
Introduction
Within the NHS the introduction of a statutory duty of quality in 1999 followed by clinical governance, national standards and regulatory frameworks have represented major steps towards delivering good quality healthcare. Most recently, government policy has shifted its focus away from targets and activity towards patient experience and outcomes. Lord Darzi's High quality care for all and the ‘quality and productivity’ agenda are initiatives that have sought to embed quality at the heart of NHS healthcare delivery.1,2 The recent government white paper Equity and excellence: liberating the NHS emphasises the importance of outcomes and a commitment to producing quality standards.3 These are to be defined through an NHS outcomes framework. In order to deliver and manage quality, it is necessary to measure it, which demands a conceptual framework within which to understand the term.4
Quality
Quality is a concept that describes those features of a product or service to which value is ascribed. Consequently, the nature of quality varies between products and services, individuals and organisations. Here it is discussed in relation to its significance within healthcare. Quality does not incorporate any idea of relative cost. Although it may be used in conjunction with cost, allowing consideration of value, the implementation of quality should not be seen as a cost-cutting exercise.
Given the subjective nature of quality, defining ‘high quality’ healthcare provision is challenging. It is not surprising that various healthcare organisations differ in their interpretations and consequently have defined it in different ways.5 The Institute of Medicine (IoM) sees quality as ‘the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge’.6 However, in order to define quality by the development of expectations or standards, it is necessary to ascribe dimensions of quality, also known as domains.7
Different organisations opt for various numbers and combinations of these domains. In the report Crossing the quality chasm the IoM expanded on its previous statement, listing six fundamental domains of quality: safety, patient experience, effectiveness, efficiency, equity and timeliness.8 In his Next Stage Review, Lord Darzi called for high quality care for all that is ‘personal, effective and safe’.1 The US Quality Assurance Project goes further, defining nine domains of quality: access, technical performance, effectiveness, efficiency, interpersonal relationships, continuity, safety, choice, and physical infrastructure and comfort.9 The Royal College of Physicians (RCP) has adopted a definition of quality which comprises patient experience, safety, effectiveness, efficiency, equity, timeliness and sustainability (Box 1).
The domains of quality used in the RCP definition of quality.
Despite the apparent variability in the number and nature of the domains ascribed, certain areas seem consistently important. A document released in March 2006 by the Organisation for Economic Co-operation and Development aimed to draw together domains of quality from the frameworks of six member countries and three international health organisations. Effectiveness, safety, patient experience, efficiency, equity and accessibility were the most frequently incorporated.10
It is of note, though perhaps not surprising, that many of the domains of quality, particularly those most frequently used, can be easily mapped onto the established four principles of medical ethics: autonomy, justice, beneficence and non-malfeasance.11 Thus, in many respects, the delivery of quality healthcare not only has ethical implications, but potentially constitutes a moral imperative.
In the evolving social, economic and political contexts of healthcare delivery, certain domains may be considered more pertinent at certain times. Interactions between different domains are inevitable and, while some of these will be synergistic, attempts to fulfil all of them may lead to tensions developing, especially in a resource-limited environment. The relationship between the domains of patient experience and equity is a ready example. Where tensions exist, the outcome that maximises quality should be sought. It may be necessary to make decisions regarding the relative importance of certain domains.
