
Abstract
Ambulatory emergency care (AEC), ie managing emergency patients without an overnight hospital stay, offers an alternative to routine hospital admission and improved patient experience. The Directory of ambulatory emergency care for adults identifies 49 clinical scenarios which present acutely but could potentially be managed in an ambulatory manner. The Society for Acute Medicine and the NHS Institute for Innovation and Improvement conducted a national survey of 131 UK acute hospitals to understand the current level of AEC provision. Seventy-nine per cent of respondents indicated their site provided some AEC, but the number of conditions covered was limited and AEC tended to be ad hoc and informal at most sites. Weekend access was limited. Only deep vein thrombosis ambulatory protocols were well-established (65%), with other conditions formally implemented as ambulatory pathways at 0–35% of responding sites. There is a significant opportunity for further expansion of AEC through increased awareness and support.
Background
Access to emergency care in the NHS has improved considerably over the last decade, with most acute trusts consistently achieving the four-hour access time. However, medical admissions are continuing to increase.1,2 This places an emphasis on clinicians and hospital managers to ensure that only those patients who actually require admission to a hospital bed are admitted, and that their length of stay is commensurate with their acute care needs. Ambulatory care offers an alternative to routine hospital admission and studies suggest that patients often prefer this form of care.3–6 The current UK definition of ambulatory emergency care (AEC) is supplied in the Royal College of Physicians Acute Medicine Task Force Report:
clinical care which may include diagnosis, observation, treatment and rehabilitation, not provided within the traditional hospital bed base or within the traditional outpatient services that can be provided across the primary/secondary care interface. In the context of acute medicine, it is care of a condition that is perceived either by the patient or by the referring practitioner as urgent, and that requires prompt clinical assessment, undertaken by a competent clinical decision maker.7
The Directory of ambulatory emergency care for adults8 was published by the NHS Institute for Innovation and Improvement in 2007 and identifies 49 conditions or clinical scenarios which present acutely, where there is potential for ambulatory care. The directory outlines the potential range of opportunity for the ambulatory management of each condition. In a minority of cases, eg deep vein thrombosis (DVT), there are well-established ambulatory pathways in many hospitals; however, for others the current standard for care remains primarily on an inpatient basis.
The Royal College of Physicians of Edinburgh's UK consensus statement on acute medicine9 suggests that acute medicine allows ‘alternatives to hospital admission to be fully explored including the use of urgent outpatient referrals, intermediate care, ambulatory care, palliative care and end of life care’. It also states that ‘explicit standards must be set for acute medicine including: rapid assessment, the development of patient pathways, ready access to diagnostic services, treatment and effective discharge arrangements’. These practices are entirely consistent with those required to deliver AEC.
The benefits of AEC include improved patient experience, reduced risk of hospital-acquired infection by avoiding inpatient admission, and improved use of resources through reduced inpatient bed occupancy. It also has a key role to play in providing cost-effective approaches to improving quality of care in the NHS.10
Delivering AEC is a goal for acute medicine therefore the Society for Acute Medicine (SAM) and the NHS Institute have collaborated to develop a joint questionnaire-based survey to study existing AEC provision in acute medicine in the UK. This includes assessing existing pathways, how they are being delivered, what benefits and challenges have been encountered and exploring preferred support mechanisms for future ambulatory care pathways.
Subjects and methods
Questionnaires were administered, using two modalities (paper and electronic), to SAM members. The questionnaires were identical and based on current national guidelines.7,8 A paper-based questionnaire was disseminated during the national SAM conference (May 2009) to conference delegates, including medical staff and allied professionals (although the majority of attendees were acute physicians). A further electronic reminder (and access to an electronic version) was subsequently circulated to SAM members. Where duplicate results were received, one was removed with priority given to responses from consultants and completeness of response.
