
Key points
Malaria must be considered in all patients with fever or history of fever who have visited a malaria endemic country
The challenge in malaria is that of rapid diagnosis and initiation of appropriate antimalarial and supportive treatment
Physicians should be aware of the therapeutic and prognostic implications of life-threatening falciparum versus non-falciparum malaria
Prompt recognition of the severe manifestations of malaria requires an increased level of care or referral to a specialist unit
The water-soluble artemisinin derivative, artesunate, one of the new antimalarial agents, is the current drug of choice in severe falciparum malaria rather than quinine
Malaria is one of the most common imported infections in travellers.1 The number of cases in travellers is trivial set against the global scale of disease, but in this age of frequent international travel it is essential that clinicians are at least aware of when to suspect, and how to diagnose malaria. Detailed specialist advice can always be sought.
Epidemiology
The five species of malaria parasites now known to affect humans differ in their geographic distribution:
Plasmodium falciparum: most common in sub-Saharan Africa and Melanesia (Papua New Guinea and the Solomon Islands).
P. vivax: mainly Central and South America, North Africa, the Middle East and within the Indian subcontinent.
P. ovale: almost exclusively in West Africa.
P. malariae: mainly in Africa.
P. knowlesi: on the island of Borneo and other parts of South-East Asia.2
Clinical features
The clinical symptoms and signs of malaria are produced by the asexual forms in the blood which destroy red cells, localise in critical organs, obstruct the microcirculation and release ‘toxins’, leading to the classical malarial rigor with pronounced fever.3 The incubation period is variable, but may be as short as seven days and, exceptionally, up to 20 years. Most (>90%) P. falciparum infections in travellers occur within six weeks after return from foreign travel. Compliance with antimalarial chemoprophylaxis cannot exclude the diagnosis.
After a prodromal period of fatigue and aching, the abrupt onset ensues of a rigor consisting of a ‘cold’, ‘hot’ and ‘sweating’ phase, and high temperature. In P. knowlesi infections the cycle occurs every 24 hours; in P. falciparum the periodicity of fever tends to be less predictable, and the fever may be continuous due to the asynchrony of parasite development. Headache, cough, myalgia (flu-like symptoms), diarrhoea and mild jaundice are non-specific symptoms of all malarias. Examination of a patient with mild malaria often reveals a fever, tachycardia and little else.
Severe malaria
Definitions of the clinical manifestations of severe malaria (complications) are for the standardisation of clinical studies rather than for clinical care and must be taken in context (Table 1).4 Any degree of impairment of consciousness, prostration, jaundice, evidence of renal impairment, repeated vomiting or a parasitaemia of 2% or higher, especially in non-immune individuals and in pregnancy, should be treated parenterally.5 In our study of falciparum malaria, a parasitaemia of that level predicted a 12-fold risk of severe disease.6 In a large study of 400 cases of severe malaria, increasing age, increased parasitaemia and decreased Glasgow Coma Score were associated with increased mortality.7
Manifestations of severe falciparum malaria.4*
Complications of severe malaria
Cerebral malaria
The patient may pass from drowsiness to coma gradually over a few days or abruptly within 1–2 hours, often heralded by a convulsion. Most of these patients have no focal neurological signs, but occasionally they may have cranial nerve palsies, monoplegia or hemiplegia, extensor posturing, decerebrate or decorticate rigidity, dysconjugate eye movements, grinding of the teeth (bruxism) or hiccoughs. Coma may be due to direct neurological involvement, status epilepticus, severe acidosis or hypoglycaemia, each of which requires different management.
Respiratory distress
In respiratory distress there is rapid laboured breathing, sometimes abnormal in rhythm,8 resulting from an acute respiratory infection, compensation for severe metabolic acidosis, severe anaemia or pulmonary oedema. Pulmonary oedema, in turn, results from hypoalbuminaemia, iatrogenic fluid overload or direct alveolar capillary damage leading to the acute respiratory distress syndrome. Again, each of these requires different management.
Acidosis
Acidosis (base excess <12 mmol/l), acidaemia (pH <7.3) or lactate above 6 mmol/l indicates a poor prognosis. It results from poor tissue perfusion, lactate generation by the parasite and anaerobic glycolysis, reduced lactate clearance by the liver, impaired renal function (acid excretion) or exogenous acids (eg salicylates).
Hypoglycaemia
Decreased conscious level may obscure the diagnosis of hypoglycaemia. Suspicion should be circumstantial, especially during quinine therapy, particularly if the patient is pregnant.9 The cause of hypoglycaemia is multifactorial; hyperinsulinaemia due to quinine therapy is important.

