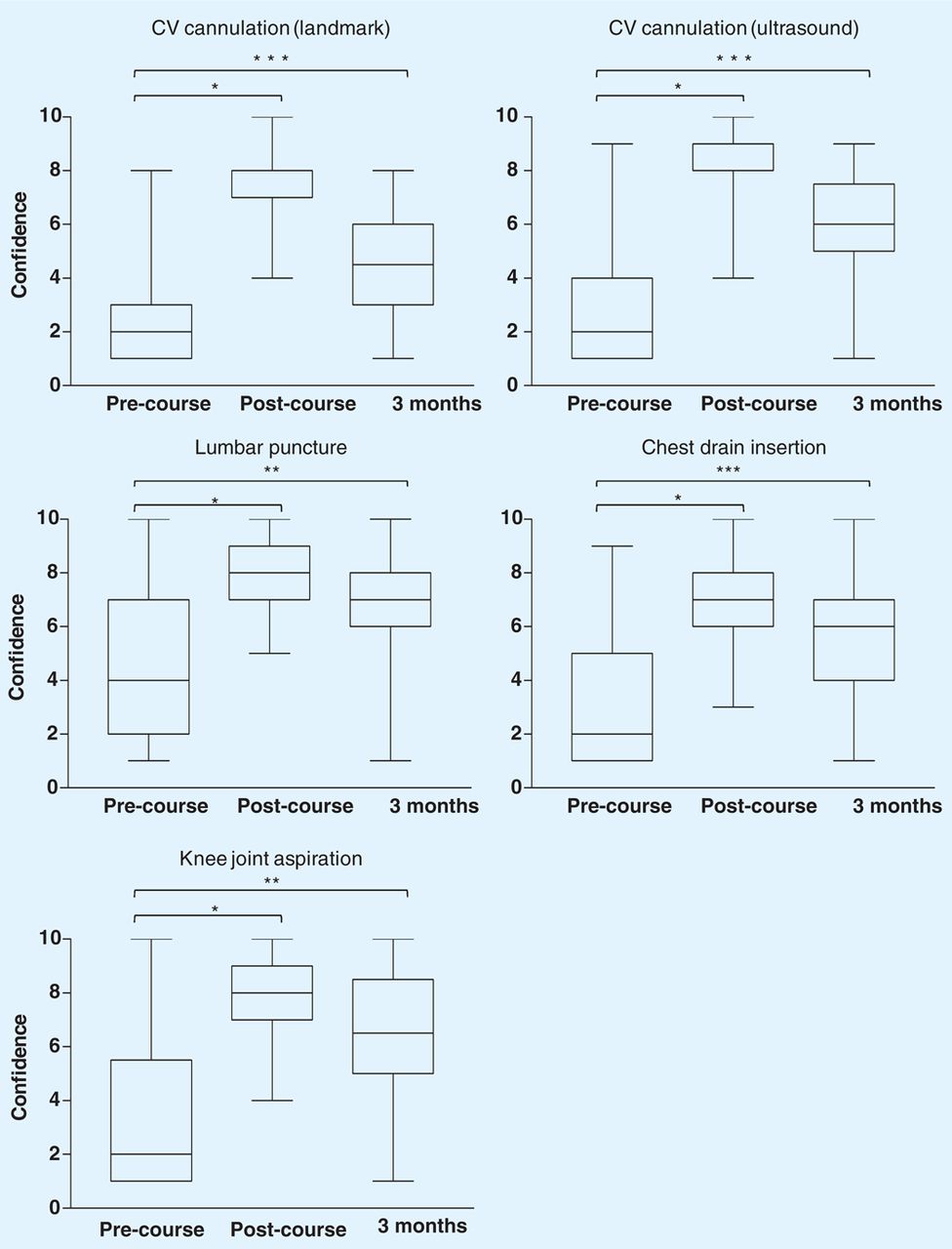
All attendees (43) completed the immediate post-course questionnaire, two of the pre-course questionnaires were not returned. Of these, 30 (70%) completed the three-month post-course questionnaire. Sixty-nine per cent of attendees were foundation year (FY)1, 14% FY2 and 17% specialty training (ST) trainees. Prior hands-on experience of the procedures ranged from 62% of delegates for LP to 12% for landmark-guided CVC (Table 1). Self-reported confidence in each of the procedures increased significantly immediately after the course and an increase was sustained at three months when compared with the pre-course results for all procedures (Fig 1). A small but significant fall was seen between the post-course and three-month results for both CVC techniques which were the least performed in this period. There was substantial variation in the proportion of delegates who had performed procedures in the three-month post-course period ranging from 4% (landmark-based CV cannulation) to 71% (LP) (Table 1). Feedback was universally positive and all attendees said they would recommend the course to colleagues.
