
Key points
Adrenaline for self-injection is frequently given inappropriately for non life-threatening localised reactions
Adrenaline for self-injection should only be prescribed for patients who have had systemic reactions and where there is a high probability of reoccurrence
The most common causes of chronic urticaria are stress and underlying medical problems, not immunoglobulin (IgE)-mediated allergy
Angioedema accompanied by urticaria is not due to hereditary angioedema
Angioedema triggered by angiotensin-converting enzyme inhibitors (ACE-I) may occur at any time after the initiation of therapy
Anaphylaxis has been defined as an acute, life-threatening systemic reaction with varied mechanisms, clinical presentations and severity that results from the sudden systemic release of mediators from mast cells and basophils.1 It is rapid in onset and may cause death.2 Anyone may develop anaphylaxis, but patients with a personal or family history of atopic disease are at greatest risk. The problem may be much more common than realised. Figures of 12–15% of the US population being affected have been produced,3 and an estimated one in 1,333 of the English population has experienced anaphylaxis.4 This figure is based on prescriptions for adrenaline (epinephrine) for self-injection and may therefore overestimate the number of true systemic reactions. Fatal reactions appear rare, perhaps less than one per five million population per year, but the published figures may not be reliable as there is no requirement specifically to report deaths due to anaphylaxis.5 The figure was acquired after self-injection devices were introduced so it is not known what difference the devices have made to outcomes in terms of deaths prevented. Clinical experience suggests that adrenaline is being administered unnecessarily for localised reactions without airway compromise, and that too many patients are being issued with adrenaline for self-administration. It is essential that self-injection devices are issued only to those patients with a clinical indication and that they are shown how to use them correctly and that the technique is rechecked when prescriptions are reissued.
Urticaria and angioedema
Urticaria is characterised by a red, raised itchy rash resulting from vasodilatation, increased blood flow and increased vascular permeability consequent upon mediator release from mast cells. Urticarial wheals can vary in size (from a few mm to large lesions (10–20 cm), they may be single or numerous and are intensely itchy. Urticaria occurs in the superficial dermis while angioedema refers specifically to localised deep tissue swelling.
Urticaria and angioedema may occur together and as a part of an anaphylactic reaction, but either may occur alone and may not be due to non-immunoglobulin (IgE) mechanisms, although almost all urticaria is non-IgE mediated. Urticaria is common: at least 20% of the population will have it at some point in their life. Adrenaline is not indicated for the management of urticaria.
Anaphylaxis
Anaphylaxis due to the presence of IgE antibodies (type 1 hypersensitivity) represents the most severe form of immediate allergic reaction. The immune system must have been exposed previously to the allergen for IgE antibodies to form and anaphylaxis occur.
The reaction is due to release of mediators from mast cells, stimulated by allergen cross-linking of membrane-bound specific IgE antibodies. There is immediate release of histamine from preformed granules in the mast cells, the mast cells are then activated leading to increased synthesis of other mediators such as leukotrienes. This synthetic process builds up over 4–6 hours, and is thought to be responsible for late reactions which may occur some hours after the initial immediate reaction has subsided. Clinically similar reactions can be caused by substances that directly activate mast cells without the presence of specific IgE (previously termed anaphylactoid reactions). Substances well known to trigger this type of reaction include strawberries, radiographic contrast media and opiates (codeine and morphine derivatives). Direct ingestion of histamine through eating foods rich in histamine (tomatoes, shrimps, lobster) or foods that have undergone bacterial spoilage (scombroid poisoning) will rarely give clinically similar reactions.
