
- angiotensin-converting enzyme inhibitors
- angiotensin receptor blockers
- chronic kidney disease
- diabetic nephropathy
- hypertension
- microalbuminuria
Key Points
Annual screening for microalbuminuria is recommended for all patients with diabetes
Effective treatment of hypertension is the most important of the modifiable risk factors in preventing progression of diabetic nephropathy (DN)
Clinical trials have shown that it is possible to alter the natural history of DN by targeting multiple risk factors (eg smoking cessation, achieving tight glycaemic control and lowering blood pressure)
Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers are indicated for patients with hypertension and/or albuminuria and can be used at all stages of DN with appropriate monitoring
Timely referral for those approaching end-stage renal disease is imperative to ensure adequate individual planning for renal replacement therapy
Diabetic nephropathy (DN), a common chronic kidney disease (CKD) aetiology, has become the most frequent cause of end-stage renal disease (ESRD) requiring dialysis and/or renal transplantation.1,2 DN is costly to manage and associated with a substantially increased risk of cardiovascular disease and premature death. In the UK, DN now accounts for 24% of incident patients with ESRD.2 The risk of developing DN is similar in both type 1 (T1DM) and type 2 diabetes (T2DM) but most diabetic patients with ESRD will have T2DM, reflecting the higher prevalence of T2DM in the population.
Diagnosis
A diagnosis of DN should be considered in patients with any form of diabetes and albuminuria. The urinary albumin excretion can range from microalbuminuria (30–300 mg/24hr) through ‘dipstick-positive’ proteinuria (300 mg/24hr) to nephrotic range proteinuria (>3.5 g/24hr). Albuminuria is usually associated with hypertension and a later decline in renal function. Other microvascular diabetic complications are usually present: 90% of patients with T1DM and 70% of patients with T2DM with nephropathy also have retinopathy. Timed urine collections are cumbersome and often inaccurate, so the diagnosis can be made in a diabetic patient with an elevated urinary albumin:creatinine ratio on at least two occasions separated by three months (Table 1). DN is presumed to be the cause of albuminuria in diabetic patients when there is no evidence of other kidney disease on history, clinical examination or renal ultrasound. A renal biopsy is not required for diagnosis.
Equivalent ranges of urine protein loss. Diabetic nephropathy is present when there is persistent albuminuria on repeated testing.
Aetiology
DN is a complex multifactorial disorder with both genetic and environmental components. Clinical risk factors associated with the onset and progression of DN have been identified, many of which are modifiable (Table 2).
Risk factors for development and progression of diabetic nephropathy (DN).
Effective treatment of hypertension is the most important of the modifiable risk factors in preventing progression of DN. In the UK Prospective Diabetes Study (UKPDS), blood pressure (BP) control (144/82 mmHg v 154/87 mmHg) had more impact on diabetic outcomes than glycaemic control (HbA1c 7.0% v 7.9%) in terms of microvascular complications and mortality.3 Even loss of nocturnal ‘dipping’ of BP increases the risk of developing microalbuminuria.4
Pathogenesis
The pathogenesis of DN is incompletely understood, but chronic hyperglycaemia is associated with long-term glomerular haemodynamic changes and dysregulation of a number of metabolic pathways. Elevated extracellular glucose levels result in renal cell hypertrophy, expansion of the extracellular matrix, increased levels of profibrotic growth factor and transforming growth factor.
Renal cell injury also results from interaction with advanced glycation end-products (AGEs) formed by non-enzymatic glycation of amino acids and proteins. AGEs can bind to the vascular wall and basement membranes, leading to release of free radicals, damage to the microcirculation, endothelial cell activation and promotion of atheroma.