Results
There were 161 individual responses to the survey. Forty-eight responses were from duplicate hospital sites, and once all duplicates had been removed 113 responses were analysed. These responses were from 92 acute trusts, which represents approximately 48% of all acute trusts across England, Scotland, Wales and Northern Ireland (there are 155 acute trusts providing adult emergency care in England; 14 major accident and emergency (A&E) units in Wales; nine acute hospitals in Northern Ireland; and 14 health boards in Scotland, for a total of 192). The following results were received per region; Northern Ireland (1), East Midlands (4), East of England (6), North East and West Midlands (7 each), Wales (8), Scotland, South Central and South East Coast (9 each), London and Yorkshire and Humber (11 each), and North West (20).
The vast majority of responses were from doctors (92%); 65% of the responses were from consultants. The majority of these consultants were acute physicians (due to the nature of the conference and the SAM membership).
Ambulatory emergency care adoption
The majority of respondents indicated that their hospital site provided some AEC services, although 17% of responding sites do not (Fig 1). The majority of sites (55%) describe AEC services as operating within a range of specialty services (ranging from respiratory to A&E), with just under a quarter (24%) describing a single coordinated service.

Does (your) site provide any ambulatory emergency care services?
Table 1 lists the ambulatory care pathways in use, the stage of the pathway involved and whether a protocol was in place or in development. Respondents were asked to distinguish at which stage of the patient's care, ambulatory management was available: pre-diagnosis investigation (eg while awaiting a specific diagnostic), early treatment (ie early management of the condition) and/or early discharge (to enable an earlier discharge than traditionally anticipated). Respondents were also asked whether a protocol was in place to guide the ambulatory care or whether protocol development was underway.
Reported provision of ambulatory emergency care services by condition.
The top conditions currently managed in an ambulatory manner are DVT, transient ischaemic attack (TIA) and cellulitis. Responses indicate that hospitals are managing patients in an ambulatory manner across all stages of the patient journey, from pre-diagnosis investigation, early treatment through to early discharge, depending on the patient's clinical condition and stability (as the figures across the first three columns are fairly consistent). Most interest was expressed in developing AEC protocols for pulmonary embolism, cellulitis, falls and anaemia.
Ambulatory emergency care delivery
Respondents indicated that ambulatory care is most commonly an integral part of the acute medical unit (AMU, 45 sites) with the day care unit being the next most common (Fig 2). The size of these designated ambulatory care areas varied but ranged from two to 12 trolleys, with an average of four chairs or beds.
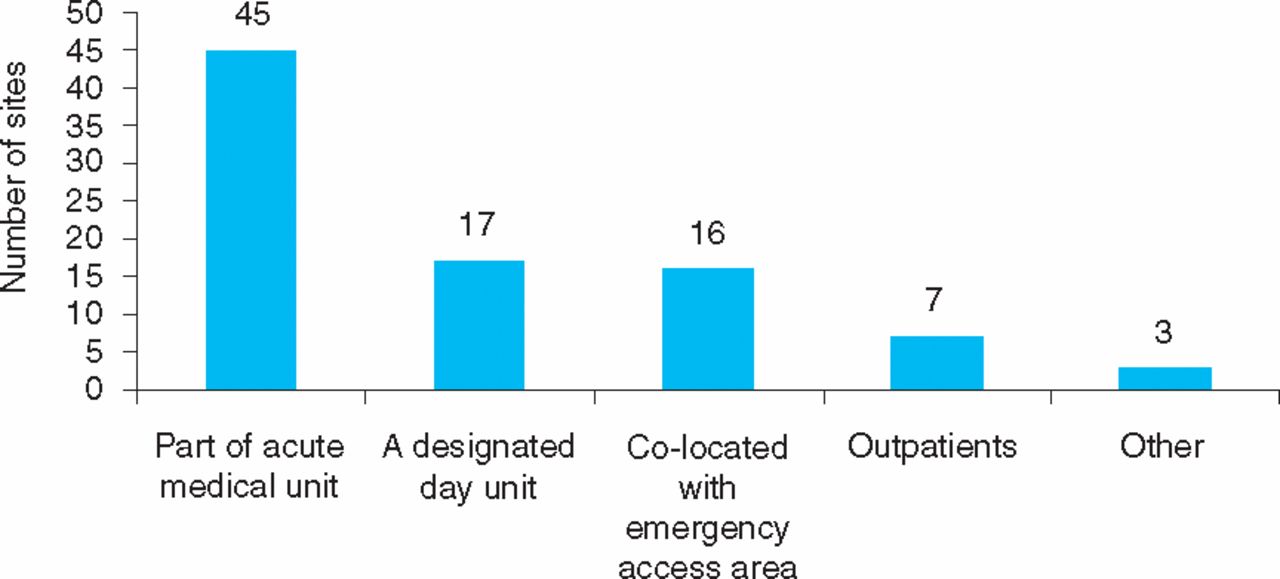
Location of ambulatory emergency care patient services.