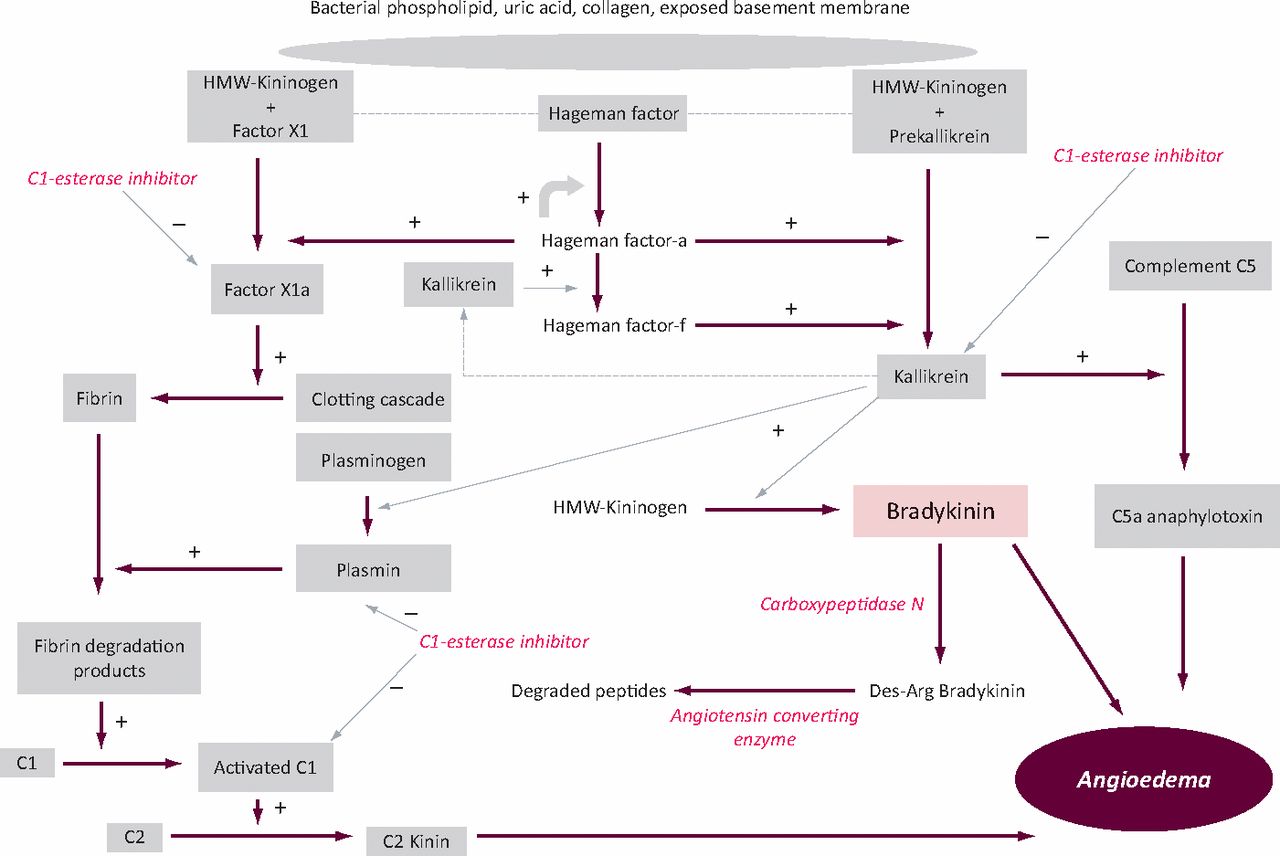
The swelling of angioedema is caused by uncontrolled activity of bradykinin (Fig 1) and, to a lesser extent, complement breakdown products such as C2-kinin. Rarely, angioedema may be hereditary, due to defects in C1-esterase inhibitor (types I and II)6 and gain of function mutations in coagulation factor XII (Hageman factor, type III).7 Angioedema may occur in the context of specific IgE-mediated responses but most cases are not associated with any identifiable external trigger.

Diagram of factors involved in generation of angioedema and the roles of C1-esterase inhibitor and angiotensin-converting enzyme (HMW = high molecular weight).
There should not be an assumption that all cases of urticaria and angioedema are allergic in nature, and these should be distinguished from the systemic response of anaphylaxis. The treatment is very different.
Signs and symptoms
Anaphylaxis is a systemic reaction. Typical features include a feeling of doom, hypotension, often with loss of consciousness, diarrhoea, vomiting and abdominal cramps, laryngeal oedema and bronchospasm. Urticaria may be present, but up to 50% of reactions may not be accompanied by this rash.8 Urticaria, with or without angioedema, especially when chronic, is almost never due to IgE-mediated mechanisms.
