
Key Points
Type 2 diabetes (T2DM) has an increased risk of cancer; patients need to receive lifestyle advice to reduce this risk
Metformin is protective against cancer in observational studies and should be considered for first-line treatment in T2DM and continued alongside other therapies if possible
Further studies are needed to investigate whether analogue insulins increase the risk of cancer
Vigilance of new therapies may need to be extended to many years to ensure there is no increased cancer risk
Type 2 diabetes (T2DM) is associated with a greater incidence of cancer, particularly of the pancreas, breast and colon.1 This association may be multifactorial, possibly linked to obesity, insulin resistance or hyperglycaemia. For example, carcinoma of the colon is associated with obesity, hyperglycaemia, metabolic syndrome, hypertriglyceridaemia, insulin treatment and raised insulin-like growth factor (IGF) levels.2
Diabetes therapies
Metformin
Therapies used to treat patients with diabetes may increase or decrease their cancer risk. Population-based cohort studies support this, showing a higher cancer-related mortality in those treated with insulin or sulphonylureas compared with patients on metformin therapy.3 This may be due to a harmful effect of the sulphonylurea and insulin therapies or to a protective effect of metformin. Pilot studies from a diabetes database suggest the latter.4 The potential mechanism is that metformin activates adenosine monophosphate-activated protein kinase which may suppress tumour formation.
Insulin analogues
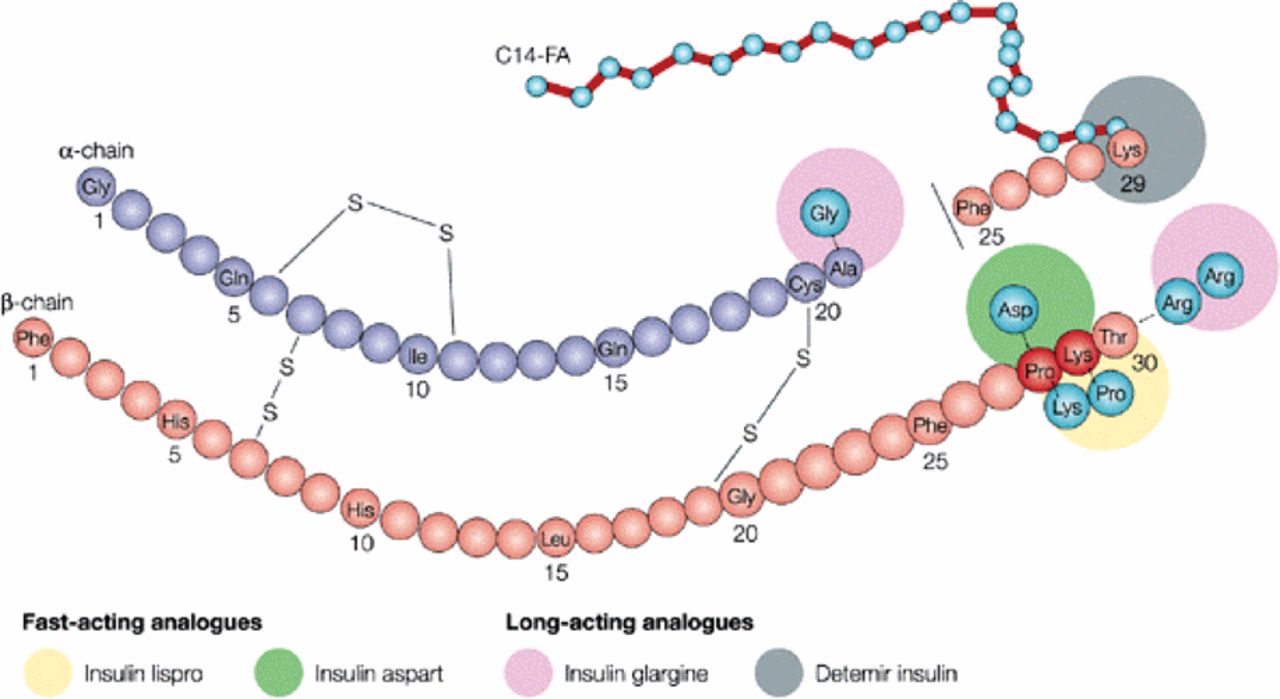
Intermittent exogenous insulin replacement is frequently unable to meet the challenging physiological demands in patients with diabetes, resulting in both hyperglycaemia and hypoglycaemia. The analogue insulins were developed with various modifications of human insulin by substitutions of amino acids and additions to delay or increase the rate of insulin absorption and to prolong or shorten activity (Fig 1). The analogues are divided into short- and long-acting compounds (Table 1). In England, insulin aspart is the most frequently prescribed short-acting insulin and insulin glargine the most frequently prescribed long-acting insulin (Fig 2).6 If these insulins increase mitogenicity, this may have a significant impact as most patients would be expected to remain on them for many years and have protracted exposure.
