
Abstract
During their careers, most general physicians are involved in the decision-making process for patients that potentially require percutaneous endoscopic gastrostomy (PEG) insertion. However, poor patient selection and less than favourable outcomes are frequently observed in this group. With the aim of identifying and addressing the underlying issues, the PEG service at University Hospital Llandough was radically changed over an eight-year period. The development of a nurse-led pre-assessment service and design of a specific referral form was successful in reducing the number of PEG referrals and consequently the 30-day mortality rate. Furthermore, the educational and training needs of general physicians of all grades regarding the issues surrounding PEG placement were identified and addressed at formal teaching sessions. A combination of these factors has positively impacted on our service, with more appropriate patient selection and a reduced 30-day mortality rate.
Introduction
Percutaneous endoscopic gastrostomy (PEG) feeding is used as long-term enteral nutrition for patients unable to maintain sufficient oral intake, with the decision to place a PEG often made by a general physician responsible for the care of the patient. After insertion, the 30-day mortality rate is significant, estimated at up to 28%.1 The nature of the underlying condition and poor patient selection are likely causes of this high mortality rate, as highlighted by the 2004 National Confidential Enquiry into Patient Outcome and Death (NCEPOD) report, where it was stated that 19% of PEGs were deemed futile.2 In particular, patients with advanced dementia were identified as receiving no long-term benefit from PEG feeding. Complications arise from inappropriate patient selection often relating to their fitness to undergo the procedure due to frailty or acute illness, including chest infection.2 Recognised indications for PEG insertion include neurological disorders of swallowing, head injury, mechanical obstruction and long-term partial failure of intestinal function.3 Complications include bleeding, intestinal or colonic perforation, infection and tube displacement. The risk of complications can be reduced by ensuring appropriate patient selection through pre-assessment and high standards of aftercare of both the patient and gastrostomy tube.
The University Hospital Llandough (UHL) is part of the Cardiff and Vale NHS Trust with 480 beds and a busy unselected medical intake of approximately 12,000 patients per year. Historically, clinicians at UHL referred patients for PEG insertion without any input from the gastroenterology department. Patients were often seen for the first time by the endoscopist in the procedure room immediately prior to the procedure. There were no uniform standards for patient selection, with large numbers of ‘inappropriate’ referrals and PEG placements. As a result, some would be deemed unsuitable by virtue of co- morbidities or be too unstable to undergo endoscopy and so would be returned to the ward. There was also inadequate preparation for the procedure or aftercare. There was no specific undergraduate or postgraduate training on PEG insertion and the surrounding issues. In order to develop a service that resulted in better patient selection, a multidisciplinary approach was established. In particular, knowledge deficits and training issues among doctors commonly involved in referral, discussion and preparation of patients needed to be addressed. The impact of these changes on the pattern of referrals and mortality rates from 2001 to 2009 were therefore reviewed. The knowledge of referring clinicians of different grades about PEG insertion, indications, contraindications, procedural complications and consent were also assessed.
Methotitles
Nursing pre-assessment
Pre-assessment of all referrals by a nutrition nurse specialist (NNS) was introduced in 2001. It was implemented with the aim of decreasing the number of inappropriate PEG referrals as well as optimising the status of suitable patients pre-procedure. All referrals were reviewed on the ward by the NNS who, where appropriate, liaised with the family and referring teams. In particular, she assessed the indication for PEG, the patient's co-morbidity and current health, contraindications as well as technical issues such as their ability to lie flat and open their mouth. Those deemed unsuitable for PEG insertion were discussed with their medical team and consultant gastroenterologists.
At the same time, patient information leaflets, information stickers for the medical notes and the standard advice on provision of PEG aftercare were commenced. All patients referred for PEG insertion and their relatives were provided with written and verbal information about the procedure. To optimise patient care, a checklist to be undertaken before the procedure was inserted into the case notes. This included measurement and correction of international normalised ratio, intravenous (iv) access, consent and antibiotic prophylaxis in the form of a single dose of cefuroxime 750 mg iv prior to the procedure.4 After the PEG was placed, the endoscopist put a second information sticker into the notes with detailed after-care advice. The NNS visited each patient on the ward to provide staff with advice regarding the care of the gastrostomy tube, such as pushing the tube in and rotating it after the first two weeks. Patients were reviewed on a weekly basis until discharge by the NNS or on request.
