
Key points
Most patients with obstructive sleep apnoea (OSA) have not yet been diagnosed; symptoms of sleepiness/fatigue, low mood, nocturia and impotence may all warrant referral for sleep studies
There is a complex relationship between the metabolic syndrome and OSA
Weight loss should be strongly pursued in all overweight OSA patients
Treating hypothyroidism and acromegaly may cure OSA
Great caution should be exercised in the prescription of opiates to OSA patients
Obstructive sleep apnoea (OSA) is a common condition which greatly impacts on quality of life and is associated with reduced life expectancy. Most diagnosed cases are managed by respiratory physicians. There is established, well-evidenced guidance on treatment, especially with continuous positive airway pressure (CPAP).1 However, given an incidence of at least 2% in the adult population, it is inevitable that clinicians from a range of specialties will see patients with OSA of whom up to 80% will be undiagnosed. Such patients may present in extremis in the emergency room or as outpatients with symptoms that mimic those of another disorder or with a comorbid condition that predisposes to OSA. It is also important to have an understanding of prescribing for patients with OSA, including the risks of sedation.
This article reviews areas of overlap with non-cardiological specialties. An accompanying article discusses the cardiovascular associations of sleep apnoea syndromes. (pp 275–8).
Symptoms
Most people with OSA are males in mid-life and around 70% are obese. It is, however, important not to assume all patients fit this stereotype. A more complete risk profile is given in Table 1.2 The most frequently reported symptoms are daytime sleepiness and unrefreshing sleep with poor concentration. Low mood and marital disharmony are also commonly present.3 These symptoms reduce quality of life but may be misinterpreted as due to fatigue or depression. In women in particular the primary complaint may be one of feeling tired all the time with no energy, rather than falling asleep uncontrollably in the daytime. Headache especially on waking has been thought to be a symptom of OSA and may be present when severe OSA leads to ventilatory failure with CO2 retention, but headache alone is not suggestive of OSA even if it is present on waking.4
The STOP BANG scoring system. This validated score can be used as a quick screen for obstructive sleep apnoea (OSA) risk, particularly in judging presurgical risk and the need to refer for diagnostic respiratory studies. Reproduced with permission from Wolters Kluwer.
Nocturia is another common symptom of OSA. The likely mechanism is that negative pressure swings within the thorax during apnoeas cause an increase in transmural cardiac pressure. The atria are stretched, leading to increased release of atrial naturetic peptide with a resultant diuresis. Nocturia alone rarely causes daytime sleepiness and this combination of symptoms should trigger referral for sleep studies. The frequency of nocturia is a good predictor of the severity of OSA, as measured by the apnoea-hypopnoea index (AHI).5
Another common symptom in men is impotence. It is unusual for this to be the presenting symptom of OSA, but investigation of impotence in a man with OSA should be delayed until the sleep disordered breathing is adequately treated.
Occasionally patients present with a short history of worsening sleepiness, progressing to coma due to CO2 retention. There is an overlap with obesity hypoventilation, and patients may have coexisting chronic obstructive pulmonary disease (COPD),6 but in some the life-threatening decline is solely attributable to OSA. Cor pulmonale is often present. Initial treatment may include intubation and ventilation or non-invasive ventilation in the emergency room, but the outcome is generally favourable and CPAP may be adequate treatment at home in the long term.
