
Case presentation
An elderly Asian man returned from Bangladesh with an 18-month history of intermittent hiccoughs, anorexia, weight loss and fever. He had type 2 diabetes on insulin therapy with deteriorating glycaemic control. Examination revealed a thin, pale man, with intermittent hiccoughs, darkening of palmar creases and mucous membranes, angular stomatitis, oral ulceration and mild epigastric tenderness. He appeared clinically dry. He was noted to have a spiking fever to 38.58C and became notably hypotensive with a blood pressure 82/35 mm/Hg during his admission. Initial investigations are shown in Table 1. Chest radiography was unremarkable and an abdominal ultrasound noted a 13.5 cm splenomegaly. There was no evidence for a sub-phrenic abscess.
Initial laboratory investigations.
Differential diagnosis
This subject's initial presentation was relatively non-specific but in association with hypotension would fit with a diagnosis of Addisonian crisis. An infective process, particular tuberculosis (TB), would be high on the differential list given the patient's intermittent fever. Hiccoughs were a persistent feature of the initial presentation and focused attention on ruling out abdominal pathology, particular a subphrenic collection and uraemia. Examination and initial investigation did not identify evidence of a neurological or respiratory cause for hiccoughs. Both hyponatraemia and hyperglycaemia have been associated with persistent hiccoughs.