The information about patients referred for a PEG insertion between October 2001 and September 2006 was obtained from records kept by the NNS as well as patients' medical notes and the hospital's computerised patient management system. The total numbers referred each year, those inserted successfully, unsuitable referrals, failed procedures and 30-day mortality rates were measured. Prior to the introduction of the outreach service in 2001, very little data were collected on the number of PEGs inserted, mortality or complication rates. The numbers inserted using the endoscopy reporting system for the three years prior to the introduction of the pre-assessment service were obtained, and then the 30-day mortality rates were recorded by using the hospital computer system and accessing patient case notes. Information on the indications, failed procedures and reasons for mortality were not available for this time period.
Implementation of referral form
In 2006, a specific PEG referral form was designed to augment the pre-assessment service, based upon a form implemented in Sheffield in 2004.1 Although an overall reduction in the number of referrals for PEG insertion was observed between 2001 and 2006, a proportion were still deemed unsuitable after review by the NNS. In an attempt to address this, the referral form was introduced which included additional information for referring doctors to aid them in the decision-making process about suitability for PEG insertion. Ethical issues, such as advanced dementia, an assessment of the patient's fitness for procedure, consideration of co-morbidities, contraindications to the procedure and the need to carry out a mini-mental state examination, were added to the form.
Education issues
Soon after the introduction of the new referral form in 2006, a questionnaire was undertaken to assess the knowledge base of doctors from foundation year 1 to consultant level who were involved in referring and caring for patients requiring PEG placement. Junior doctors of all specialties were asked to complete the questionnaire at core teaching and senior members of the team at medical meetings. The questionnaire was sent via internal mail to consultants, requesting them to return the completed questionnaire to the department.
The impact post-intervention
The final part of the study was to ascertain if the pre-assessment service in combination with the referral form and teaching sessions had decreased the number of PEG insertions, inappropriate referrals, failed procedures and 30-day mortality rate. Mortality data from the three years prior to the introduction of pre-assessment and then after intervention were analysed, and data from 2001–6, prior to the referral form and new teaching sessions, was then compared to the data from 2007–9 to determine if there was a significant reduction in any other parameter over the study period.
Statistical analysis was undertaken using the chi-squared test for 2 × 2 tables to analyse the differing proportions of outcomes, and a Fisher's exact test when the number of subjects was <5. All analyses were performed using the SPSS statistical software package, version 14 (SPSS Inc, Chicago, IL).
Resultitles
Nursing pre-assessment (2001–6)
In total, 477 patients were referred for PEG insertion from October 2001 to September 2009 (Table 1). In the three years prior to nurse pre-assessment, 52/155 patients died within 30 days of their PEG placement, compared to 44/218 after pre-assessment until September 2006. This is highly statistically significant (p=0.003). In the first year of pre-assessment, 25% of patients referred were deemed unsuitable for the procedure (Table 2). The breakdown proportions of reasons for an unsuitable referral have remained similar over the five-year period after nursing assessment was introduced, and the pattern of indications for PEG insertion are largely unchanged. By far the largest group of indications were neurological diseases with the primary indication being cerebrovascular accident (CVA), which is in accordance to the NCEPOD data.2 The data show a small number of patients with head and neck cancer having a PEG inserted. It is important to note, however, that the data are on inpatients alone and a high number of outpatients coming in for PEG insertions have head and neck cancer.
Overview of percutaneous endoscopic gastrostomy (PEG) referrals, numbers of suitable and unsuitable referrals and failed procedures between October 2001 and September 2009.
Indications, reasons for unsuitable referrals, failed procedures and causes of death up to 30-days post-procedure between October 2001 and September 2009. * unable to open mouth, extensive previous gastric surgery, unable to maintain oxygen saturations; **eg stricture; *** eg hiatus hernia, other pathology found – gastric cancer. CVA = cerebrovascular accident; PEG = percutaneous endoscopic gastrostomy.