Metabolic syndrome and obstructive sleep apnoea
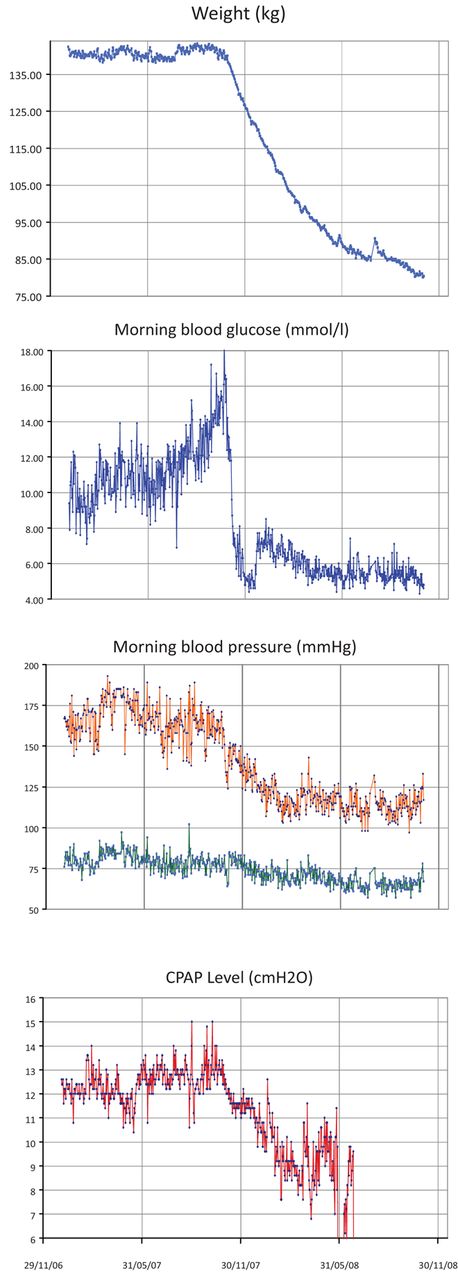
Combinations of central obesity, insulin resistance, dyslipidaemia and hypertension are commonly seen in people with OSA. Weight loss alone may lead to a resolution of all of these risk factors for ischaemic heart disease (Fig 1). Several aspects of the interrelationship of obesity and OSA have been summarised in a recent review.7 The relationship between OSA and obesity may be two way as there is evidence that sleep disruption can lead to weight gain, and treating OSA with CPAP can reduce visceral fat deposits. Weight loss through calorie restriction under strict supervision was effective in a randomised controlled trial for patients with mild OSA.8 For cases resistant to behavioural intervention, bariatric surgery may be indicated and can lead to marked reductions in the severity of OSA.

The effects of weight loss on obstructive sleep apnoea (OSA), and features of the metabolic syndrome. The graphs show the impact of weight loss achieved through increased exercise and a calorie controlled diet. The patient, a 58-year-old man, was taking 10 drugs (including for diabetes, hypertension (three drugs), dyslipidaemia, gout, depression and hypothyroidism) and using continuous positive airway pressure (CPAP). On advice from the sleep clinic, he started a weight loss regimen. He had an auto-CPAP device (this seeks the optimum pressure to treat apnoeas overnight, and the falling pressure shows the improved airway patency over time). At the end of the follow-up, CPAP could be withdrawn and his only medication was thyroxine (unchanged from his initial attendance). All data were recorded daily at home by the patient who had a technical background and was keen to monitor his own progress.
In regression analysis controlling for obesity, OSA has been shown to be an independent risk factor for insulin resistance.9 Among people with type 2 diabetes, 20% may have OSA, but treatment with CPAP does not necessarily improve glycaemic control.10 Weight loss may again be the most effective intervention if it can be sustained.
Endocrine disorders and obstructive sleep apnoea
Hypothyroidism
There is an overlap in the clinical features of OSA and hypothyroidism, and hypothyroidism may cause OSA. Subclinical hypothyroidism has been found in up to 11% of newly diagnosed patients with OSA,11 while in one series 30% of people with hypothyroidism had OSA.12 There is debate about the economic value of screening OSA patients for hypothyroidism, but treatment with thyroxine can cure the OSA in those with definite disease and unequivocally raised thyroid-stimulating hormone. Clinical benefit can occur before weight loss, probably through upper airway changes.11
Acromegaly
Acromegaly is a much less common disorder and there would be no value in screening for it in all OSA patients. However, the converse is not true, with reports of 50% of acromegalics having OSA. Again, treatment of the underlying endocrine disorder can lead to resolution of the OSA.13
Sex hormones
Sex hormones are implicated in the genesis of OSA. The condition is more common in men. The incidence in women increases after the menopause and may be reduced to an extent by hormone replacement therapy. Suppressing androgen secretion with progesterone in men is ineffective as a treatment for OSA; indeed, the levels may already be low in men with the condition.14 In men complaining of low libido and fatigue, OSA may explain a low testosterone level; treatment with CPAP can be associated with improved potency.15 Deterioration in OSA has been seen in male patients given testosterone supplementation. New symptoms of sleepiness in such a patient should trigger appropriate investigations. In women with polycystic ovary syndrome (PCOS) the serum levels of male hormones are raised and obesity is common. There is predictably an increased incidence of OSA, perhaps fivefold, compared with women without PCOS.