Initial management
The patient was treated symptomatically on initial presentation. Antipyretic medication was administered for the fever. Fluid resuscitation with normal saline was instigated when the patient became hypotensive. Blood sugars were monitored more intensively and his insulin titrated appropriately.
Case progression
Given the history, a serum cortisol was taken at 09.00. This revealed a cortisol measurement of <50 nmol/l. A subsequent short synacthen test demonstrated no response to adrenorcorticotropic hormone (ACTH) (0 min <50 nmol/l, 30 min 52 nmol/l, 60 min 50 nmol/l). Plasma ACTH was unequivocally raised (340 ng/l, normal 10–80) confirming primary adrenal failure. An abdominal computed tomography (CT) scan identified bilateral diffuse adrenal enlargement without calcification (Fig 1a).
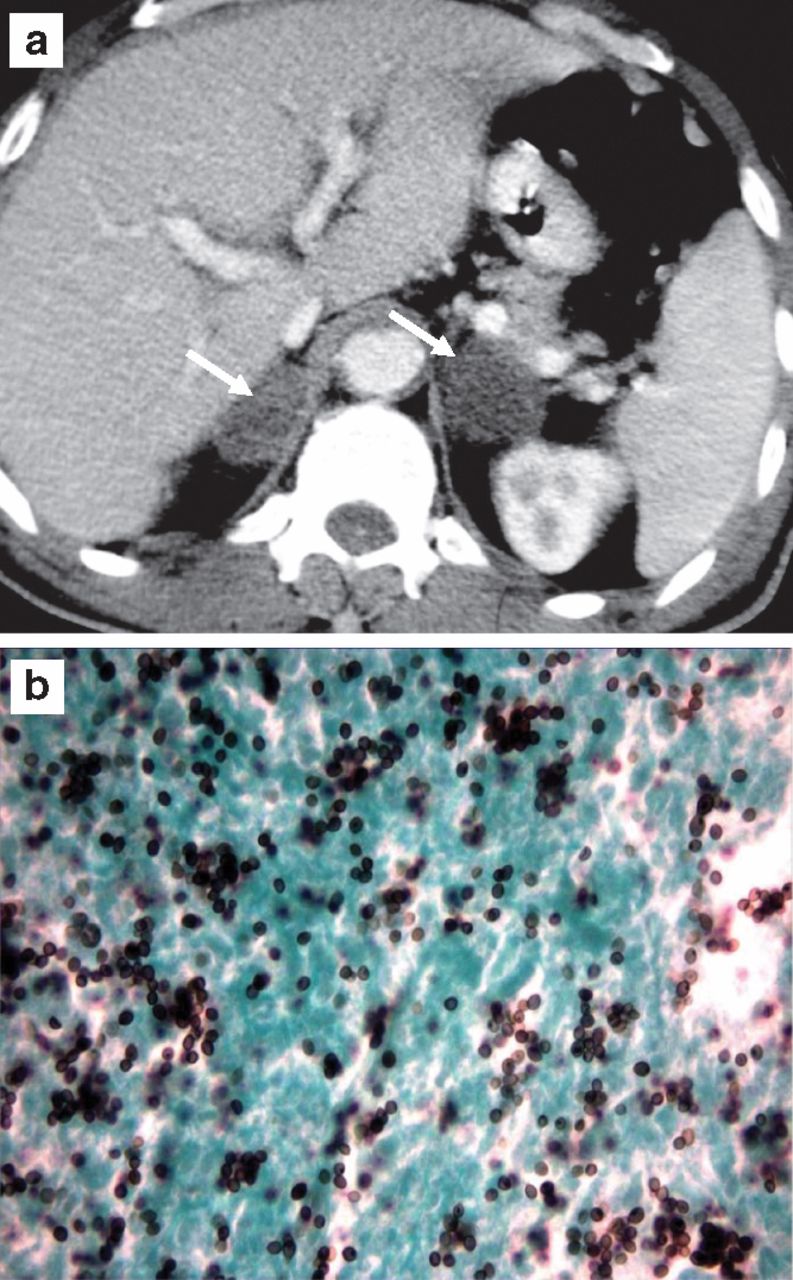
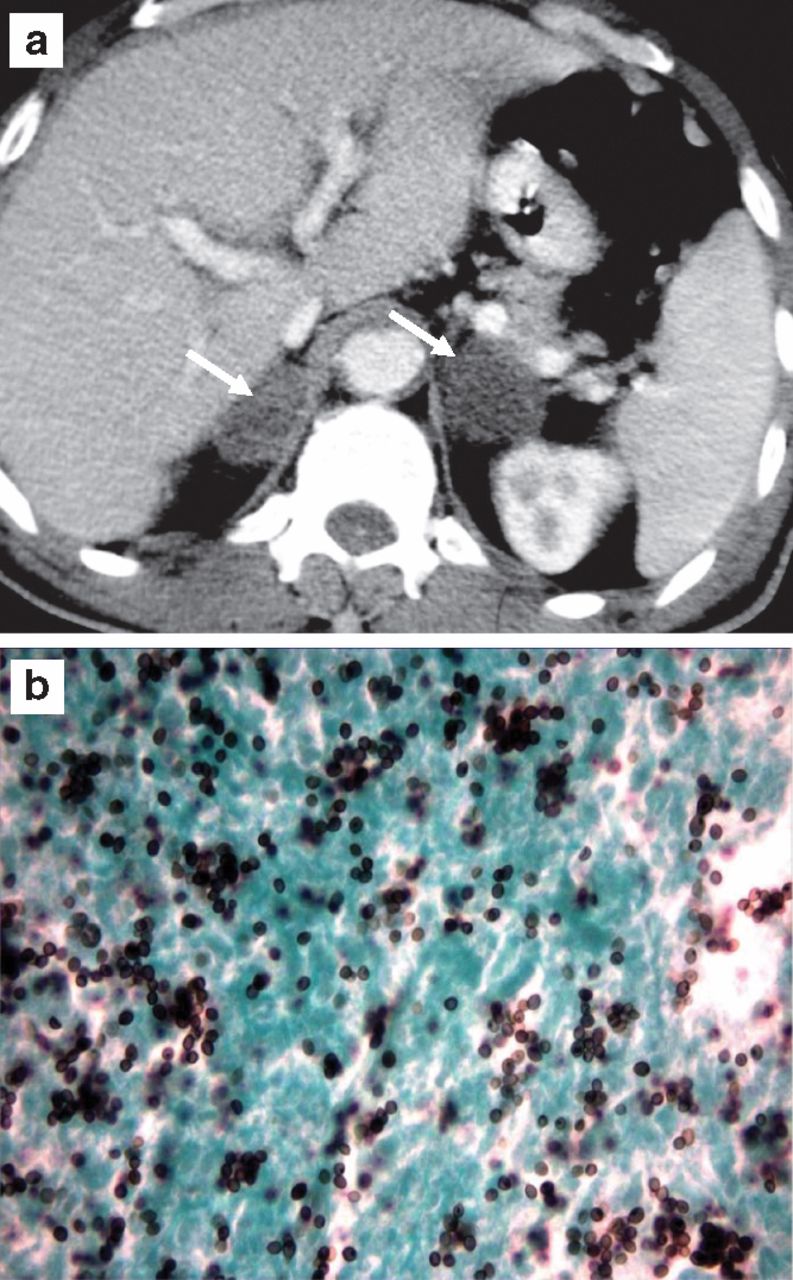
(a) Computed tomography (CT) abdomen (axial) demonstrates bilateral adrenal enlargement (white arrows). (b) Histology from CT-guided biopsy sample with Grocott stain revealing infiltration of histoplasma.