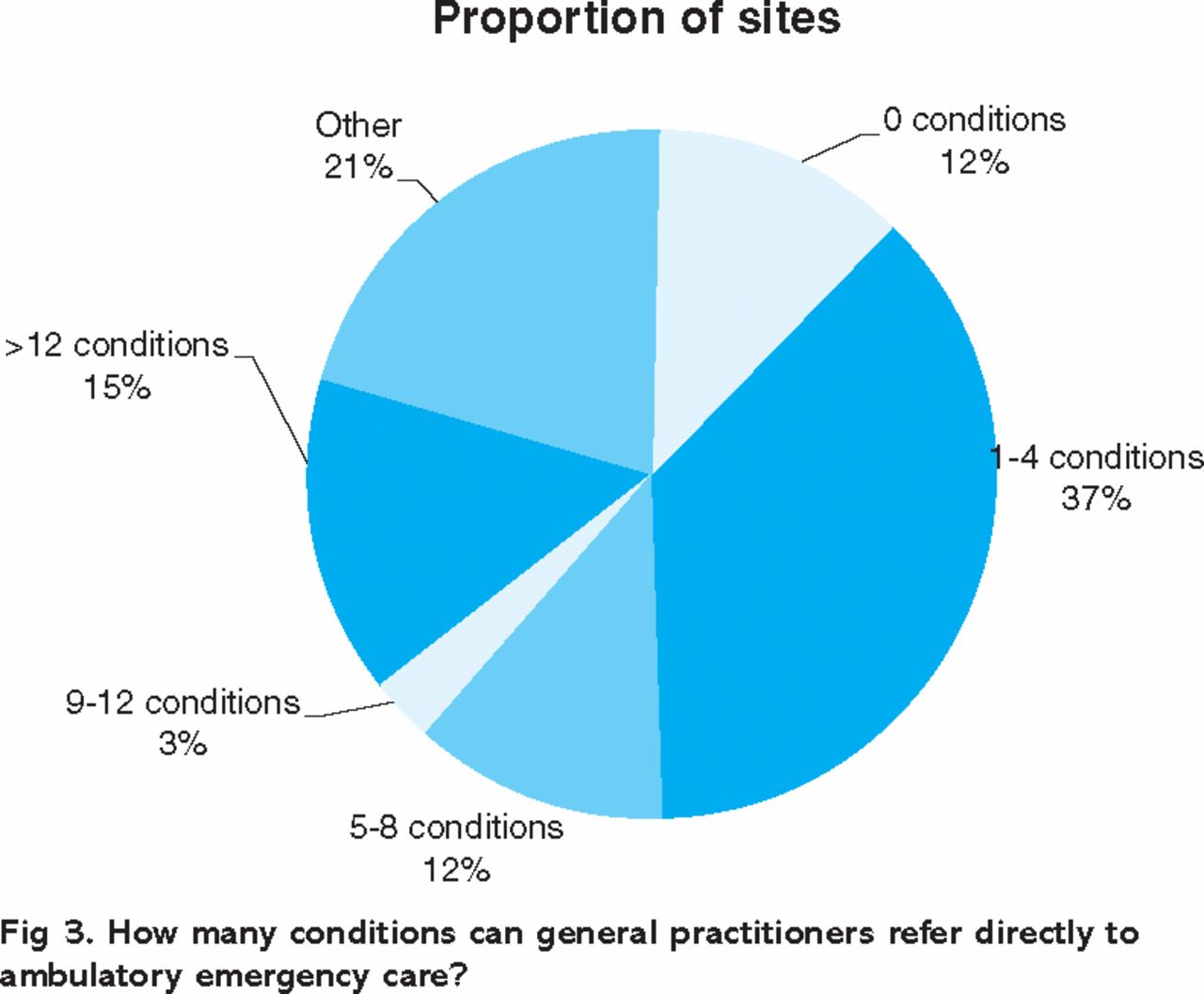
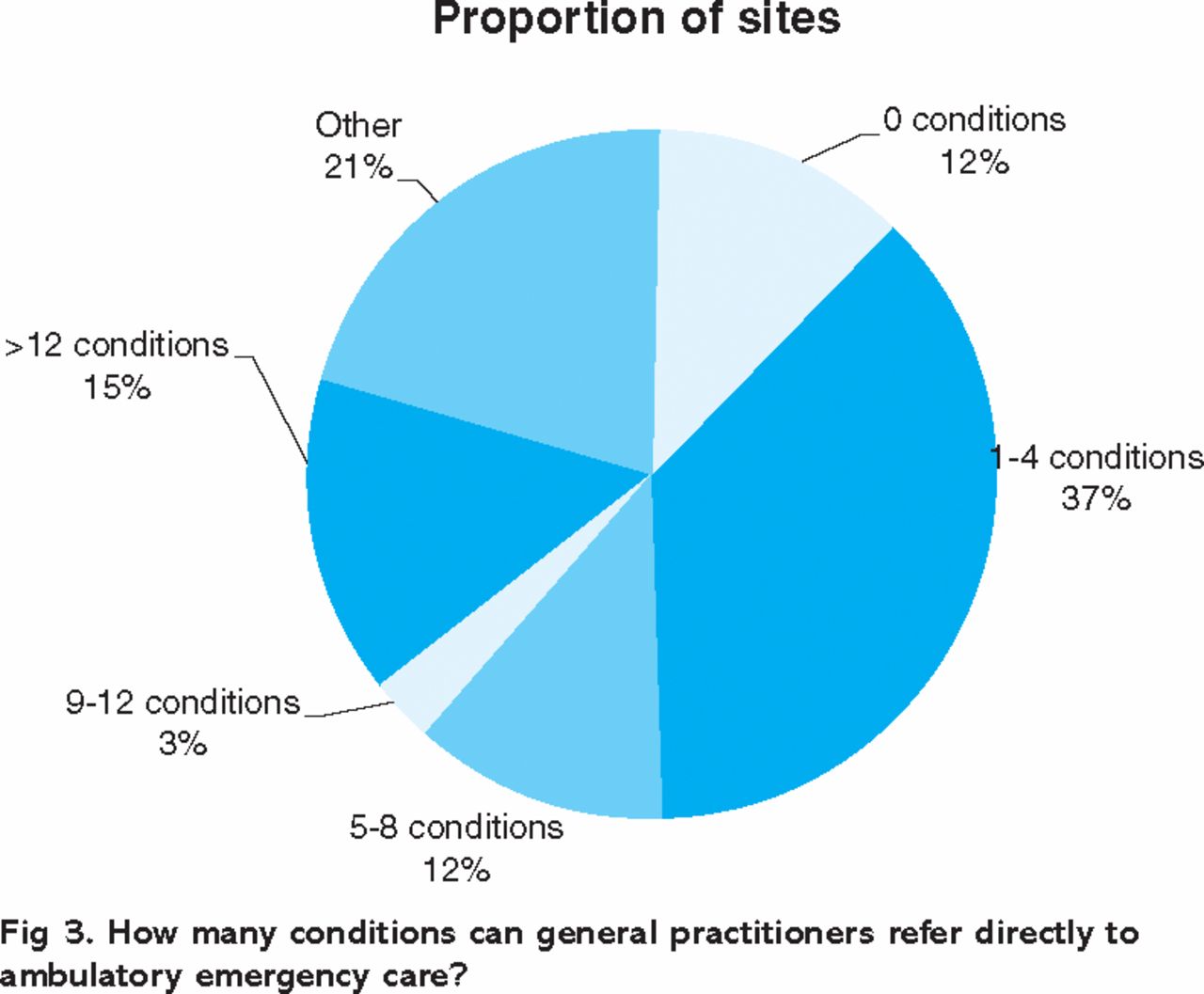
How many conditions can general practitioners refer directly to ambulatory emergency care?

