
Abstract
This paper presents an analysis of the views and ideas generated at a recent health policy discussion for doctors in training. This provides an illustration of the creativity and enthusiasm that trainees can bring to the policy sphere by providing unique insights and a fresh perspective.
Introduction
Doctors willing to involve themselves in the formulation of health policy have tended to be rare. Among doctors in training, this seems to be shifting. Clinical leadership schemes for trainees, emerging following a call in Lord Darzi's NHS Next Stage Review,1 have proved popular. They have also provided an impetus for the development of a cadre of UK doctors eager to shape the future of the NHS.
A recent event at the Royal College of Physicians (RCP) gathered together doctors in training from national leadership schemes for an evening of debate. Participants represented all major specialties and stages of training. Discussion centred around three policy areas, chosen to reflect recent developments and future medical practice, and attendees were challenged to generate policy recommendations. This paper presents the views expressed and ideas generated as an indicator of the trainee perspective. They demonstrate the valuable role doctors in training can play in health policy development, providing unique insights and fresh perspectives.
The role of doctors in the social determinants of health
Estimates suggest 10% of variations in health are determined by medical care and 15% by social factors.2 Sir Michael Marmot's recent reports for the World Health Organization and the UK government have refocused attention on the social determinants of health.3,4 Despite efforts to address social factors, inequalities within the UK remain profound. Life expectancy for those living in the most deprived boroughs of England is, on average, a decade shorter than for those in the most affluent boroughs.4 Historically doctors have argued for societal reform to improve health. Given competing pressures on doctors today, what is their current role in addressing these social determinants of health?
The term ‘social determinants of health’ requires clarification. Discussion at this event contrasted ‘causes’ of disease, such as smoking, and ‘causes of the causes’, such as poor education. Most attendees felt that the medical profession should address the causes of disease, rather than merely treating the consequences. Whether the medical profession should routinely be addressing the ‘causes of the causes’ was more contentious. Some felt that doctors should focus their energy on areas where their influence alone is seen to be significant. Given time and financial constraints, others felt that involvement may perhaps be beyond the day-to-day remit of individual clinicians, but where time allows, evidence-based initiatives should be prioritised. Given the imperative to concentrate on cost-effective activities, attendees highlighted the need to develop tools able to assess impact and demonstrate cost-effectiveness of specific interventions. This is particularly important in order to demonstrate value and aid understanding of how to best utilise a specialist's skills and time.
Many attendees recognised the professional duty to improve health as engendering a requirement to articulate the causal link and the case for action on the social determinants of health, in their broadest sense. It was highlighted that doctors remain the most trusted among all professionals,5 and are viewed as highly influential members of society, and that this may confer a responsibility to use this influence to advocate for policy changes to improve health. Attendees felt that local and national clinical leaders may be best placed to take on this role on behalf of the profession. What part individual front-line clinicians should play remains unanswered. Prevention was widely considered by attendees a valuable use of doctors' time, often being more cost-effective than treatment and producing measurable benefits in health. It was also felt that opportunistic action within the doctor–patient relationship should be promoted. However, attendees felt less comfortable with recommending proactive action outside of these confines. The role of each specialty in acting on the social determinants of health may not be equal. However, few – if any – can claim social factors are irrelevant to their work.
As these debates continue, it is evident that there is a groundswell of interest in social determinants within the younger medical generation. Many doctors and medical students are keen to engage in these issues during training and clinical practice, recognising the importance of such work on health.6 It was suggested that opportunities to take on roles where specific projects may be undertaken and skills developed could be valuable. These could include secondments to primary care trusts or other organisations, including those outside of healthcare. The enthusiasm of these individuals offers the potential of significant health gains for society. Action is required to ensure these are fully realised.
Performance measurement and reporting
Quality is now the organising principle for NHS care, making the measurement and management of performance a live issue. Reports comparing the performance of different NHS trusts are now commonplace, including those on hospital standardised mortality ratios and methicillin-restistant Staphylococcus aureus infection rates.7 A precedent for publishing individual performance figures was set by cardiothoracic surgeons, yet this has not heralded the expected widespread adoption of such measures within medicine.8,9 While the benefits of measurement are recognised, consensus has not yet been reached on how and what to measure and how to publish the results.