Further investigations revealed a serum 17-OH-progesterone was not raised, ruling out a diagnosis of congenital adrenal hyperplasia (CAH). Serum aldosterone was low, as expected with primary adrenal failure, but plasma renin levels were also undetectable. Plasma and urinary catecholamines were within the normal range. A Heaf test was negative. A CT-guided biopsy of the adrenals was carried out. This revealed the presence of numerous small yeast-like structures on polarisation microscopy which were strongly positive with Grocott's methenamine silver stain, suggesting a diagnosis of Histoplasma capsulatum (Fig 1b). This was confirmed by serology and culture. The patient was commenced on parenteral glucocorticoid (hydrocortisone) treatment initially and then converted to oral replacement. His symptoms significantly improved and the pyrexia was rapidly abolished. Mineralocorticoid (fludrocortisone) replacement therapy was subsequently commenced. Histoplasmosis was treated initially with ambisone (lysosomal amphotericin-B) intravenously and then oral itraconazole. His general condition improved, and he was discharged home.
A final diagnosis of Addison's disease with bilateral adrenal enlargement secondary to disseminated histoplasmosis was made.
Discussion
Though rare, bilateral adrenal enlargement has an important differential diagnosis. Differentials include tumours such as lymphoma, bilateral adrenocortical adenomas or phaeochromocytomas. Metastasis of tumours to the adrenal, adrenal haemorrhage (including the Waterhouse-Friderichsen syndrome) and congenital adrenal hyperplasia may all present with bilateral adrenal enlargement. Infections, most commonly TB but also other mycoses, are also important in the differential diagnosis.
Early in the initial assessment for adrenal enlargement several important issues must be clarified. These include the cortisol status of the subject and the need for glucocorticoid replacement, and evidence for a phaeochromocytoma, catecholamine excess and the need for sympathetic blockade. An adrenal biopsy may be necessary to secure the diagnosis and is indicated in the context of Addison's disease and adrenal enlargement. Histoplasma capsulatum, a dimorphic fungus, is the most common endemic mycosis worldwide. Found in the soil of bat and avian habitats, transmission occurs via aerolised spores. Common in North America (Ohio and Mississippi valleys), Latin America and East Africa, in endemic regions over 80% of the population may have been infected.1 Immunocompromised subjects are at greater risk. Acute infection may resemble a flu-like illness but many subjects remain asymptomatic. This case illustrates a classical presentation of disseminated histoplasmosis with probable hepatosplenic and confirmed adrenal involvement, mouth ulcers, fever and weight loss. Other features include lymphadenopathy, meningitis and diffuse interstitial lung infiltrates. Adrenal involvement is thought to occur in up to 10% of cases but histoplasmosis as a cause of adrenal failure is rare (<1%), with TB being the most common infective cause (20%).2,3 As such, there is a justifiably low threshold for considering anti-tuberculous therapy in patients with adrenal failure. However, similarities in presentation and a high mortality associated with untreated disseminated histoplasmosis (between 80% and 100%) make it an important diagnosis to consider despite its relative rarity, especially in patients coming from endemic areas.4 Laboratory diagnostics included antigen detection, serology and culture. Haematoxylin and eosin (H&E) staining with polarised light demonstrates the typical morphology of small yeast-like structures in addition to strong positivity with Grocott staining (Fig 1b). Treatment for severe acute or disseminated histoplasmosis includes intravenous amphotercin-B followed by oral itraconazole or ketoconazole which may require a prolonged course of treatment, up to one year.
Addisonian crisis is a medical emergency requiring a combination of fluid resuscitation, glucose and glucocorticoid administration. A new diagnosis may be secured by demonstrating an inappropriately low random cortisol and elevated paired ACTH level in the context of acute illness. A short synacthen test may be needed to clarify the diagnosis with equivocal cortisol measurements. This subject demonstrated an Addisonian biochemical picture of hyponatraemia, a metabolic acidosis and mild hypercalcaemia. Fever is a noted feature of adrenal failure. Hiccoughs have not been previously associated with a diagnosis of Addison's disease. Primary adrenal failure would normally be associated with low aldosterone and raised renin levels. In this subject, renin levels where undetectable suggesting an additional diagnosis of hyporeninaemic hypoaldosteronism (type IV renal tubular acidosis), likely to be a consequence of renal damage or autonomic dysfunction secondary to long-standing diabetes. While the case presented here describes a rare cause of bilateral adrenal enlargement, it highlights the need to be aware of the possible differential. Glucocorticoid and catecholamine status must be actively addressed and TB considered high on the differential list. For this particular subject, treatment resulted in resolution of the hiccoughs.
- © 2011 Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.