
Lesson
A 38-year-old man of Malaysian origin presented via an urgent referral to the diabetes clinic with a short history of fatigue, weight loss of 20 kg, polyuria and polydipsia. A random plasma glucose was 28 mmol/l and he had ketonuria. He was commenced immediately on insulin and his symptoms rapidly improved. Four months later, however, he presented to the emergency department with four weeks of worsening dizziness, fatigue, anorexia, weight loss, polyuria and polydipsia. He had no other past medical history of note. He had returned to the UK recently to seek a medical diagnosis after living in the Czech Republic for six years.
On examination he was cachectic (weight 41 kg, body mass index 18 kg/m2), pulse rate 110 bpm regular, blood pressure 110/60 mmHg lying and 70/30 mmHg standing. Further cardiorespiratory, abdominal and neurological examination was normal, with no signs of peripheral sensorimotor neuropathy or diabetic microangiopathy. Plasma glucose was 22 mmol/l and heavy ketonuria was noted, but arterial pH was 7.38 and bicarbonate was 22.2 mmol/l (22–29 mmol/l). Glycated haemoglobin on admission was 7% (4.8–6.4%). Electrocardiogram and chest radiograph were normal.
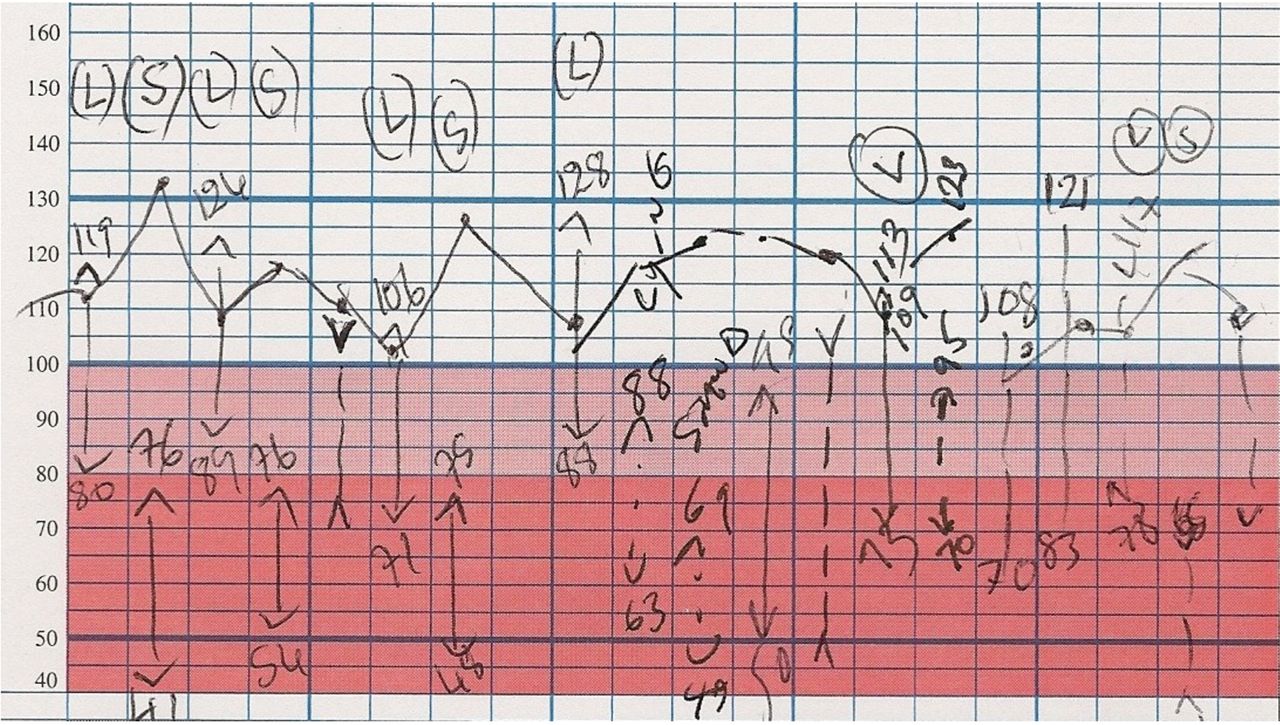
He was treated with intravenous (iv) 0.9% saline and insulin, and became rapidly normoglycaemic. His lethargy, anorexia, tachycardia and orthostatic hypotension, however, persisted. Postural blood pressure drops of 30–40 mmHg were noted (Fig 1) and he remained symptomatic with severe postural dizziness. Minimal symptomatic improvement was seen with fludrocortisone and midodrine. The patient had no other symptoms suggestive of diabetic autonomic neuropathy.

Severe orthostatic hypotension and tachycardia demonstrated on blood pressure chart.
In view of his persistent tachycardia and orthostatic hypotension, further investigation was undertaken. Serum sodium was low at 128–134 mmol/l (136–146). Serum and urine osmolalities were 254 mosmol/l (280–290) and 343 mosmol/l (50–1400) respectively, with a urinary sodium of 42 mmol/l. Synacthen test excluded hypoadrenalism (cortisol baseline 444 nmol/l, 30 minutes 872 nmol/l). Thyroid function, anterior pituitary hormones and tumour markers were normal. Coeliac antibodies, full autoimmune and serological screens were negative, including HIV and syphilis. Computed tomography thorax, abdomen, pelvis and magnetic resonance (MR) brain were normal. Echocardiography showed left ventricular global hypokinesis with moderately reduced left ventricular function (ejection fraction of 35–40%). Cardiac MR showed mildly increased signal in the mid-anterior and anterolateral segments on T2 weighting, indicating myocardial oedema and suggesting a myocarditis.
On further questioning, the patient revealed he had been camping in the Czech Republic and recalled a rash spreading over his arms the previous summer that had spontaneously resolved. Serum and cerebrospinal fluid (CSF) samples were strongly positive for Borrelia burgdorferi IgG, suggestive of Lyme neuroborreliosis. Three weeks of iv ceftriaxone was administered. At review, the patient remained fatigued, but postural hypotension had improved (lying 100/76 mmHg, standing 92/64 mmHg). Echocardiogram showed his ejection fraction had improved to 50%.
Discussion
Lyme disease is a tick-borne infection caused by Borrelia burgdorferi.1 It is endemic to northeastern USA and Central Europe, with incidence in the Czech Republic of 36 per 100,000. The clinical presentation is divided into early, late, local and disseminated features. Erythema migrans and flu-like prodrome are early features, while later features include arthritis, polyneuropathies, and Lyme carditis.1 The latter is rare but may manifest as AV block or a myocarditis.2 The Infectious Diseases Society of America recommend parenteral ceftriaxone, or oral doxycyline for two to four weeks for neurological or cardiac disease.1
While postural hypotension is well recognised in diabetic autonomic neuropathy, it was felt unlikely to be a cause of this patient's condition, as he had no other features of diabetic microangiopathy, and had a short duration of diabetes, which appeared to be well controlled.
Autonomic complications of Lyme neuroborreliosis are uncommon, but have been described previously as causing pseudo-obstruction3 and reflex sympathetic dystrophy.4 Radiculopathy, initially diagnosed as diabetic related, but subsequently found to be due to Lyme in diabetic patients has also been described.5 Patients with Lyme disease have shown lymphoplasmocellular infiltrates in the autonomic ganglia.6
- © 2011 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.