Other disorders
OSA is associated with increased levels of sympathetic tone. In occasional patients with severe hypertension, screening blood and urine results may suggest an underlying diagnosis of phaeochromocytoma. Treatment of underlying OSA can correct these abnormalities.16
Prescribing for obstructive sleep apnoea
A number of studies have investigated pharmacological interventions for OSA. They have in the main been underpowered and often of insufficient duration to document any changes in symptoms.14 There may be beneficial effects in individual patients from topical nasal steroids if nasal obstruction is part of the presentation. There are ongoing studies, but no other drug therapy can be currently recommended for the treatment of OSA. Several antihypertensive agents were examined to see if they might improve the OSA. None showed a consistent effect on apnoea frequency, but there were positive impacts on hypertension. Low mood is a common association of OSA and patients may be prescribed antidepressants. Studies have shown no adverse effects from selective serotonin receptor inhibitors, but no benefit in terms of apnoea frequency. Mirtazapine has been shown to increase daytime sleepiness and promote weight gain, and is not a drug of choice in OSA.
Adverse effects
Some drugs may exacerbate the severity of OSA:
Alcohol has long been reported to be such an agent. Patients may spontaneously report this association, although the scientific evidence is slight. Avoiding excessive alcohol consumption, which may itself adversely affect sleep quality and lead to weight gain, is to be recommended.
Sedation. There is understandable concern about the prescription of sedative agents which might relax the upper airway, suppress ventilatory drive and reduce the individual's likelihood of arousing from an apnoea – the usual mechanism by which the apnoea resolves. There has been general guidance that benzodiazepines should be avoided, with some reports of worsening OSA.11 In contrast, randomised controlled trials examining the impact of non-benzodiazepine sedatives, such as eszopiclone17 and prolonged-release melatonin,18 have shown no adverse effects on OSA indices in patients with mild to moderate disease.
There is more concern around opiates with evidence, at least in children, that people with OSA need lower doses of opiate/opioid medication for adequate pain control.19 Opiates should be kept to the minimum dose, in line with good prescribing practice in general, and patients should be strongly advised of the need to persevere with CPAP treatment for their OSA while taking opiates.
Interventions
Undergoing procedures, such as bronchoscopy or endoscopy under sedation or anaesthesia, may be a time of particular risk for someone with OSA. This is due to relaxation of the airway dilators, a blunting of the drive to arouse during an apnoea and potentially loss of airway reflexes due to local anaesthesia. In a helpful review, the limited data available were used to propose risk stratification, suggesting that procedures likely to be undertaken by physicians with awake sedation would be of relatively low risk.20 For all interventions, the use of opiates was a marker of increased probability of an adverse outcome. Additional oxygen should always be used judiciously during such procedures as it may obscure important hypoventilation, but this does not seem to be a particular risk for people with OSA in the absence of comorbid COPD or obesity hypoventilation. There is indeed evidence that it can improve overnight oxygen saturations, with no important deterioration in the AHI, and might lead to some improvement in mood, perhaps in this sole regard being more effective than CPAP.21
Conflict of interests
TQ has received sponsorship from UCB Pharma Ltd and a travel bursary from Cephalon UK to attend sleep medical conferences. IES has received a speaker's fee from Cephalon UK and sponsorship from UCB Pharma Ltd to attend a sleep medical conference.
- © 2011 Royal College of Physicians








{kind=link}