Access times for ambulatory services.

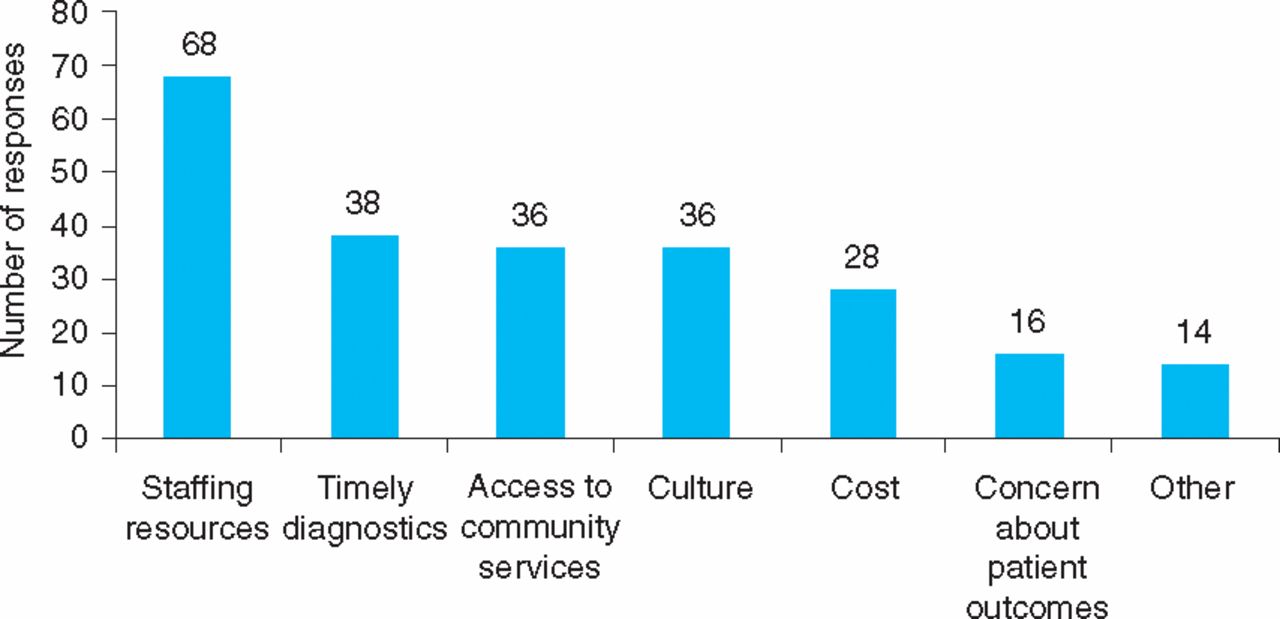
Perceived barriers to implementing ambulatory emergency care.