The proportion of course attendees who had performed the indicated invasive procedures prior to the course and in the three months immediately afterwards.
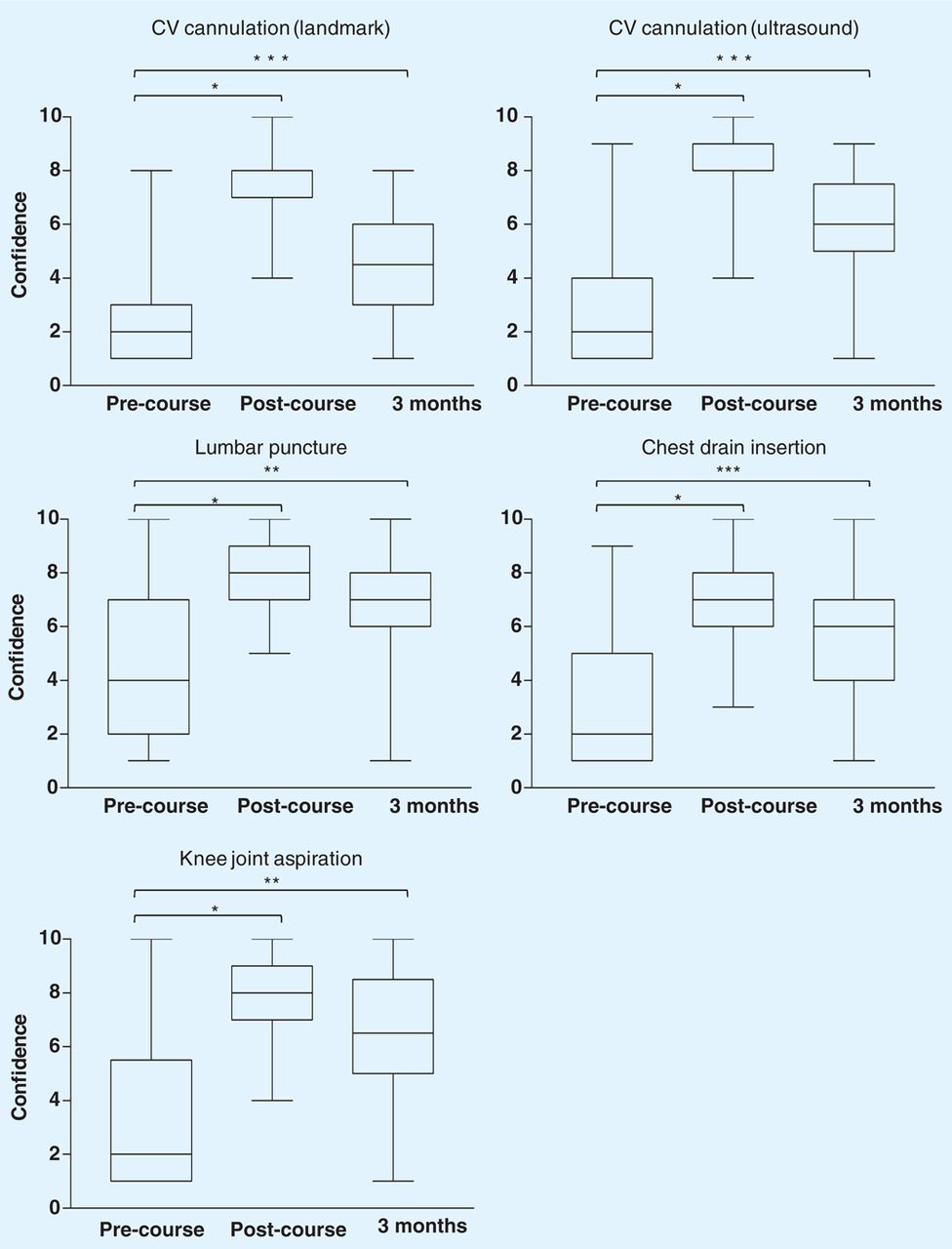
Self-reported confidence before and after the course. Trainees were asked to indicate their confidence on a 10-point scale from one (none) to 10 (excellent) before, immediately after and three months after the course. Significant differences were seen for all procedures at both post-course time points compared with the pre-course scores (p=<0.01). Horizontal bar = median, box = interquartile range, vertical bars = range. ∗p=<0.001, ∗∗p=<0.01, ∗∗∗p=<0.05.