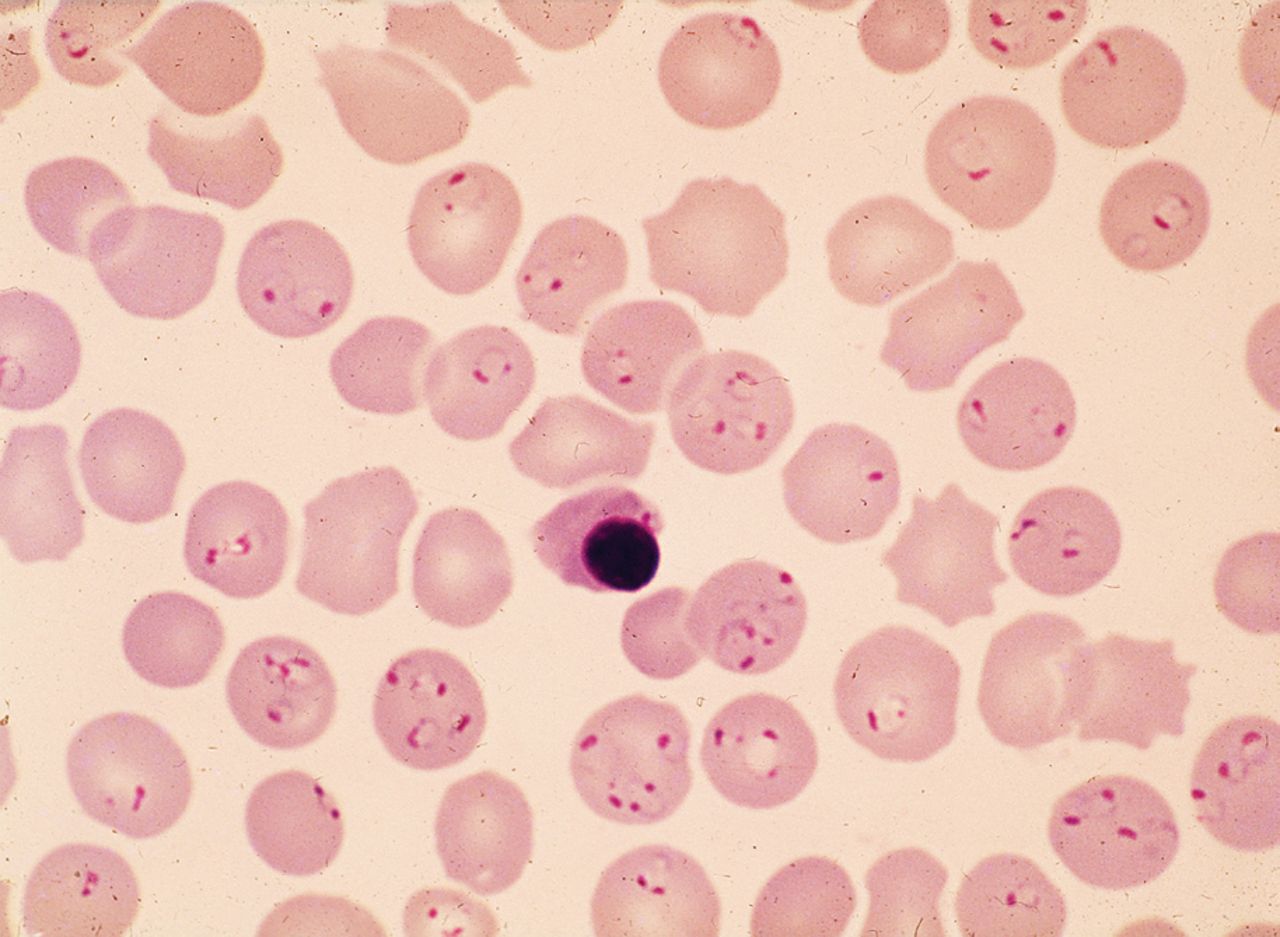
Blood film showing Plasmodium falciparum hyperparasitaemia.
Circulatory collapse (shock)
Shock is relatively rare. The blood pressure may be at the lower end of the normal range due to vasodilatation and hypovolaemia. Hypotension is more commonly due to supervening bacterial sepsis.10
Bleeding
Despite the frequent presence of thrombocytopenia, most likely the result of diffuse sequestration of platelets,11 overt evidence of bleeding is rare in malaria. Bleeding is more likely to occur in the setting of disseminated intravascular coagulation. There is often subtle activation of the coagulation cascade in the absence of clinical bleeding.12
Renal involvement and blackwater fever
A degree of renal impairment commonly occurs in severe malaria. Acute renal failure is rare, but can occur not only during the acute parasitaemic phase but also after parasite clearance, and may be non-oliguric. Blackwater fever may be dramatic, sometimes in the setting of glucose-6-phosphate dehydrogenase (G6PD) deficiency or in a semi-immune patient given quinine, but does not invariably lead to renal impairment.13 Hyponatraemia is often self-correcting.