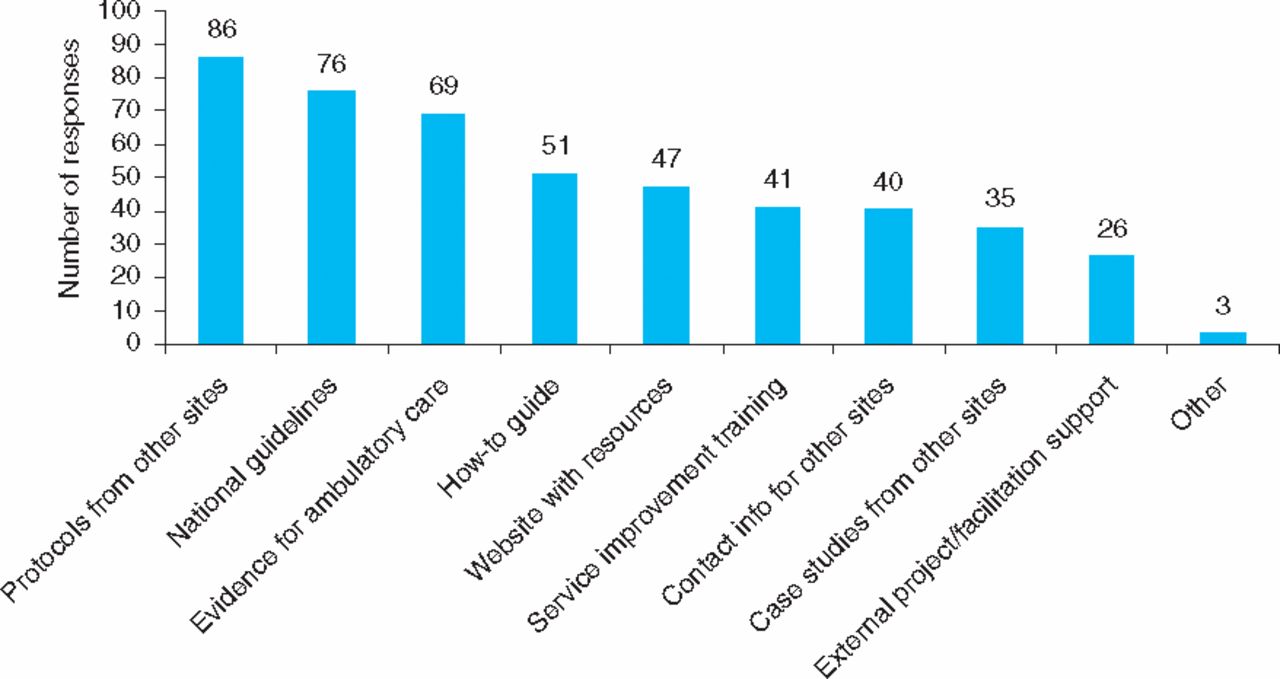
Additional support which would facilitate expanding ambulatory emergency care locally.
Access to ambulatory emergency care services
The majority of responding hospital sites supported direct general practice referral for one to four conditions. The majority of ambulatory care services were only available during standard working hours on week days.
Implementation and adoption considerations
Several implementation-related questions were included to explore why levels of adoption of AEC appear low and how these can be addressed. Staffing resources to lead and deliver AEC services were cited most commonly as the greatest barrier to their adoption, with concern about patient outcomes featuring less prominently. Other comments on key factors were:
involvement of primary care and primary care trusts
buy-in and integration between acute medical units and the specialties
advanced skills for nursing staff
improved planning of pathways
financial incentives for ambulatory care
seven-day working to improve access
a ‘can-do’ organisational culture.
Respondents indicated a clear preference for three support mechanisms: ambulatory emergency protocols from other sites; national ambulatory emergency guidelines; and evidence for AEC (including information about the financial impact and patient experience). Comments also included suggestions for:
internal management support for staffing and a designated area for providing care
establishment of regional and national networks of acute physicians.
Discussion
The results of this first questionnaire-based review of AEC in the UK suggest that the majority of acute trust hospital sites provide a limited amount of AEC services – most commonly for DVT – and that there remains a significant opportunity in the NHS to expand its provision that could be based on the Directory of ambulatory emergency care for adults8 and supported by the development of common protocols.