Attendees saw the increasing prevalence of public reporting of the performance of organisations, teams and individual practitioners as inevitable. Across all sectors, public expectation and appetite for reporting and accountability is growing. Within the medical profession, reporting is increasingly recognised as a pre-requisite to a truly patient-centred healthcare service. However, attendees did not view public reporting as risk-free, with concerns relating to the quality and specifics of the data collected, in addition to ensuring accurate and fair analysis and presentation.
Trainees felt strongly that doctors and patients should be actively involved in the design and interpretation of public reporting schemes, to determine which measures should be reported and to assure confidence in the data. It was felt that while the process of data collection for reporting may be costly to trusts in the short term, there was significant potential to increase efficiency and value within organisations over the longer term.
Traditionally, individual clinician performance has been rarely scrutinised or reported on. Attendees urged careful consideration of the granularity of measures. Many argued that, especially in non-surgical specialties, team or service-based performance measurements may be more appropriate than those pertaining to individuals. Calibration of data was considered vital to provide appropriate and accurate comparisons. Doctors in training raised concerns that some valuable activities may not directly contribute to a measured patient outcome. Appropriate consideration must therefore be given both to the metrics used and to protecting such ‘non-measured’ activity.
Much concern has been expressed about the perverse incentives created by public reporting and targets. Attendees too were concerned, citing examples of potential refusal to treat high-risk patients or failure to report patient safety concerns. Such behaviour has deleterious consequences for patient care. The cardiothoracic experience demonstrates that the availability of data can be beneficial and that such issues can be avoided if the data are appropriately contextualised.9 Attendees felt that websites could potentially provide patients with useful information, reassuring them that their doctor meets an acceptable standard, while also supporting a drive within the profession to excellence. Equality of access to and translation of data were deemed essential to ensure that the provision of data does not widen health inequalities with more informed patients choosing higher performing providers.
As information technology facilitates the capture and communication of data in an environment of growing public expectation for transparency and information, the shift towards embedding performance management and reporting at the heart of quality healthcare provision is gathering momentum. No single uniform approach will work across specialties, organisations or patients. Tailored mechanisms will instead be required, together with a willingness to learn from cases where performance management and open reporting have failed to deliver higher quality healthcare. In this way, the NHS can avoid hitting the target but missing the point.
The future of medical education and training
The current objective of medical training is to produce doctors who are ‘fit for purpose’. Competency is essential, but more is needed to encourage the aspiration to excellence recommended by the Tooke Report11 and the high quality care advocated in the NHS review.1 One way to promote excellence is to incentivise performance of trainers and trainees. Currently, trusts are given performance incentives to deliver care but not to train doctors. This reflects one of the fundamental challenges of postgraduate training – its tension with service delivery. While service delivery itself offers training opportunities, a balance must be struck between the demands of training and delivering a service.
Doctors in training reported that medical training remains overly hierarchical, with attitudes of superiority commonplace. Some attendees felt that being labelled ‘juniors’, despite years of postgraduate work, can lead to disengagement of doctors in training from the profession, resulting in a cohort who feel disempowered and undervalued. Comparisons were drawn with peers in the private sector, where it is perceived that more emphasis is placed on the development of a motivated, productive workforce. Attendees felt that much could be learnt from other sectors, where optimising the ‘human infrastructure’ is viewed as a priority in delivering quality and innovation.
In the USA, teaching hospitals are forced to focus on their educational reputation in order to attract high-calibre students and doctors who they will train and nurture for several years. Attendees felt that hospitals in the UK do not have the same degree of educational investment, as doctors rotate through shorter attachments at each institution and job allocation is performed remotely. While postgraduate education remains the responsibility of deaneries in reality it is the hospitals that deliver training. By offering hospitals more responsibility, the quality of training may improve. Additionally, medical education is undergoing a shift in focus from knowledge to skills and attitudes. Advances in technology provide opportunities to further skills development. Attendees were particularly enthusiastic about the role of simulation in exposing doctors in training to challenging situations within a safe environment. It was proposed that education be continuous and integrated, coordinating undergraduate and postgraduate training and utilising emerging resources.