Quality improvement
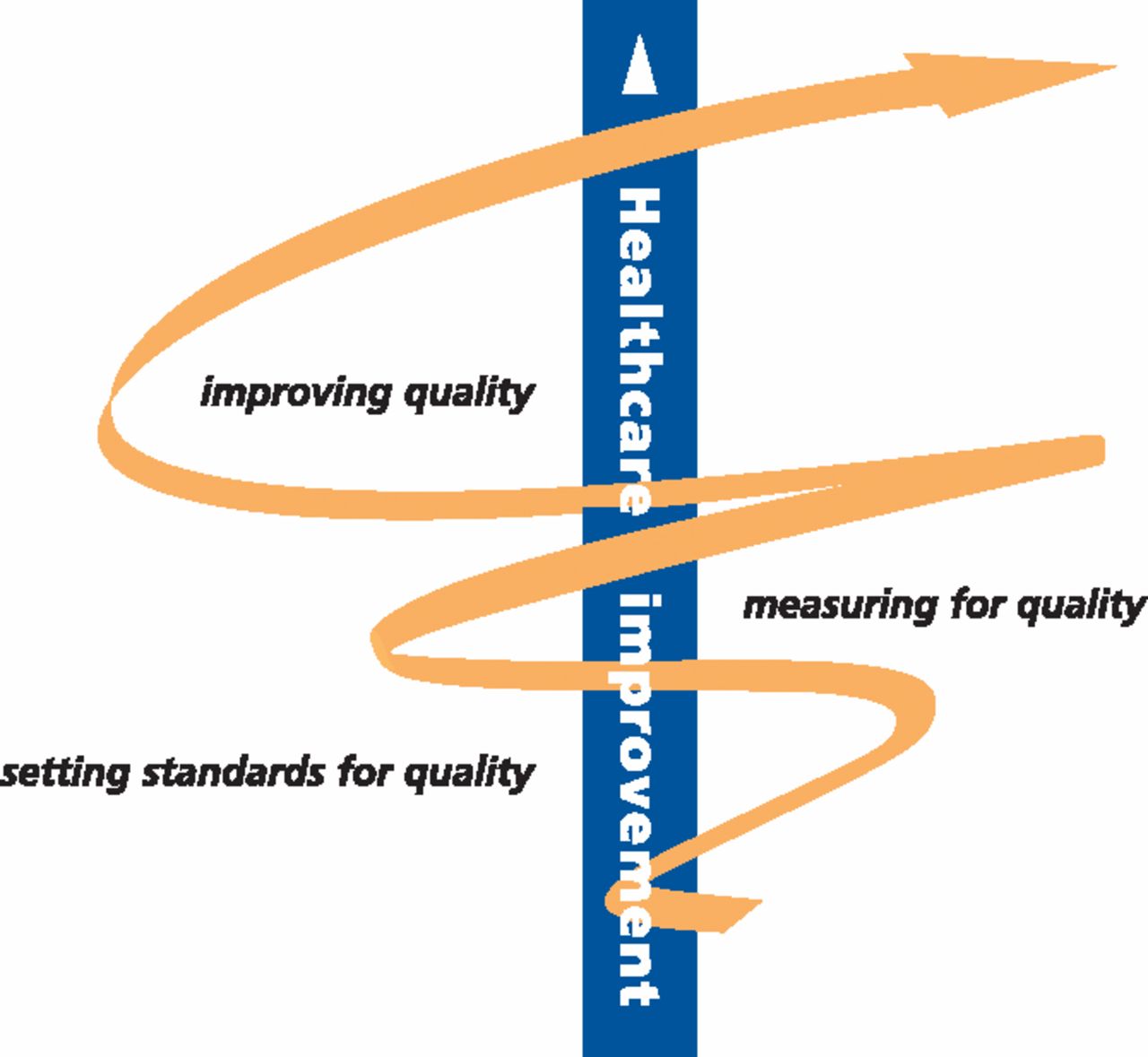
Quality is not a static concept; there is a need for continued improvement. High quality healthcare cannot be delivered by systems and institutions content to rest upon their laurels – this indicates the importance of the science of quality improvement. The ‘quality improvement spiral’ illustrates the basic principle (Fig 1).

The RCP quality improvement spiral.12
Improving quality is about making healthcare safer, more effective, patient-centred, timely, efficient, equitable and sustainable. Single changes can demonstrate improvements across multiple domains. For example, getting it right first time, through a reduction in error and harm, will not only improve patient outcome and satisfaction, but will also make care more effective and efficient.
Until recently, the science of quality improvement (QI) was not well understood in healthcare; the majority of workers' understanding of quality came from quality assurance (reliance on regulation and inspection to improve the delivery of care). Most QI approaches were developed in industry and have since been adapted for healthcare. Although most health professionals will have a scientific background, this tends to focus on the search for new knowledge; the applied science of QI has significant differences.
The domains of quality improvement.
The key elements of QI are a change (an improvement) and a method (techniques and tools). Improvement is about change and action based on experience. Individuals and teams combine a threshold for action with a readiness to develop and test ideas, and to make changes to protocol. Improvement is aspirational, future-focused and applied in complex clinical systems, unlike pure research, where variables are controlled. There are several methods, all of which are founded on a science concerned with understanding variation and the application of statistical methods and behavioural principles.13 Given the wide range of operational environments in healthcare, changes must be context specific. Each team works differently and implementation requires a strategy specific to the setting.
QI measurement techniques include the use of small, rapid tests of change in real-time, and time series data for internal learning and monitoring progress. Improvement science also supports the delivery of learning from clinical audit, benchmarking and clinical research – how knowledge from a variety of sources is made real in the clinical setting.
Two key factors prevent knowledge becoming isolated in pockets of excellence. The first is the ability to spread innovations and new and improved practice across clinical teams and healthcare systems. The second is the ability to sustain the change over time and to resist the temptation to revert to inferior practices.
The need for clinician engagement
The Department of Health has recently commissioned the National Institute for Health and Clinical Excellence to produce a series of quality standards, the measures against which quality of clinical services will be judged. Clinicians rightly see themselves as guardians of healthcare quality; they must involve themselves in the determination of quality standards. Additionally, learning how to plan, deliver and measure improvements in complex systems will be a crucial skill for all doctors. Clinical leaders who can develop teams to deliver change and reliably improve quality, will influence both system performance and patient outcomes.14
- Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- Building resilient health systems in Africa beyond the COVID-19 pandemic response
- Environmentally sustainable emergency medicine
- A pathway to net zero emissions for healthcare
- Making healthcare and health systems net zero
- Sustainability in quality improvement: redefining value
- Infrastructure - the key to healthcare improvement
- Reducing the carbon footprint of hospital-based care
- Quality Versus Costs: A False Paradigm
- Does Shared Decision-Making Provide an Opportunity to Improve the Outcome of Peritoneal Dialysis Catheter Insertion?
- Learning from practice variation to improve the quality of care
- Assessing the health benefits of tackling climate change