Table 1 shows that on a yearly basis, the total number of referrals up until September 2006 do not greatly differ. In 2002, there was a reduction in the number of referrals which may reflect the medical team's previous interactions with the nutrition nurse.
The most common cause of failure of the procedure was an inability to site the gastrostomy due to prior gastric surgery, hiatal hernia or oesophageal stricture (Table 2).
Implementation of referral form and education (2006–9)
After the referral form was implemented in 2006, it is possible to compare data with the five years of nursing pre-assessment to determine if there was any impact on referrals. The diagnostic group of dementia patients have shown a significant reduction in total referral numbers (p<0.002), however the reduction in numbers of patients deemed unsuitable referrals with advanced dementia was not statistically significant (p=0.490). The total reduction in the number of unsuitable referrals after implementation of the referral form did not quite reach statistical significance (p=0.061).
In the past year, the total number of patients being referred for PEG insertion has decreased, with only 38 referrals in 2008–9, almost half that of 2001 (Table 1). The number of insertions attempted (including failed procedures) compared to referrals has also decreased, with 66 in the first year of pre-assessment, and 26 in 2008–9, but this is not statistically significant (p=0.141).
The proportion of unsuitable referrals that were deemed inappropriate following discussion with the patients and their families and where other modalities of feeding were used (such as at-risk oral feeding) was found to increase after implementation of the referral form, and was statistically significant (p=0.018).
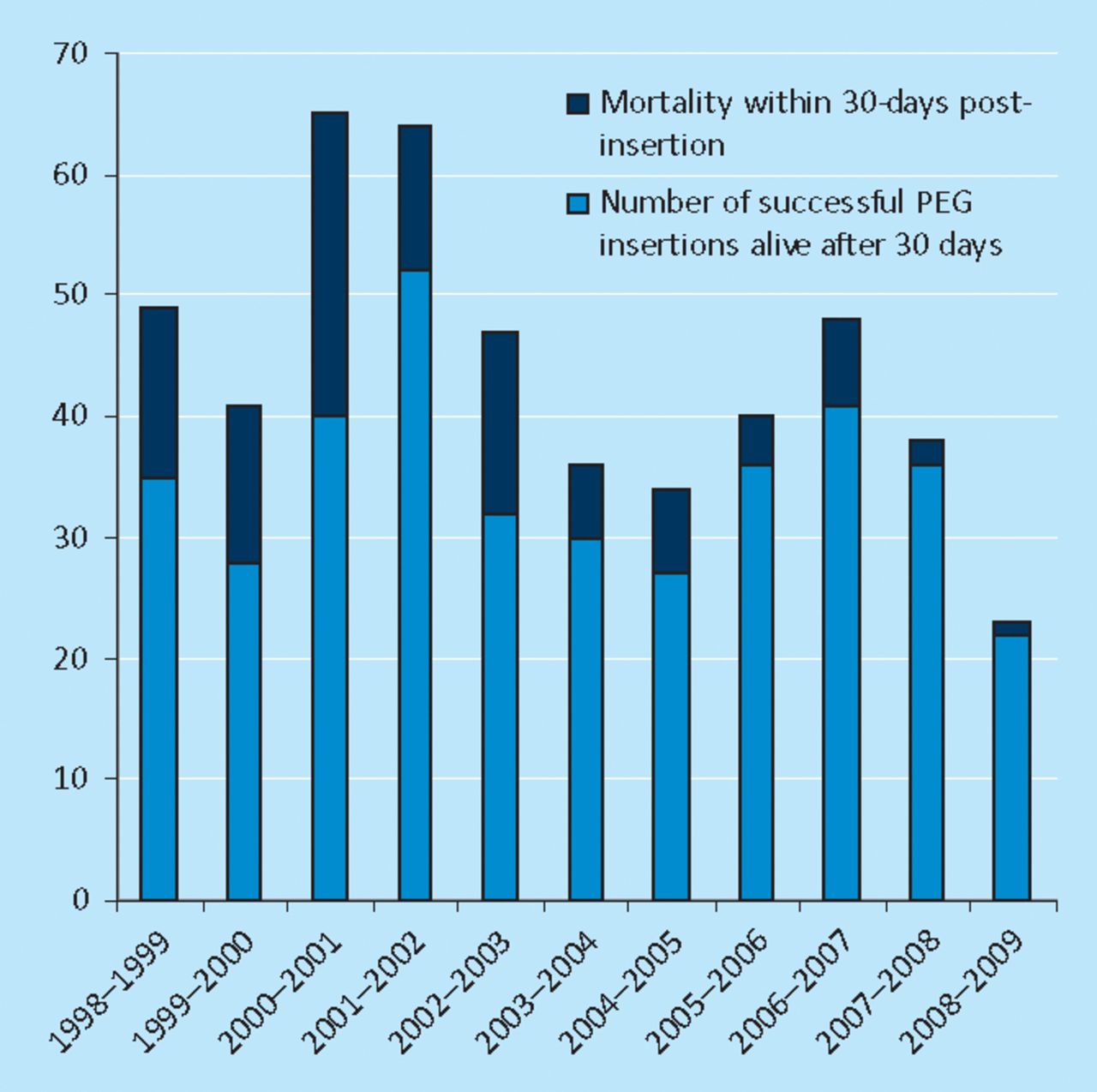
There is a positive effect of the referral form on 30-day mortality rates, which have reduced further after implementation of the form and education, compared to pre-assessment only (Fig 1). Again this is statistically significant (p=0.012). Causes of death in those patients that died within 30 days of PEG placement are given in Table 3, along with the time in days after PEG insertion that death occurred. The leading causes of death throughout the study period were caused by the underlying disease process (CVA) or by aspiration pneumonia.

Successful percutaneous endoscopic gastrostomy (PEG) insertions alive after 30 days compared to the 30-day mortality rate.
Causes of 30-day mortality post-percutaneous endoscopic gastrostomy insertion.
Education issues
Forty-six out of 58 (79%) questionnaires distributed between junior and senior doctors were completed. On average, each clinical team would refer only one patient for PEG placement during a four-month period. Consultants appeared to make the decision to refer for PEG (70%), the remainder being made by the specialist registrar. Conversely, it was the junior members of the team who completed the referral form, discussed the procedure with the patients and relatives (in 73%) and took patient consent (where appropriate) for the procedure (in 90%).