Attendees reported dissatisfaction that medical practice and training is increasingly dominated by ‘tick-box’ exercises. While it is recognised that these may increase objectivity, such assessments become problematic when the completion of a form is considered more important than applying the principles that the form attempts to assess. Discussions highlighted similar challenges facing the assessment and review system intended to provide quality assurance in postgraduate training. Attendees felt disappointed that competency-based training had not yet become a reality. Encouragingly, many felt that appropriate structures are in place but reported professional engagement in the process of assessment and review could be improved. As an evidence-based profession, doctors need evidence-based training and assessment.
Due consideration must be given to the balance between breadth and depth of experience. Gaps in the non-clinical curriculum leave medical graduates ill-equipped for the role of trainer, manager or policymaker. Despite these skill deficits, doctors are expected to be teachers, advocates and innovators. Attendees underlined the importance of sufficient flexibility within the system to ensure that individuals can express personal preference and develop their skills and interests. Additionally, the system must contain sufficient capacity to cope with the growing demands for flexible training and changing composition of the workforce.
The role of a doctor includes safeguarding the profession's future.12 This mandates a responsibility for doctors in training to feed back on their experiences and optimise training opportunities. The annual PMETB trainee surveys may facilitate improving the quality of posts. Doctors cannot simply receive or deliver training; they must also seek to better it. Attendees argued against mediocrity, stating that minimum competency should not be the end goal of medical