While 79% of survey respondents indicated that their hospital provided some degree of AEC, there was variation as to the range of conditions provided, the consistency of services available and how structured the processes were for delivering them. The percentage of ambulatory pathways that respondents claimed to have in place is higher than the percentage of actual ambulatory protocols in use, suggesting that the provision of ambulatory care, aside from fairly well-established ambulatory DVT services (65% of sites had an ambulatory DVT protocol in place), has a tendency to be ad hoc and informally delivered. Where duplicate responses were received from the same hospital site (48 responses) these were reviewed for consistency of responses – respondents from the same sites tended to have identified different sets of established AEC protocols, suggesting both ambiguity about the concept in general and a lack of formal arrangements in many cases. The survey authors have subsequently collected a number of ‘ambulatory care’ protocols from sites around the UK, a portion of which are actually inpatient protocols as opposed to specific ambulatory care protocols. Again, this suggests a lack of understanding about the concept of AEC and lack of an organisational focus on developing this aspect of care.
While the AMU appears to be the most common area for coordinating AEC, most sites do not describe an integrated process as suggested in current national guidelines.7 Given the nature of the conditions outlined a more systematic approach should improve efficiency and provide a more cost-effective system.
Similarly, the range of services offered is as yet not extensive, with direct general practice access to services only routinely available for one to four conditions (from the 49 possible clinical scenarios identified in the directory8). In addition, most services were only available during standard working hours on weekdays but even where sites offered weekend services the range was limited, for example one site provided seven-day ambulatory DVT services but its ambulatory chronic obstructive pulmonary disease services were only available from Monday to Friday. This does not support improved bed utilisation at weekends which impacts on diagnostic services on Mondays and may lead to unnecessary weekend admissions.
There are many clinical and financial benefits to be realised by the health system through increased provision of AEC services (and the fact that existing protocols tend to cover all stages of patient assessment and management indicates that there are even greater potential benefits in terms of beds and patient experience to be gained through their implementation, ie through increased consistency of care for all patients, including those who have to be admitted).
Staffing resources were cited by a significant number of respondents as a barrier, which suggests that the cost-effectiveness of shifting care from the acute setting to an outpatient or community setting through AEC services has yet to be clearly understood across the NHS. The NHS England Payments by Results tariff structure under HRG 4 includes a reduction for short stay as it did under HRG 3.5, which may be considered by acute trust finance teams as a disincentive to the development of AEC. A move towards a tariff structure akin to that which has been developed for day case surgery would provide an appropriate structure for the development of AEC. Despite the fact that staffing resources were considered the greatest barrier, the supportive measures cited were in many cases relatively cost-neutral, including national guidelines, protocol-sharing and a clear evidence base of the financial and quality benefits of implementing ambulatory emergency care.
The study suggests that although AEC is happening to some extent in the acute care setting, and is supported by national recommendations, it is not yet routine in the UK. Although protocols exist they are not uniform and there are few agreed standards of care. Overall the results suggest ambulatory care is happening but there is a desire to develop ambulatory care in a more systematic fashion. This would be facilitated by the development of national AEC guidelines and clear evidence about health economic benefits, clinical outcomes and patient experience. Protocols would provide guidance particularly for junior staff, regarding the utilisation of alternative investigation and treatment options. Developing a structure and a robust evidence base would facilitate more widespread adoption of ambulatory care. The implications of this study include a clear need to raise awareness of AEC, including national health policy level considerations about the existing financial incentives or disincentives to develop cost-effective models of care.
Conclusion
This survey suggests that there is a general enthusiasm for the concept of AEC but that implementation and understanding of the process is variable. There is significant interest in the development of national guidelines which would reduce the ‘reinventing the wheel’ process with multiple units writing similar protocols. In addition, there is support for national guidance in relation to the financial implications and developing evidence of positive patient experience. In conclusion, AEC offers an alternative to the traditional admission process, which in turn offers financial benefits and a potential reduction in hospital-acquired infection.
- Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}