Just a quarter of junior doctors had witnessed a PEG insertion, compared to 83% of consultants. Knowledge of the procedure itself was poor across all grades of junior doctors. In total, 77% of the respondents claimed to have read some literature regarding PEG insertion and 89% were aware of the new specific PEG referral form. There was a poor response to identifying indications and contraindications for PEG, demonstrating an overall inadequate level of knowledge in junior doctors. However, 74% of the respondents did recognise that advanced dementia alone was not an indication for PEG, which is consistent with current literature.1
Discussion
The NCEPOD report highlighted the need for radical change to an endoscopy service that was often failing to deliver the best care for patients.2 This study shows that many issues needed to be addressed to improve the quality of the PEG service, avoiding poor outcomes and futile procedures. By introducing a pre-assessment service led by a dedicated NNS, a redesign of the literature and increased education of clinicians, there has been an appropriate reduction in the number of PEG placements undertaken and a significant improvement in the 30-day mortality rate. By far the largest group of indications is neurological diseases with the primary indication being CVA which in is accordance with the NCEPOD data.
PEG insertion incorporates several important ethical issues including the debate whether clinicians referring terminally ill patients for gastrostomy are ‘maintaining life or prolonging death’.5 The natural history of dementia may make it appear as if the patient is ‘starving to death’ and therefore it has previously been one of the most common indications for PEG insertion.1 This has caused much debate, as it has been suggested that a basic duty of doctors is to provide adequate nutrition for patients.6 However, several studies have found that PEG feeding this group of patients does not prolong their lives, with no increase in nutritional markers after tube placement.7–9 Henderson and colleagues identified that longer-term tube feeding was actually associated with weight loss.10 These complex ethical and legal dilemmas have been highlighted recently with the publication of new practical guidance from the Royal College of Physicians.11 A reduced number of patients with advanced dementia alone undergoing PEG insertion was demonstrated in our unit following the introduction of pre-assessment. To aid assessment of the patient's cognitive state, the mini-mental examination is included on the new referral form. It is important, however, to remember that many patients with early dementia and other co-morbidities may still benefit from PEG feeding.