Severe anaemia
The anaemia of falciparum malaria is both complex and multifactorial. The fall in haemoglobin is in excess of what can be accounted for by the loss of infected red blood cells alone. Mechanisms include red cell lysis by parasites, removal of uninfected cells due to antibody sensitisation or other physicochemical changes in the spleen.
Diagnosis
Malaria must be considered in all patients with fever or a history of fever who have visited a malaria endemic country, so a travel history should be a routine part of any consultation of such patients. Malaria is a great mimic and must enter the differential diagnosis, which includes typhoid, viral illnesses such as dengue fever, influenza and hepatitis, brucellosis and respiratory, gastrointestinal and urinary tract infections.
Blood films
The definitive diagnosis of malaria is made by microscopic examination of thick and thin blood films. In falciparum malaria, mature trophozoite forms, the presence of schizonts or excessive malarial pigment present in neutrophils or macrophages might signify a worse prognosis.14
Rapid diagnostic tests
Based on antigen capture, rapid diagnostic tests using a monoclonal antibody to the histidine-rich protein 2 of P. falciparum or parasite lactate dehydrogenase of P. falciparum or P. vivax require minimal expertise but are expensive and not quantitative.15
Treatment
The mainstay of treatment of mild malaria is the administration of specific and appropriate antimalarials.5
Non-falciparum malaria
Malaria due to P. vivax, P. ovale, P. malariae or P. knowlesi requires a standard course of treatment with chloroquine (Table 2). In resistant cases of P. vivax, Malarone® (atovaquone and proguanil), quinine plus tetracycline, or Lariam® (mefloquine) can be used.16 For P. vivax and P. ovale, malaria treatment with an 8-aminoquinoline (primaquine) is given to eradicate the exo-erythrocytic (liver) forms after levels of G6PD have been measured (Table 2).
Treatment of non-falciparum malaria.
Falciparum malaria
Mild falciparum malaria
A range of treatments is available depending on cost and choice of local practice (Table 3). There is increasing use of drug combinations such as Malarone® and Riamet® (artemether with lumefantrine), which are better tolerated than quinine. Lariam® may also be used. Quinine requires treatment to be followed up by a second agent such as doxycycline to prevent recrudescence.
Treatment of mild falciparum malaria.
Severe falciparum malaria
The management of severe falciparum malaria is a medical emergency. Patients with severe malaria should be transferred to the highest possible level of clinical care (eg a high-dependency or intensive therapy unit). Measurement of glucose, lactate and arterial blood gases should be performed in the initial assessment and blood taken for cross-matching and coagulation studies. Meticulous care must be given to fluid balance as both dehydration and overhydration can occur as a result of the disease or treatment.
Artesunate
An effective antimalarial, ideally intravenous (iv) artesunate, should be given (Table 4). Quinine is an alternative. Artesunate has distinct advantages over quinine in its effectiveness and toxicity profile. In large randomised trials, artesunate gave 35% reduction in mortality in Asian adults and children17 and 23% reduction in African children.18 Artesunate is not yet produced to good manufacturing practice, and hence does not have a product licence in Europe or Food and Drug Administration approval in the USA.
Antimalarial treatment regimens in severe falciparum malaria.
Artesunate can be used on a named patient basis, where available, in the UK and via an investigational-new-drug application from the Centers for Disease Control and Prevention in the USA.19
Blood and exchange transfusion
Blood transfusion may be of benefit in patients with respiratory distress and metabolic acidosis. In units with appropriate facilities, complicated hyperparasitaemia may be treated with exchange transfusion.20 The use of the latter is controversial, but should be considered for all patients in whom the parasitaemia exceeds an arbitrary 30%. It is also indicated in those in whom parasitaemia is lower but who have manifestations of severe complicated malaria, patients who have underlying medical conditions, are elderly or pregnant.21
Supportive management
Adequate fluid replacement, but avoiding fluid overload, is essential. Elective ventilation needs to be considered, especially if there is severe acidosis, evidence of raised intracranial pressure or respiratory failure of any cause. Dialysis or haemofiltration may be required. Bacterial superinfection is common in malaria and must be suspected and empirically treated with broad-spectrum antibiotics such as a third-generation cephalosporin.
Conclusions
Malaria must enter the differential diagnosis of any febrile patient who has travelled to an endemic area. In falciparum malaria, it is important to make the diagnosis promptly if the severe manifestations are to be avoided. The use of the artemisinin derivatives, most notably iv artesunate, has the potential to dramatically reduce the mortality of severe and life-threatening falciparum malaria.
- © 2011 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.