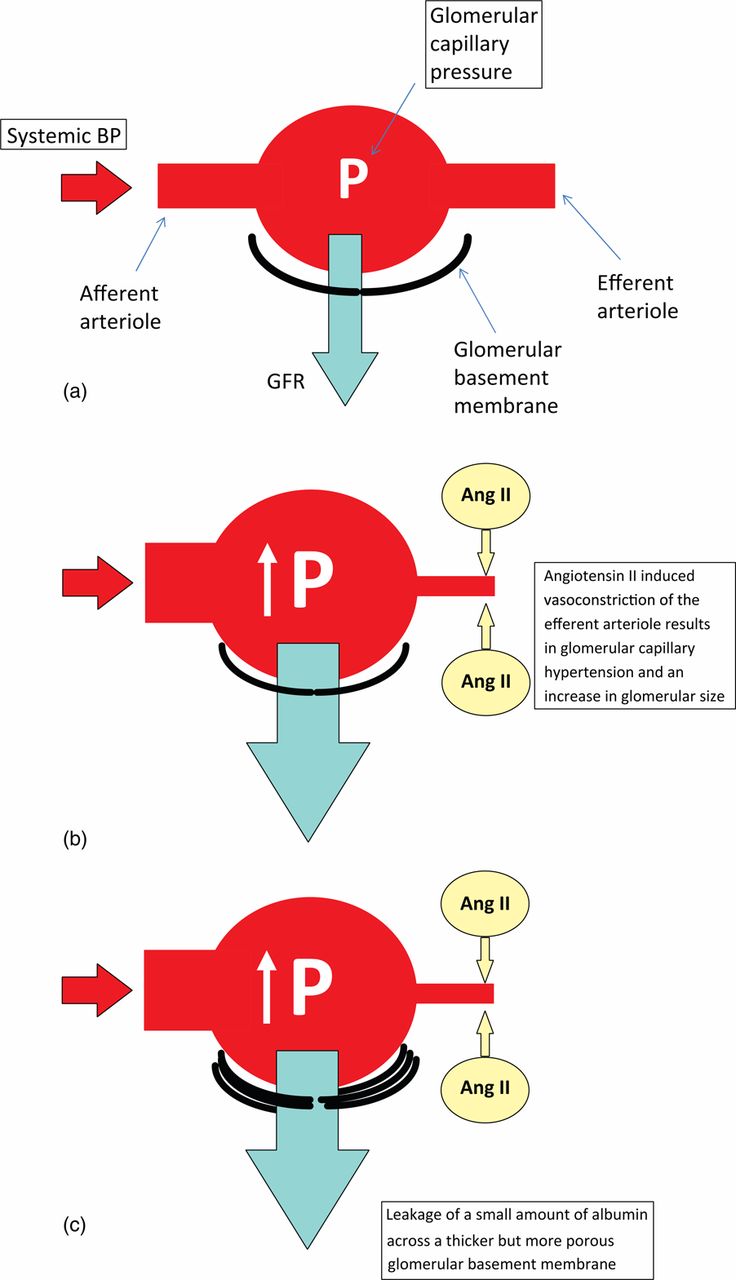
In parallel with the metabolic abnormalities there are sustained changes in the renal microcirculation leading to a rise in glomerular capillary pressure. These haemodynamic effects result in glomerular capillary hypertension. This is mediated in part by angiotensin II-induced vasoconstriction of the efferent arterioles (Fig 2). Initially, this can lead to a rise in glomerular filtration rate (GFR) resulting in supranormal GFR (a state referred to as ‘hyperfiltration’).