Patients with underlying asthma are at greater risk of severe reactions with bronchospasm. Risk factors for a fatal outcome to anaphylaxis may include age (and age-related comorbidities such as hypertension, ischaemic heart disease (IHD)) and drug therapy (particularly angiotensin-converting enzyme inhibi-tors (ACE-I)). Summers et al 9 have examined risk factors for anaphylaxis in peanut and tree nut allergic patients and found that severe pharyngeal oedema was more likely to be present in patients with severe rhinitis and those with low levels of ACE (≤37 mmol/l). Life-threatening bronchospasm was more likely in patients with severe asthma, while altered consciousness was more likely in those with severe eczema. There has been debate about whether beta-blockers have an adverse effect on outcome, but
Causes
Almost any substance is capable of triggering an IgE-mediated anaphylactic reaction. Table 1 lists the most common causes of anaphylaxis and Table 2 the differential diagnosis.
Causes of anaphylaxis.
Differential diagnosis of anaphylaxis.
Onset of anaphylaxis is rapid. Attempts by the patient (or doctor!) to blame foods eaten the day before are erroneous. Although textbooks say that anaphylaxis may occur up to six hours after ingestion/exposure this is, in practice, exceptionally rare and two hours is really the outside limit. History should include the contribution of exercise, as symptoms may rarely become apparent only when consumption is followed by exercise11 - this is an increasingly important problem. Non-steroidal anti-inflammatory drugs (NSAIDs) make it worse by increasing the passage of allergen through the gut into the blood stream in an undigested and immunoreactive form.11
Not all cases of anaphylaxis are easily resolved, and a group of patients with idiopathic anaphylaxis remain. These patients often have repetitive attacks and may require continuous steroids to control them. It is important to identify mastocytosis, as this can predispose to severe and recurrent episodes of anaphylaxis. Patients with mastocytosis must be warned of the risks of drug administration, especially anaesthetics. Within the group of patients with a history of recurrent anaphylactic reactions are a small number of patients with somatoform disorders.12
Angioedema
Localised angioedema, even with involvement of the tongue and pharynx with no systemic features, is not anaphylaxis although frequently erroneously so labelled in accident and emergency (A&E) departments and medical admissions units. Angioedema is not accompanied by systemic features. Whatever the cause, it is often preceded by a premonitory prickling at the site, but is never itchy unless urticaria is also present. Urticaria when affecting the face and especially around the eyes can give the impression of angioedema, but the distinguishing itch will be present.
Hereditary angioedema
Hereditary angioedema (HAE) is a very rare genetic condition, affecting approximately one in 100,000. There will be a family history in most but not all cases. Idiopathic, non-allergic angioedema is at least 100 times more common and usually has a much more rapid onset than HAE. Complement abnormalities during an attack will distinguish the two. HAE typically demonstrates very slow development of angioedema, without urticaria. In this condition, bowel oedema may occur, causing severe abdominal pain frequently mistaken for an acute abdomen. Failure to recognise this may lead to inappropriate laparotomies, often on more than one occasion. Almost all cases of angioedema presenting to A&E or admissions units will be due to causes other than HAE.
Causes
The most common identifiable causes of angioedema without urticaria are drugs, particularly ACE-Is, statins, proton-pump inhibitors and NSAIDs (Table 3). A proper drug history is therefore essential. ACE-Is cause angioedema by preventing the breakdown of bradykinin. Figures vary for the number of patients developing angioedema on ACE-Is, but it may be as high as 5%. Of patients presenting to a tertiary referral clinic with angioedema, 11% had ACE-I induced angioedema.13 The attacks may commence at any time after the initiation of therapy and may persist for up to three months after drug withdrawal.
Causes of angioedema.
Angioedema frequently develops during the night or in the early hours of the morning, waking the patient. This effectively excludes foods and other triggers consumed the day before. The predilection for angioedema to develop at this time is unknown. HAE should be considered (see above).
In older patients presenting with angioedema alone, it is important to look for rare acquired angioedema secondary to paraproteins which block C1-esterase inhibitor function (acquired angioedema). This is usually associated with splenic villous lymphomas. In younger patients, usually with systemic lupus erythematosus autoantibodies against C1-esterase inhibitor have been reported rarely.
No cause for the angioedema is identified in many patients and is frequently labelled as ‘idiopathic’. However, it is important to recognise the major role that psychosocial stressors play in the development of all types of pseudo-allergic reactions, including angioedema. Failure to identify these and advise the patient appropriately will ensure that the problem continues unabated.
