
Lesson
A 56-year-old male presented to the accident and emergency department following an exacerbation of his chronic left arm and neck pain. He had a history of chronic lower back pain and was under regular pain clinic review. A lumbar spine decompression some years earlier had settled neuropathic symptoms, but mechanical lower back pain persisted. He was re-referred to the pain services with neck pain and left arm brachialgia two years earlier, notably worse on movement that was not restricted to the neck or left arm, and significant fatigue. This was perceived as further spinal radiculopathies and treated as chronic pain with various forms of oral and transcutaneous analgesia, acupuncture, transcutaneous electrical nerve stimulation (TENS) and epidural analgesia. None of these methods had proved successful, with morphine derivatives proving most effective.
On admission the patient was noted to look pale, diaphoretic and in pain. Clinical examination revealed a tachycardia with pulmonary oedema and no signs of right side heart failure. Chest X-ray confirmed pulmonary oedema, and an electrocardiogram (ECG) revealed left bundle branch block (Fig 1), with electrical interference from the TENS machine mimicking ineffective pacing spikes. On the basis of the ECG, arm pain and clinical signs he was thrombolysed with tenecteplase. This resulted in a significant alleviation of his pain, his tachycardia settled and his breathing improved. He was transferred to the coronary care unit for further investigation and treatment. Troponin T peaked at 0.74, so he underwent a coronary angiogram. This revealed severe triple vessel coronary artery disease requiring coronary artery bypass grafting (Fig 2).
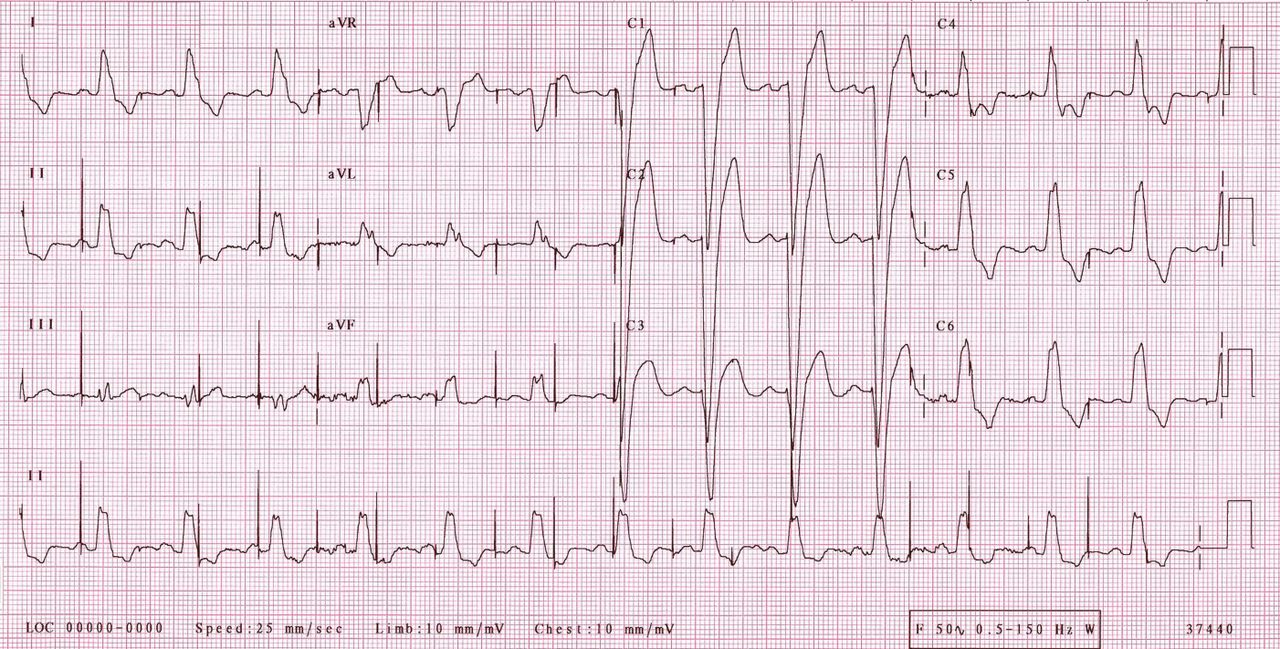
The 12-lead electrocardiogram. Electrical interference from the transcutaneous electrical nerve stimulation (TENS) machine mimics ineffective pacing spikes.

Left coronary angiogram revealing multiple stenoses of the left main stem, left anterior descending artery and circumflex artery. Note the collateral filling of the right coronary system indicating chronic ischaemia in that territory also. The apparent extra electrodes are from the TENS machine.
The patient was discharged and underwent bypass grafting six weeks later. Follow-up in the clinic three months later was encouraging. Surgery had gone well and resulted in a significant alleviation of the patient's neck and left arm pain. He returned to normal activities following recovery from surgery.
Discussion
Looking retrospectively at the patient's initial presentation to pain clinic it is apparent that his neck and arm pain, at least in part, was due to coronary artery disease (CAD) causing an atypical angina clinical syndrome. Correction of this coronary insufficiency caused a significant improvement in his quality of life. Due to the previous history of compression syndromes and lower back pain his symptoms were perceived in the first instance to be due to a similar pathology. The absence of chest pain meant CAD was not considered.
The diagnosis and treatment of brachialgia can be difficult, with the traditional textbook theory of ‘cervical affections presenting with radicular pain radiations’ being challenged by clinical studies, with only 33% of patients presenting in such a manner.1 The addition of provocative tests has not helped greatly, with methods such as Spurling's test, Valsalva's manoeuvre, and the upper limb tension test all displaying flaws in diagnostic accuracy.2 Treatment can be equally taxing, with limited randomised controlled trial data for most modalities in treating chronic brachialgia.
The possibility of angina pectoris causing his initial symptoms is easy to comment on retrospectively, but the very term angina, described by Heberden in 1772 as a ‘strangling and anxiety’ of the breast,3 led us to discount it as a possibility in the absence of chest pain. Anginal equivalents such as dyspnoea and fatigue have been well described, but tend to occur in the elderly or diabetics,4 and silent myocardial ischaemia is a relatively commonly encountered phenomenon.5 Radiation of pain to the neck, jaw and arms is also well documented, but rarely in the absence of chest discomfort, as in this patient.
Risk factors for coronary disease were present in the form of dyslipidaemia and undiagnosed hypertension. The extent of his coronary disease implies he may have been suffering with symptoms related to coronary insufficiency for some time, and had been monitored at pain clinic for over two years. It was difficult to attribute pain to significant exertion as his mobility was greatly restricted due to his mechanical lower back pain.
It takes more than one case to challenge the age old misnomer angina pectoris, but our patient does highlight the importance of keeping the adjunctive signs and symptoms of coronary insufficiency in mind when attempting to come to a diagnosis. If the diagnosis had been considered earlier, he may not have needed such radical treatment to improve his prognosis, and, perhaps more pertinently, resolve his pain.
- Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.