Insulin analogues.
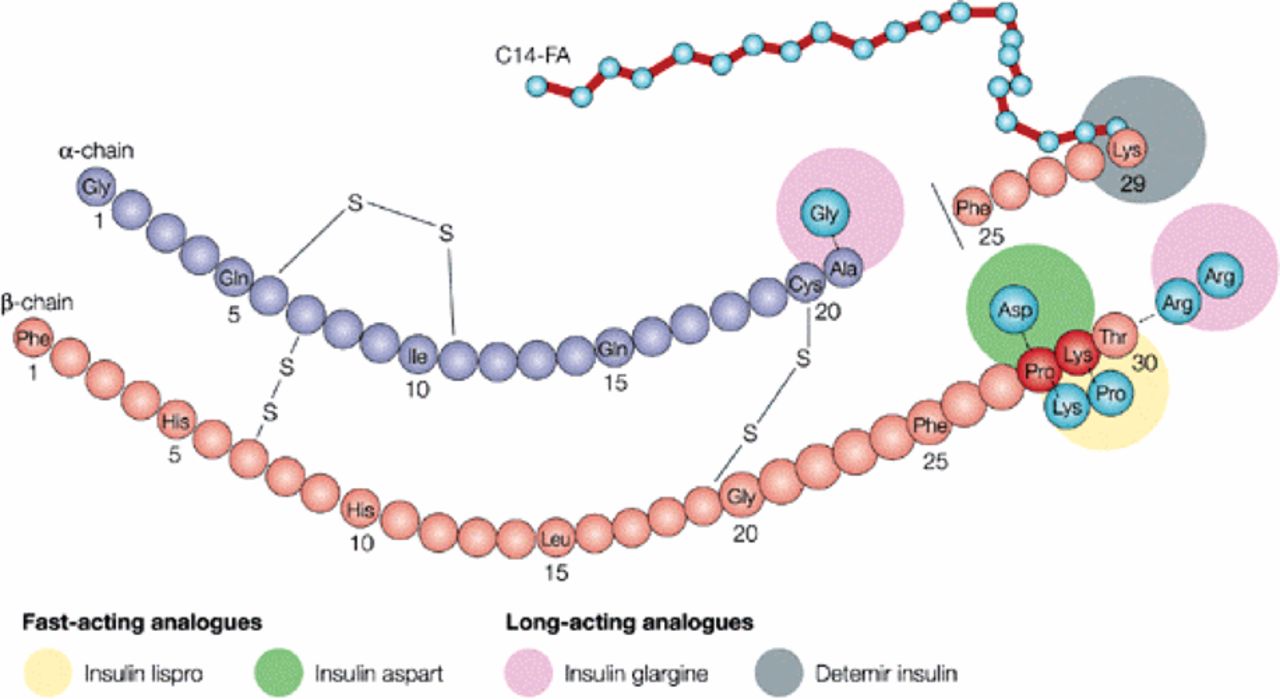
Development of analogue insulins with modifications of human insulin to alter the rates of insulin absorption and activity. Reprinted with permission from MacMillan Publishers Ltd: Drug Discovery © 2002.5
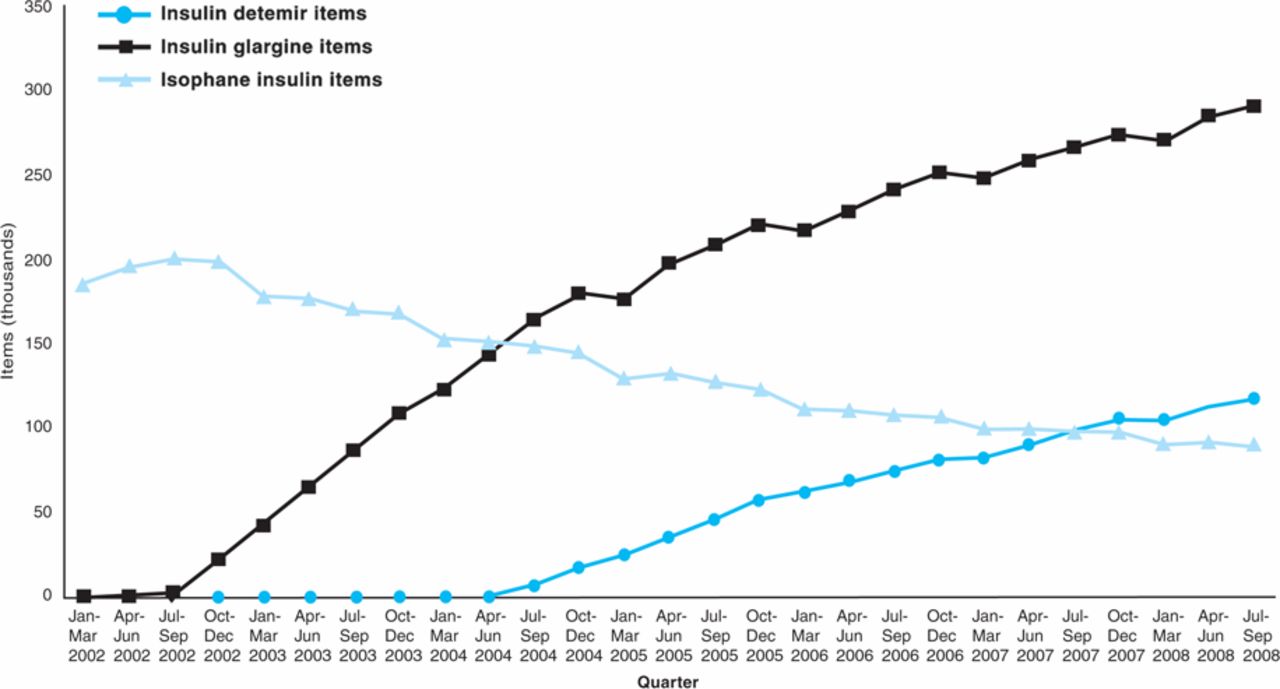
Since 2002 there has been a rising trend to prescribe insulin glargine and a fall in prescription of human insulin. Reproduced with permission from Ref 6. Copyright © 2009; The Health and Social Care Information Centre.
Insulin analogues and development of cancer
There are theoretical explanations why insulin analogues may promote growth of cancer cells. If the binding affinity is increased for the insulin receptor or for IGF-1 receptor this may increase the rate of tumour growth. Some in vitro studies7 have shown that insulins glargine, detemir and lispro have a proliferative and anti-apoptotic activity in cultured cancer cells. Insulin glargine has a six- to eightfold increase in IGF-1 receptor affinity.8
The first analogue to be developed, insulin B10Asp, was withdrawn during development due to a dose-dependent increase in mammary adenocarcinomas in rats.9 This molecule had a sixfold increase in affinity for the IGF-1 receptor and slow dissociation from the insulin receptor which theoretically may have increased mitogenicity.
Observational studies
Four retrospective observational studies were published in 2009 which had investigated the association of insulin analogues with cancer.10–13
An observational study of a large patient cohort10 raised concerns about the safety of insulin glargine. This isolated publication may have resulted in a harmful and unjustified abandonment of a widely-used treatment. A special advisory group was convened to review the findings,14 with the result that three further investigations into this subject were commissioned.11–13