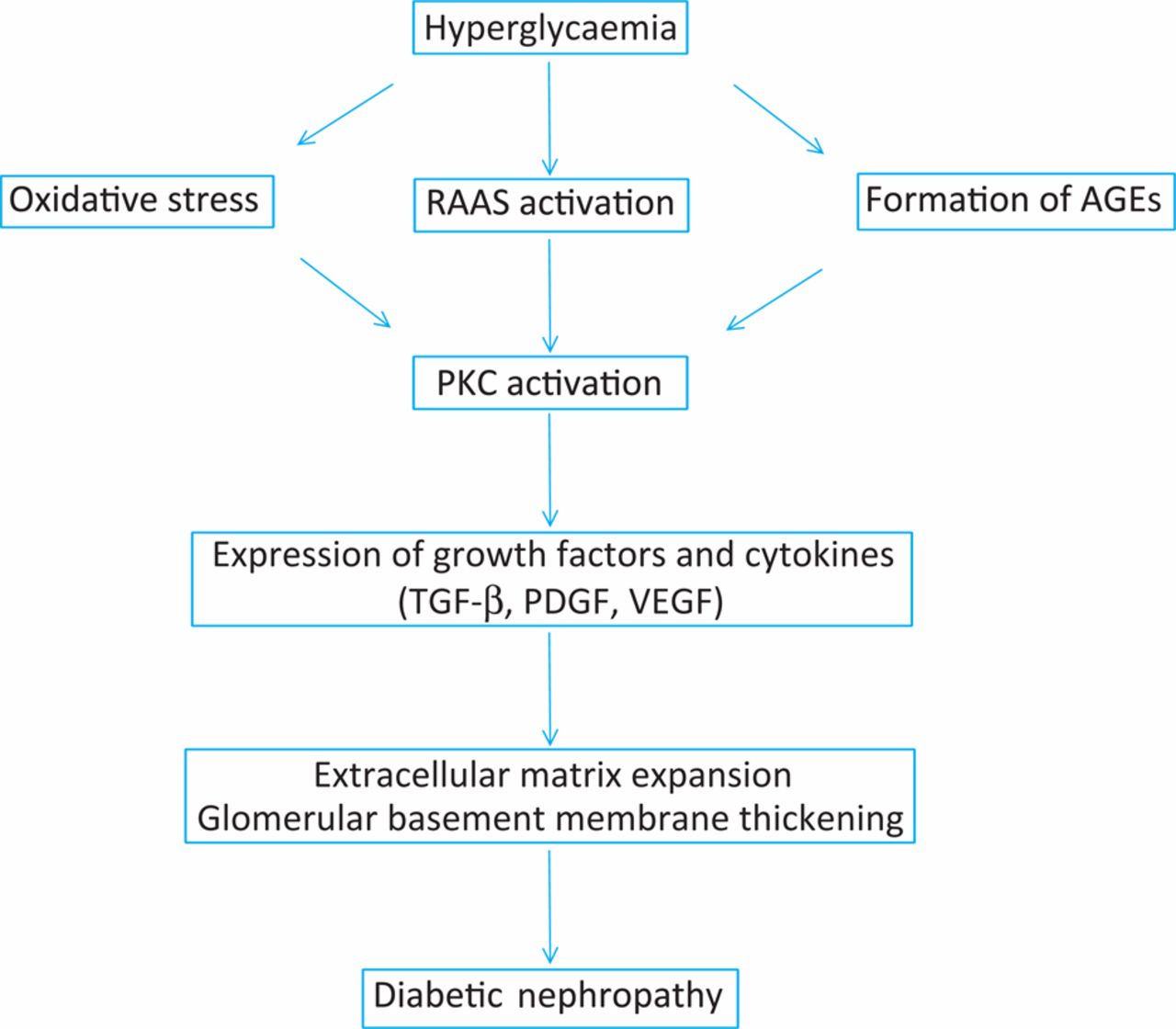
Simplified scheme for pathogenesis of diabetic nephropathy. AGEs = advanced glycation end products; PDGF = platelet-derived growth factor; PKC = protein kinase C; RAAS = renin–angiotensin–aldosterone system; TGF = transforming growth factor; VEGF = vascular endothelial growth factor

Glomerular haemodynamic changes in diabetic nephropathy: (a) normal glomerular capillary pressure and glomerular filtration; (b) glomerular capillary hypertension, glomerular hypertrophy and hyperfiltration associated with angiotensin II-mediated efferent arteriolar vasoconstriction; (c) development of microalbuminuria associated with thickened but ‘leaky’ glomerular basement membrane. Ang = angiotensin; BP = blood pressure; GFR = glomerular filtration rate.
A recent meta-analysis confirms that hyperfiltration is associated with the future risk of developing DN.5 The pathogenic role of glomerular hypertension and hyperfiltration is underlined by the efficacy of drugs blockading the renin–angiotensin–aldosterone system (RAAS) such as angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs). Blunting the profibrotic effects of angiotensin II may also be a significant factor in the benefits observed with these agents.