training; there should be a move toward delivering excellence for our patients. Culture change takes time but it is important that organisations value doctors in training who offer energy, dedication and fresh perspectives. Trainees in turn must understand their obligations to their employers and their patients.
Conclusion
These discussions demonstrate that junior doctors can talk cogently, informatively and logically regarding these issues, demonstrating both an understanding of accepted viewpoints and a fresh approach to health policy challenges. At first glance, these three topics appear disparate. However, the over-arching themes and conclusions are common. Regrettably, disengagement and apathy have been pernicious within the medical profession; we believe we can do better. We can move forward by:
clarifying the extent of our role within society
maintaining transparency and accountability in the demonstration of its fulfilment
ensuring medical training and education maintain motivation and provide broad and transferable skills.
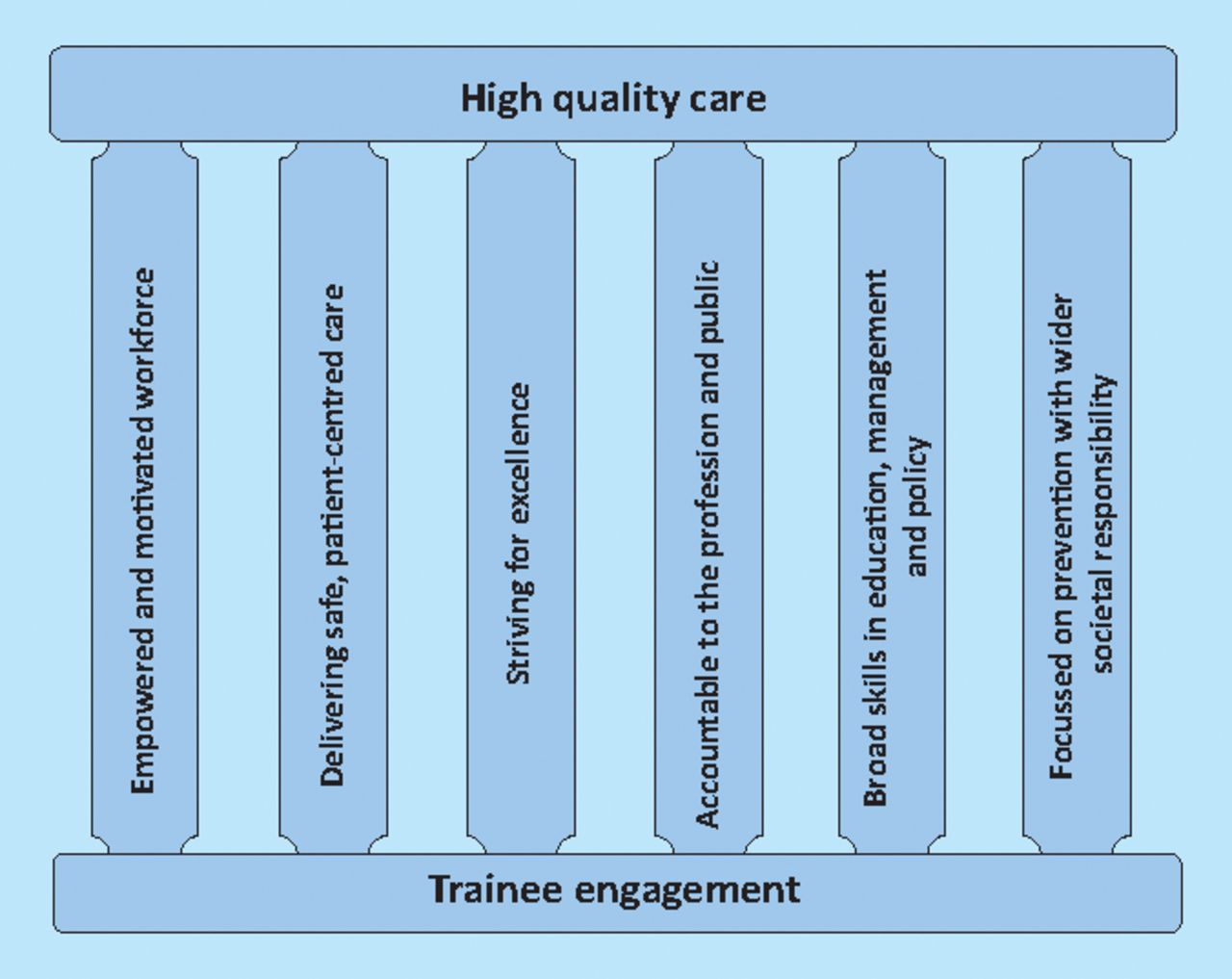
We have a vision of an empowered workforce, striving for excellence in the delivery of safe, high quality and patient-centred healthcare. The reflections in this paper provide an illustration of the creativity and enthusiasm that trainees can bring to the policy sphere. The principles described herein support the delivery of high quality care (Fig 1). Seven recommendations from these discussions have also been extracted to provide practical steps towards meeting the challenges that exist in these policy areas (Box 1). It has recently been said, ‘the second decade of the 21st century provides an opportunity for doctors to lead on the things that matter to them most…if doctors do not accept the challenge, they do not deserve to lead’.13 We accept this challenge, and call for greater trainee engagement at the policy table to demonstrate this.