Suspected anaphylaxis: investigations
Where there is doubt about the diagnosis of anaphylaxis, measurement of serum mast cell tryptase (MCT) levels can be valuable. MCT is a protein released into the circulation when histamine is released from mast cells. Levels increase within 15 minutes and decay with a half-life of 1.5–2.5 hours. In severe anaphylaxis, levels may remain raised for up to 24 hours and may also be raised in post mortem samples from patients dying from anaphylaxis. A clotted blood sample taken as early as possible during the reaction, preferably within 2–4 hours of onset can be helpful. Most cases of urticaria and angioedema will have normal MCT levels. An elevated MCT does not, however, distinguish between IgE and non-IgE mediated mast cell degranulation nor does a normal level exclude the possibility of an allergic reaction. Elevated baseline tryptase levels are found in mastocytosis.
In light of the studies suggesting that ACE levels are a risk factor for pharyngeal oedema, checking the ACE level would seem to be a sensible step. Tests to specific allergens are most appropriately performed in the allergy clinic either by using skin-prick tests or by taking blood samples to measure specific IgE. If wheat-dependent, exercise-induced anaphylaxis is suspected, checking for specific IgE to omega-5-gliadin has been found to be a useful predictive test. In patients presenting with attacks of hereditary angioedema, serum C4 levels during an episode will be low/undetectable.
Immediate management of anaphylaxis
Much of the management of anaphylaxis has never been evaluated in controlled clinical trials for obvious reasons and treatment is therefore pragmatic. The UK Resuscitation Council produced guidelines on the emergency treatment of anaphylactic reactions in 2008.14
Adrenaline
The treatment of anaphylaxis involves the prompt administration of adrenaline, which must be given by the intramuscular (im) route. First-response dose of adrenaline is usually 0.3–0.6 mg im for adult patients. A recent Cochrane review concluded that the use of adrenaline in anaphylaxis is based on tradition and on evidence from fatality series in which most individuals dying from anaphylaxis had not received prompt adrenaline treatment.15
Many patients will have self-injection devices such as Epipen or Anapen. Prescribers should be aware that the mechanisms for triggering these devices are different and therefore they should not be used interchangeably. If intravenous (iv) adrenaline is used, it must be diluted via an infusion pump (10 ml 1 in 10,000 adrenaline, diluted with 100 ml normal saline) with ECG monitoring. Significant complications can occur from using iv adrenaline including cardiac ischaemia, arrhythmias and death. It should be used only in a hospital setting by experienced specialists.
Steroids
Steroids should be administered at the earliest opportunity, not for any immediate benefit but to prevent both the production of leukotrienes and late-phase reactions (rare but preventable). The optimal dose of steroid is not known. Current guidelines suggest a dose of 200 mg hydrocortisone iv for adults.14 An attempted meta-analysis of the use of steroids identified no suitable studies so the actual value is uncertain.16 Until appropriate studies are done, custom and practice indicate that steroids should be administered.
Antihistamines
Chlorphenamine 10 mg iv is usually given. Its value is dubious once there has been massive histamine release, particularly as it is a weak antihistamine compared with third-generation antihistamines such as cetirizine or fexofenadine. It is sedating, which may be valuable in reducing anxiety. Oral administration of cetirizine 20 mg may be better if the patient can swallow. A Cochrane Review17 has found no satisfactory trials addressing the value of antihistamines in this setting. It is probable that there never will be any trials because of the logistic difficulties.
Observation
A patient who has had an anaphylactic reaction must be kept under medical observation for a minimum of six hours in case of late-phase reactions. After a period of observation, the patient may be discharged if fully recovered. (Admission to hospital is not required unless there are continuing problems.) Adrenaline for self-injection should be prescribed only for patients who have had a severe systemic reaction to an unknown or unavoidable allergen, and then only if full training of the patient is given (Table 4). Patients who have had reactions to drugs should not receive injectable adrenaline devices, but instead clear instructions about drug avoidance, backed up by information to GPs.
When to give adrenaline for self-injection.
Immediate management of angioedema
The management of urticaria and angioedema has been well-reviewed.18 Adrenaline is not indicated for angioedema unless there is clear evidence of laryngeal involvement. Administration of a large dose of a long-acting, non-sedating antihistamine, such as cetirizine 20–40 mg stat or fexofenadine 180–360 mg stat, together with a single oral dose of prednisolone 20 mg is usually sufficient for the management of symptoms. The dose of both can be repeated after 24 hours. It is best to avoid long courses of steroids. If a patient is taking ACE-Is, these must be stopped at once and, if necessary, an alternative given. Angiotensin receptor blockers and the newer renin antagonists are usually, but not always, safe. Other drugs well known to cause angioedema, such as NSAIDs and statins, should be avoided or stopped pending specialist review.