Natural history
The classic natural history of DN is described as a stepwise progression from a hyperfiltration phase via incipient nephropathy with microalbuminuria to overt nephropathy with persistent dipstick positive proteinuria, followed by progressive CKD, finally reaching ESRD. Typical histopathological changes include glomerular basement membrane thickening, mesangial matrix expansion, development of Kimmelstiel Wilson nodules and arteriolar hyaline thickening.
There are several clinical caveats to consider:
1. The natural history is predominantly based on follow-up of patients with T1DM.
2. Clinical trials have shown that it is possible to alter the natural history of DN by targeting multiple risk factors (eg achieving tight glycaemic control, aggressive treatment of hypertension and the use of ACEIs and ARBs).
3. Up to 30% of people with renal impairment and T2DM do not have DN but have another cause for their renal failure (eg hypertensive or ischaemic renovascular disease).
The natural history of DN in patients with T2DM is best described using data from UKPDS-64.6 The investigators measured the annual probability of transition from each stage of renal impairment and risk of death from all-causes or cardiovascular disease (Fig 3). The trial concluded that the proportion of patients with T2DM who develop microalbuminuria is substantial, with one-quarter affected within 10 years of diabetes diagnosis. Fewer patients develop macroalbuminuria, but the death rate in those who do exceeds the rate of progression to worse nephropathy.
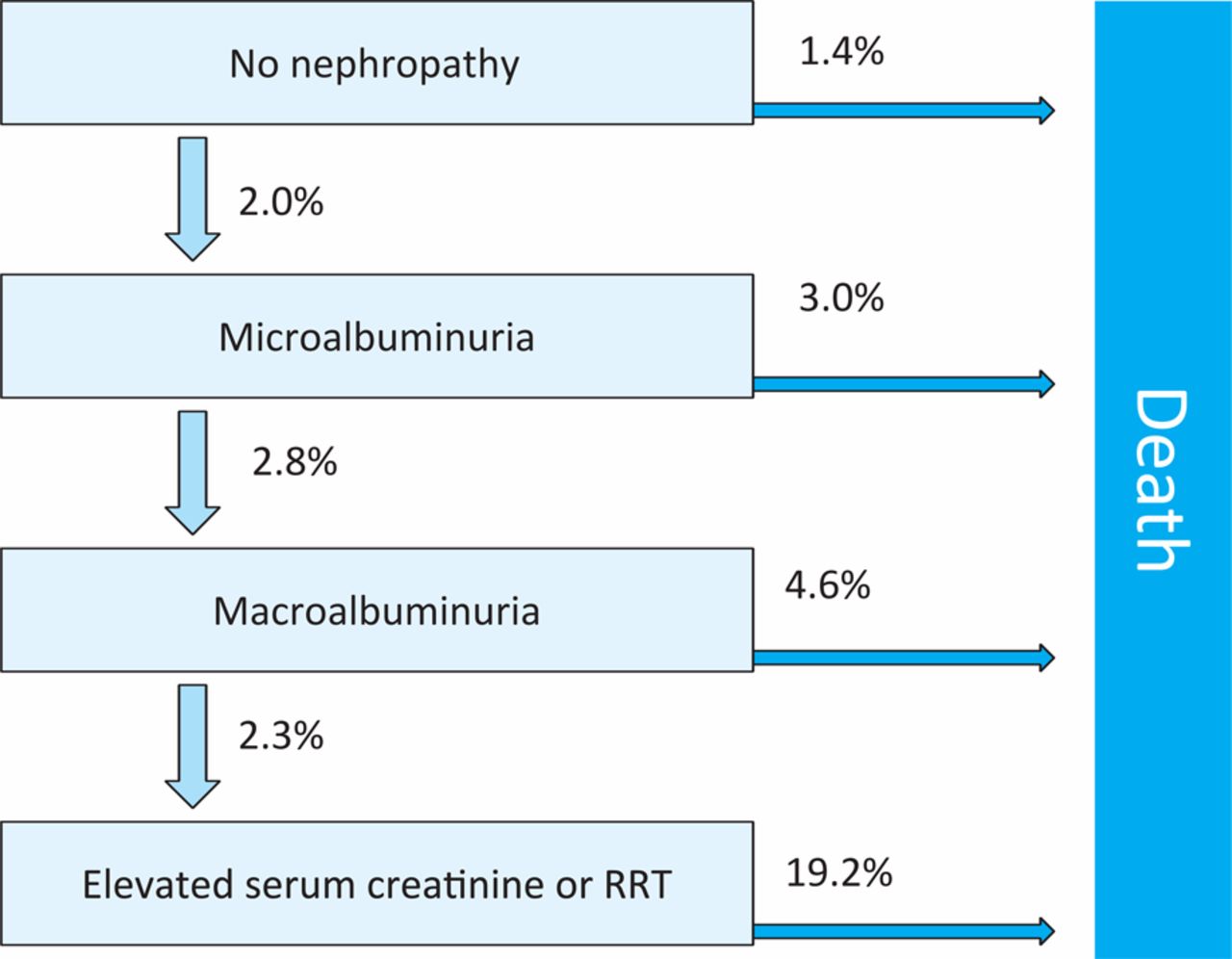
Annual transition rates through stages of nephropathy to death from any cause, as described in the UK Prospective Diabetes Study. RRT = renal replacement therapy. Adapted from Ref 6 with permission from Macmillan Publishers Ltd: Kidney International © 2003
The higher mortality is largely attributed to an increased risk of cardiovascular disease. DM, CKD and microalbuminuria are all independently associated with an increased risk of cardiovascular disease. Having all three significantly increases mortality risk. The Nord-Tr¿ndelag Health Study-2 (HUNT-2) study found that lower estimated (e)GFR categories were associated with increased relative risk of cardiovascular death.7
Treatment