Emerging recommendations

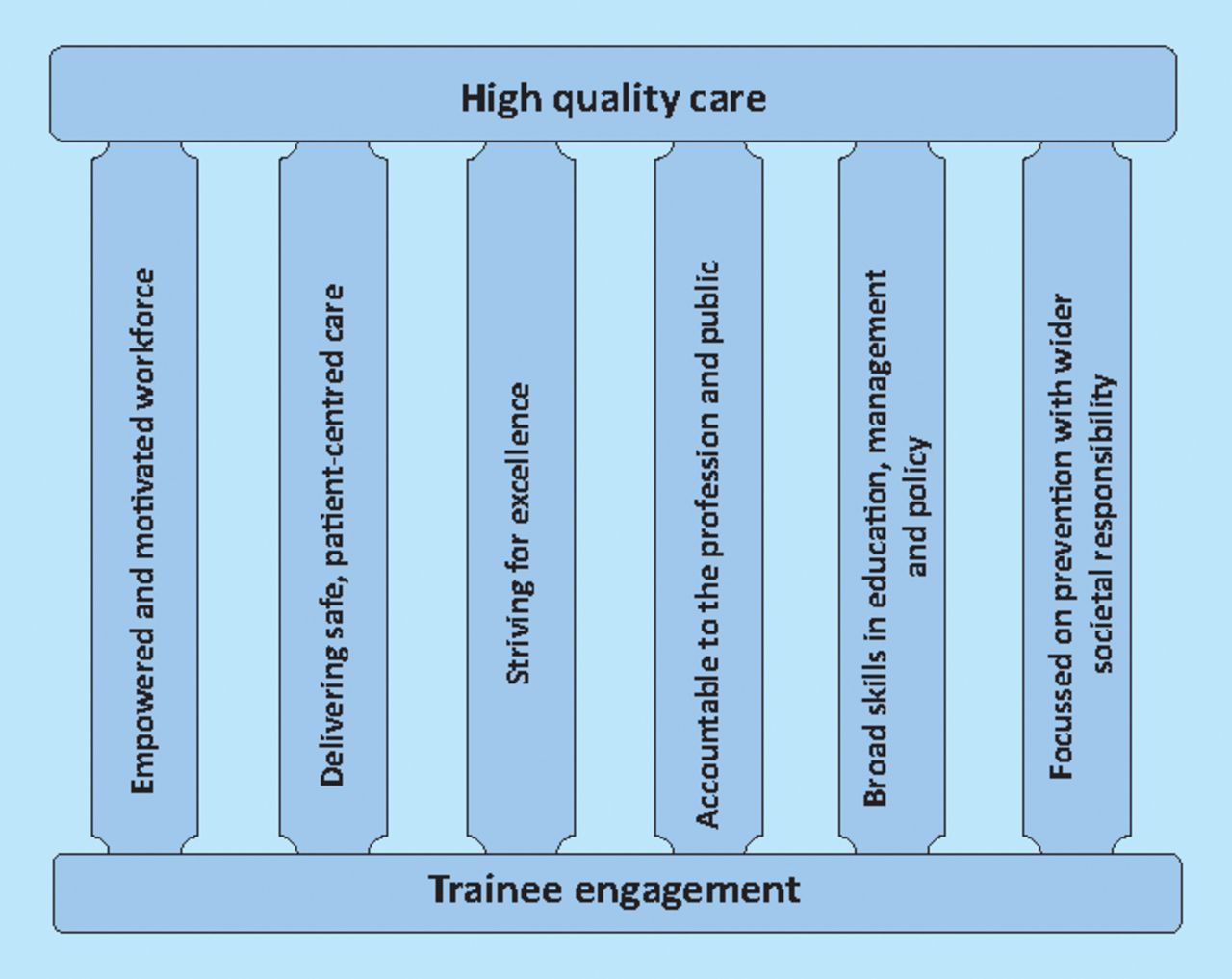
The six pillars of medical training and practice in the 21st century.
Funding
All authors want to declare financial support for the submitted work from the RCP. All authors also declare no financial relationships with commercial entities that might have an interest in the submitted work; no spouses, partners or children with relationships with commercial entities that might have an interest in the submitted work; no non-financial interests that may be relevant to the submitted work.
Provenance statement
The authors of this report were all participants in the evening of discussion at the RCP. All authors have contributed to and jointly authored this report. All authors are trainee doctors, from a variety of specialties and grades, who have previously participated in a national clinical leadership scheme. This has been either as a clinical adviser on the Chief Medical Officer's scheme or a Darzi fellow. Through their participation in these leadership schemes, they have worked at high level within key healthcare organisations including the Department of Health and RCP. This paper is based upon recollections, notes, audio recordings and transcripts of the event. The contents of this paper represent the interpretation of these by the authors, and in no way commit the Department of Health, RCP or other organisations. The authors would like to acknowledge Professor Peter Smith who facilitated the discussion and Professor Sir Ian Gilmore and Dr Sue Shepherd who conceived and facilitated the event. The event was funded by the RCP.
- Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.