Discussion
The procedures described in this study are essential skills for the acute medical physician and form part of the core medical training (CMT) curriculum.4 Opportunities for training are being eroded by implementation of the European Working Time Directive, but the emphasis is still on learning new techniques in the acute setting with formal teaching programmes infrequently available. A limited number of studies, principally from the USA, have looked at the attitudes of trainees to training in invasive procedures, and these have identified substantial levels of discomfort – in one such study this was despite the trainees having performed the prerequisite number of procedures to achieve independence.5,6
Approaches other than model-based training include the use of cadavers, which has been shown to improve competence and outcomes,7–9 but its use is limited by practical constraints. A ‘procedure firm’, to which trainees were assigned for two weeks, produced only modest improvements in confidence.10 The use of models has been shown in various settings to improve competency and confidence.11–13 Models are available for the teaching of a number of procedures and while even the best of these have limitations in terms of realism, they can provide a useful platform on which to base procedure skills training prior to their application on patients. Many hospitals have skills laboratories equipped to varying degrees with these resources. Importantly, whereas patient-based training by necessity has to consider, foremost, the clinical needs of the patient, the use of models allows a strictly learner-centred experience. Educational research has shown that deliberate practise and immediate structured feedback are crucial to skills acquisition15 and structured learning within the environment of the clinical skills laboratory enables this in a safe environment and encourages reflective learning.16 A number of studies have shown the benefits of model-based training – dedicated training sessions or courses which include practical instruction on models have been shown to improve competency and confidence.11–14,17 However, no data are currently available for patient outcomes. The use of simulation-based training is also gaining ground in surgery and is increasingly recognised as a useful tool for safe, learner-centred training.18,19 This was given particular emphasis in the recent chief medical officer's annual report.20
Likert scales have been previously used to assess the confidence of trainees in aspects of performing medical procedures and were deemed an appropriate tool for use in this study.5–7,10 The data presented in this study would be strengthened by the presence of a control group: the intention of the course was to offer training to as many junior doctors as wished to attend and a control group would therefore have been subject to selection bias. Furthermore, controlling for clinical experience in a hospital where trainees rotate through a variety of posts would have been difficult. Assessment of competence was outside the scope of the one-day course: the intention was to improve confidence and provide a basis of familiarity with the procedure. Furthermore, it was felt that formal assessments after a relatively short course were inappropriate and could potentially undermine the primary objective of the course. Assessment of competence could not have been achieved by a self-reported questionnaire as the poor association between self-reported competence and objective competence is well documented.21 Whether or not they attended the course, all trainees would have appropriate supervised training on patients. It is hoped that this study will provide a foundation for further work: the effect on a course such as this on the subsequent acquisition of procedural skills, particularly in terms of time needed to achieve objective competence, would be of particular interest in the setting of a controlled trial.
This study has shown that a simple relatively inexpensive course produces sustained improvement in trainee confidence in the medium term and it is anticipated that this foundation would enhance learning and skill acquisition when subsequently performed in the clinical setting. The popularity of the course among FY trainees (who made up 69% of attendees) was surprising as the course had not been specifically targeted at this group. This training is likely to be of greatest benefit prior to clinical exposure and should be considered as part of FY and CMT programmes.
Conclusion
Structured teaching in invasive procedures is popular and effective in improving confidence in junior medical trainees. We believe training should be made available to junior doctors at an early stage in their careers.
- © 2010 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- Postgraduate medical procedural skills: attainment of curricular competencies using enhanced simulation-based mastery learning at a novel national boot camp
- Procedural instruction in invasive bedside procedures: a systematic review and meta-analysis of effective teaching approaches
- Intercostal chest drain insertion by general physicians: attitudes, experience and implications for training, service and patient safety