Annual screening for microalbuminuria is recommended for patients with T2DM from the time of diagnosis as the duration of their diabetes will be unknown. For patients with T1DM, annual microalbuminuria screening is recommended from five years after diagnosis. BP treatment targets vary in different guidelines but we suggest targets of 125/75 mmHg for those with proteinuria over 1 g/24hr and 130/80 mmHg for those with less than 1 g/24hr. A reduction in protein excretion to below 0.5–1.0 g/24hr is recommended, although this can be difficult to achieve in practice. National Institute for Health and Clinical Excellence (NICE) management of T2DM guidelines8 identify management of lifestyle, glycaemic control, BP, albuminuria and dyslipidaemia as priorities for treatment.
Glycaemic control
Excellent glycaemic control can prevent the onset of microalbuminuria, reverse glomerular hypertrophy and hyperfiltration, and stabilise or decrease proteinuria in those with established DN. Intensive therapy to near-normal glycaemia can reduce the onset or progression of DN even in those with previous poor glycaemic control.9
Methods for HbA1c measurement are affected by renal failure, leading to falsely elevated levels. However, in those patients with advanced CKD other factors contribute to decrease in measured HbA1c, leading to an underestimate of glycaemic control, for example reduced red blood cell life span, recent transfusion, iron deficiency, accelerated erythropoiesis due to administration of erythropoietin and metabolic acidosis.
CKD is associated with insulin resistance, but the half-life of insulin increases as renal failure progresses and patients may need a reduction in total insulin dose, particularly those with reduced appetite associated with uraemia.
Oral hypoglycaemic drug therapy can also be challenging in diabetic patients with advanced CKD. Metformin is used with caution in people with CKD because of the associated risk of lactic acidosis. A dose reduction of 50% is suggested for those with an eGFR below 45 ml/min/1.73 m2. Patients should be advised to stop metformin when eGFR is less than 15 ml/min/1.73 m2 or during any periods of illness, dehydration or exposure to radiocontrast.
First-generation sulphonylureas, meglitinides, alpha-glucosidase inhibitors and thiazolidinediones should be avoided in advanced CKD (eg eGFR <30 ml/ min/1.73 m2) unless patients are under specialist care. Second-generation sulphonylureas are the agent of choice, but may also require dose reduction due to increased drug half-life.