German study. The original German study10 examined data collected for insurance purposes. Four different insulins were studied (insulins glargine, lispro and aspart, and human insulin) with co-administration excluded. There was a correlation between insulin dose and cancer risk. In the unadjusted analysis human insulin had a greater risk of cancer, but adjusting for dose reversed this risk and showed a dose-dependent increased risk of malignancy with insulin glargine compared with human insulin. The addition of metformin or other oral hypoglycaemic agents did not reduce this risk.
This study has been criticised for potential ‘reverse causation’: those in the insulin glargine group may have had a lower insulin dose and higher glucose levels deliberately as they were considered to have greater frailty and greater comorbidity, including potential cancer. In addition, patients with both T1DM and T2DM were included. It is unlikely that those with T1DM would be on insulin glargine alone but may have been receiving human insulin alone or a short-acting analogue alone (via a pump). This may have resulted in a higher proportion of patients with T2DM in the insulin glargine group. Patients with T2DM have a greater incidence of insulin resistance and therefore a greater cancer risk.
UK data. In the UK, cancer risk in those on monotherapy with metformin or sulphonylurea and those on different insulin regimens were examined in data collected from primary care for the Health Information Network.11 This study demonstrated an increased risk of solid tumours for treatment with both insulin and sulphonylurea compared with metformin.