It is difficult to determine the effect of the referral form compared to educational input, as they were implemented over the same time period. Unfortunately, as there were still a high number of inappropriate referrals observed, the referral form itself has not acted to prevent patients who clearly do not meet the criteria from being referred. However, the referral form can be viewed as a tool for the NNS to easily select those patients that are clearly inappropriate for PEG insertion. It is important to note that the cohort of patients in this study often represent difficult feeding issues that benefit from further specialist nutritional advice, and require liaison with medical teams and patients' families to reach a solution which best benefits the patient. Education sessions in addition to the advice and input given by the NNS in a variety of cases over time may plausibly have increased awareness of patient suitability for PEG insertions. It is extremely likely that all of the interventions implemented act cumulatively to reduce the numbers of inappropriate and futile PEGs being undertaken, so although there was a statistically significant increase in the proportions of unsuitable referrals who were trialled with other methods of feeding after 2006, this is entirely appropriate. The most important end point is the reduced 30-day mortality rates.
The General Medical Council (GMC) in their recent guidance, Tomorrow's doctors, have deemed that nutritional assessment be a core competency in undergraduate medical training and foundation grade training.12 In our hospital, knowledge deficits and training issues are also now being addressed via formal teaching on PEG insertion, especially for foundation grade doctors. This involves lecture-based teaching with a video of PEG insertion and discussion about the procedure and patient consent. All grades of doctors are invited to attend these sessions. They are also encouraged to liaise with the NNS when managing a patient that may be suitable for PEG insertion.
Information provided to the patient and family members is also an important consideration. Carey and colleagues reported that families' expectations of PEG feeding exceeded the outcome and that they often need more information about the procedure and possible consequences.13 Capacity to consent should also be assessed by the referring team prior to referral, as this will impact upon the type of consent form required and grade of doctor needed to obtain consent. This is of particular relevance in view of published GMC guidance,14 which states:
If you are the doctor undertaking an investigation or providing treatment, it is your responsibility to discuss it with the patient. If this is not practical, you can delegate the responsibility to someone else but they should be: suitably trained and qualified and have sufficient knowledge of the proposed treatment with risks involved.
Information regarding the potential risks of the procedure is included on the new referral form to aid junior doctors in obtaining informed consent, as in practice consent is often taken by the referring team on the ward and confirmed by the endoscopist prior to the procedure.
The development of a pre-procedure sticker ensures patients are adequately prepared, minimising last minute cancellations in the procedure room, which is distressing for the patient and their relatives. Improvement of aftercare has been achieved by a clear instruction sticker in the notes and follow-up by the NNS, which as a result has improved the standards of PEG aftercare by the ward staff.
Conclusions
Introduction of a nurse-led pre-assessment service coordinating a multidisciplinary approach to PEG insertion has led to an appropriate reduction in the number of procedures undertaken and improved the 30-day mortality rate compared to published data. A redesigned referral form has augmented the implementation of this change, bringing to the attention of the patient's medical team whether a request for PEG placement is clinically indicated, and acting as a tool for the NNS to easily identify patients who may not benefit from a PEG. By liaising with junior doctors and prompting discussion of complex cases, they are able to develop skills which can be used in patient care across a wide range of medical specialties in the future. This study has demonstrated that this approach has been effective in achieving better standards of care at UHL.
Acknowledgements
We would like to thank Drs Sarah Clarke and Noreen Khan for completing part of the audit regarding the knowledge of doctors on PEG placement, Rosie Crimmins for coordinating audit data, Dr Andrew Yeoman with his help with the statistical data and Dr D Sanders, consultant gastroenterologist, Royal Hallamshire Hospital, for permission to adapt his PEG referral form.
- Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.