Hypertension and microalbuminuria management
Non-pharmacological measures to reduce BP, such as salt restriction and weight loss, are important but if BP is above 140/90 mmHg antihypertensive drug therapy is appropriate. For patients with T1DM, an ACEI is first-line treatment or, if poorly tolerated due to cough or angioedema, an ARB. There is more evidence for the use of ARBs in T2DM, but in clinical practice ACEIs appear to have similar effects. Benefits of RAAS blockade include reduction in intraglomerular pressure and hyperfiltration, antifibrotic effects and endothelial stabilisation.
In patients with microalbuminuria or hypertension at all stages of nephropathy, an ACEI or ARB should be considered and uptitrated to achieve BP and proteinuria targets. Repeating a renal function test is advised one week after introduction or dose escalation; a creatinine rise less than 30% and a potassium level below 6 mmol/l may be accepted. Patients should be told to stop these drugs during any episodes of dehydration, intercurrent illness or exposure to radiocontrast.
The use of dual RAAS-blockade with an ACEI and ARB remains controversial. Compared with monotherapy, combined therapy can produce a greater reduction in protein excretion. Nevertheless, the recent ONgoing Telmisartan Alone and in Combination with Ramipril Global Endpoint Trail (ONTARGET) study reported that combining an ACEI and ARB in patients with vascular disease or high-risk diabetes, but without heart failure, did not reduce the risk of the primary outcome (death from cardiovascular causes, myocardial infarction, stroke or hospitalisation for heart failure) but increased the risk of hypotensive symptoms, syncope, hyperkalaemia, and renal failure requiring dialysis.10
Aliskiren is a direct renin inhibitor with similar efficacy to ACEIs and ARBs in lowering BP. When used in combination with an ARB it resulted in a 20% greater reduction in proteinuria, independent of effect on BP.11 Long-term safety and efficacy data are needed before routine use of aliskiren could be recommended.
Most patients with DN require multiple drugs to achieve BP goals. In those with volume overload, a diuretic will help enhance the antiproteinuric effects of RAAS blockade. Addition of calcium channel blockers can help to achieve BP targets. For those who remain proteinuric, a non-dihydropyridine agent such as diltiazem may reduce intraglomerular pressure and proteinuria. A pooled analysis of nine major clinical trials of DN12 confirmed that lower mean arterial pressures are directly correlated with reduction in the annual loss of GFR.
Simultaneous targeting of multiple clinically modifiable risk factors for DN has proved to be a successful prevention strategy. Prolonged follow-up of the STENO Diabetes Centre (STENO-2) study participants demonstrated that intensive intervention with multiple drug combinations and behaviour modification in at-risk patients with T2DM had sustained beneficial effects with respect to DN, vascular complications and cardiovascular and all-cause mortality.13 Treatment goals for the intensive therapy group included BP below 140/85 mmHg, HbA1c below 6.5%, use of ACEI irrespective of BP, and aspirin in those with cardiovascular risk.
Novel agents
Various other novel agents for the treatment of DN and reduction in proteinuria are currently being investigated including fibrates, fish oils, vitamin D analogues and peroxisome proliferated activated receptor-gamma agonists.
Referral
Referral to specialist renal services should be considered in accordance with local and national NICE CKD guidelines.14 Indications for referral include:
eGFR less than 30 ml/min/1.73 m2
rapidly deteriorating renal function
sustained increase in serum creatinine (>30%) after starting an ACEI or ARB
uncontrolled hypertension on three agents
nephrotic range proteinuria, or
if another non-diabetic glomerular disease is suspected.
Another renal diagnosis should be considered if retinopathy is absent in T1DM or if there is sudden onset of nephrotic range proteinuria, haematuria or rapidly declining renal function.
Timely referral for those approaching ESRD is imperative to ensure adequate individual planning for renal replacement therapy: that is, dialysis or transplantation (kidney or combined kidney and pancreas).
Summary
The earliest sign of DN is the development of microalbuminuria which is associated with a significant risk of both progressive renal failure and premature death from cardiovascular disease. Optimal glycaemic and BP control, including the use of RAAS blocking drugs, can prevent, slow and even reverse the processes causing DN.
- © 2010 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}