It should be noted that there was no absolute increased risk ascribed to these treatments, only in comparison with metformin. Moreover, the addition of metformin to either sulphonylurea or insulin ameliorates the increased risk. There was no increased risk of cancer in analogue insulin compared with human insulin. Metformin lowered the risk for pancreatic and colonic cancer but not for breast or prostate cancer.
Scottish study. The national diabetes database was used to investigate the subject in Scotland.12 Patients treated with insulin were divided into those receiving insulin glargine alone, insulin glargine plus other insulin (various human and analogue insulins), and insulins without glargine. Overall, there was no increase in cancer risk with insulin glargine compared with those not receiving it. Subset analysis showed a higher incidence of cancer and a higher rate for breast cancer in those treated with insulin glargine alone compared with insulin glargine plus other insulins. The patients on insulin glargine alone were older and had worse glycaemic control. This may again reflect allocation bias, with less healthy patients receiving once daily insulin glargine as it is a simple regimen with a lower risk of hypoglycaemia. If exposure to insulin glargine is harmful, it is difficult to postulate how adding other insulin may reduce this risk.
Swedish study. A Swedish study used national registers to compare different insulin regimens divided as in the Scottish study.13 There was an increased risk of breast cancer in those on insulin glargine alone compared with women using other insulins. Again, if there is a harmful effect of insulin glargine, there seems no clear explanation why there should be more breast cancer in the insulin glargine alone group compared with the insulin glargine plus other insulins group. Again, allocation bias cannot be excluded.
Meta-analysis of trials. A meta-analysis of randomised controlled trials sponsored by the manufacturer to investigate whether insulin detemir increased the risk of cancer showed no evidence of increased risk.9 The overall incidence of cancer in the meta-analysis was low, probably due to the inclusion criteria for most trials actively excluding malignant disease.
Discussion of study findings
There has been a cautious response to the inconsistent findings in these studies. It is widely acknowledged that there is no proof of causation where association exists. Allocation bias is likely and could be prevented only by a randomly allocated study. There was also a short exposure time to the insulins; this would be unlikely to suggest a causal association between insulin and cancer but may suggest promotion of occult malignancies. Other confounding effects may be previous treatment exposure to oral hypoglycaemic agents and differing national practices to detect occult malignancy (eg breast cancer screening programmes).
Cancer risk in less established therapies
The potential for increased cancer risk is not confined to the more established therapies. Some of the newer therapies to treat T2DM have been investigated for increased mitogenicity. These newer agents have not yet been linked with any case reports of cancer, but a protracted exposure may be required before this would be seen and vigilance must be maintained.
Sitagliptin
The effects of sitagliptin, a dipeptidyl peptidase-IV inhibitor, and metformin on β-cell function were examined in an animal model. There was an increase in ductal cell turnover and ductal metaplasia, both of which are risk factors for the development of pancreatic cancer.15 The addition of metformin prevented ductal cell proliferation.
Liraglutide
Studies in mice and rats given liraglutide, a glucagon-like peptide-1 (GLP-1) receptor agonist, showed an increased risk of thyroid c-cell focal hyperplasia and c-cell tumours which may suggest an increased risk of medullary cell thyroid cancer. However, there appear to be differences in thyroid physiology between the rodent models and man. Specifically, c-cells are much more abundant in the rodent thyroid and express the GLP-1 receptor which, on stimulation, generates cyclic adenosine monophosphate, ultimately leading to calcitonin release. Calcitonin is used clinically as a biomarker for medullary cell thyroid cancer and, in all patient trials to date, has remained in the normal range.16
Conclusions
The main conclusions to draw are that T2DM is associated with cancer and that there are sufficiently strong signals to warrant further investigation into the potential mitogenic effects of analogue insulins and the potential adverse effects of the newer therapies.
The potential beneficial antitumour effects of metformin are attracting interest in the world of oncology. There is no evidence that established practice should be altered. Metformin is the first-line therapeutic agent to be considered for the treatment of T2DM in most published guidelines. There is good evidence of cardiovascular benefit from metformin therapy.17 The evidence considered here suggests a protective effect of metformin against cancer, thus strengthening the case for metformin to be considered as a first-line therapeutic agent in T2DM and to be continued alongside other therapy where possible.
- © 2010 Royal College of Physicians








{kind=link}
{kind=link}