Hereditary angioedema
Hereditary angioedema does not respond well to adrenaline, steroids or antihistamines. Treatment has largely been with purified C1-esterase inhibitor, but new treatments are now available. Management should be discussed with a clinical immunologist.
Immediate management of urticaria
The acute management of urticaria is similar to angioedema: high doses of oral non-sedating, long-acting antihistamines should be used. Oral chlorphenamine should be given only at night because of its sedating effect. Continuous oral steroids are inappropriate, but a single dose to treat acute flares is acceptable. Doses of antihistamines in excess of those recommended in the British National Formulary (BNF) will frequently be required. Safety data exist for cetirizine and fexofenadine in doses up to fourfold higher than normally used. This is preferable to the use of steroids.
Follow-up management
Anaphylaxis
For a patient not previously known to suffer from anaphylaxis, it is essential that rapid follow-up is arranged with a clinical service experienced in the investigation and management of anaphylaxis. This may be carried out either by a clinical immunologist or an allergist and can be undertaken as an outpatient once the patient is stable and can be discharged from hospital. Any information about food exposure at the time of the reaction should be preserved or noted until this review as it may give valuable clues to further investigation.
If there is deemed to be a risk of further systemic reactions and the allergen is unavoidable, a self-treatment kit with adrenaline for self-injection (minimum of two pens), together with cetirizine 20 mg and prednisolone 20 mg as stat oral doses should be provided (Table 4). Clearly, patients with risk factors such as asthma, severe rhinitis, elevated serum tryptase levels and low ACE levels should be prioritised to receive adrenaline. Caution should be observed in giving adrenaline to patients with known or suspected IHD, uncontrolled hypertension, or those taking tricyclic antidepressants or cocaine, due to the risks of ventricular arrhythmias. The dose of adrenaline in those on beta-blockers should be reduced by 50% to prevent unopposed alpha activity and paradoxical hypertension. Whether beta-blockers should be stopped is debatable and should involve a discussion between the patient's cardiologist and immunologist/allergist.10
Urticaria and angioedema
Patients with recurrent urticaria and angioedema who have frequent attacks may benefit from regular preventative antihistamines, using long-acting, non-sedating antihistamines. Doses may need to be escalated above those normally recommended in the BNF (30 mg bd for cetirizine). For nocturnal symptoms, sedating antihistamines including chlorphenamine and hydroxyzine may be considered. Cimetidine, which has unusual immunosuppressive properties, has been suggested as an additional treatment but benefit appears to be limited. It is unclear whether other H2-blockers have the same effect. Doxepin has potent antihistaminic activity but is very sedating. Mirtazipine is also very effective and has fewer side effects. As noted, long-term steroids should be avoided. For angioedema alone without urticaria, antihistamines may be effective, but better results may often be obtained with tranexamic acid (1 g qds). Monitoring of liver function is necessary and regular ultrasound scans of the liver (every three years) are recommended if treatment is long-term.
Conclusions
Anaphylaxis is now a common and serious, but fortunately rarely fatal, medical health problem and it is crucial that patients receive appropriate acute and follow-up treatment. It is however essential that it is distinguished from benign non-allergic urticaria and angioedema (which is at least 100 times more common), and that adrenaline is used only in those patients that truly require it. A good working definition of anaphylaxis is a reaction which involves one or both of the two severe features:
respiratory difficulty, which may be due to laryngeal oedema or asthma, and/or
hypotension, which may present as fainting, collapse, or loss of consciousness.19
The Resuscitation Council use similar criteria (airway, breathing and circulation problems) in addition to the rapidity of onset of symptoms and the presence of skin/mucosal changes, although recognising that these latter changes may be absent or subtle.14
Using these definitions, patients can be correctly identified as having anaphylaxis and early treatment with im adrenaline given appropriately, whilst avoiding unnecessary prescriptions in those who do not require it. Delay in administration of adrenaline has been identified as a risk factor for a poor outcome.20 However, giving a patient a diagnosis of anaphylaxis inappropriately can not only lead to unnecessary prescriptions of adrenaline but may also lead to increased anxiety levels for patients and family. Therefore the clinician should be confident of the diagnosis before management is instituted.
- © 2011 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.