
Abstract
This lesson reports the case of a 32-year-old female presenting with left-sided homonymous hemianopia after a road traffic accident. A diagnosis of vertebral artery dissection (VAD) was missed at presentation after an initial computed tomography head scan was normal. Later, VAD was confirmed on neck magnetic resonance imaging. VAD is an uncommon cause of stroke in the young and, to date, there are no current emergency guidelines available for the management of patients with the condition.
Introduction
Traumatic vertebral artery dissection (VAD) is frequently unrecognised.1 It accounts for 20% of strokes in patients aged 45 and younger2 and up to 8% of those aged 60 and younger.3 It occurs in about 1% of patients following a blunt mechanism of injury.2 Dissection of the extracranial vertebral or carotid arteries are a relatively common cause of ischaemic stroke in the young.3,4 Dissection can cause ischaemic or haemorrhagic stroke although the latter is much more uncommon.5
The common symptoms of VAD at presentation include headache, vertigo, paraesthesia, neck and occipital pain.3 In addition, there is evidence from the existing literature describing ophthalmic symptoms occurring as the primary presenting complaint in 15–86% of cases.6,7 This lesson describes the case of a 32-year-old female who presented with left homonymous hemianopia secondary to traumatic VAD.
Lesson
Following a road traffic accident, a 32-year-old patient presented to accident and emergency with frontal headache radiating to the occiput, blurred vision, memory loss and neck pain. Initial examination revealed the patient to be haemodynamically normal. There was no spinal or abdominal tenderness and neurovascular examination was initially normal. Upon further examination she was found to have a left homonymous hemianopia. Magnetic resonance imaging (MRI) of the head showed evidence of multiple foci of signal abnormality in the cerebellum (Fig 1) and right temporal lobe with evidence of infarction in the right occipital lobe and smaller areas of signal abnormality in the left occipital lobe (Fig 2). Normal flow-voids were seen within the vertebral and basilar arteries with marginal enhancement. No evidence of any carotid abnormality was found on ultrasound scanning. Subsequent MRI imaging of the neck confirmed the suspected diagnosis of vertebral artery dissection, showing a narrowed segment of the right vertebral artery around C7. The patient was commenced on aspirin and dipyramidole and was discharged with follow-up under the neurologists. Ten months after the initial injury, the patient still has persisting visual impairment.
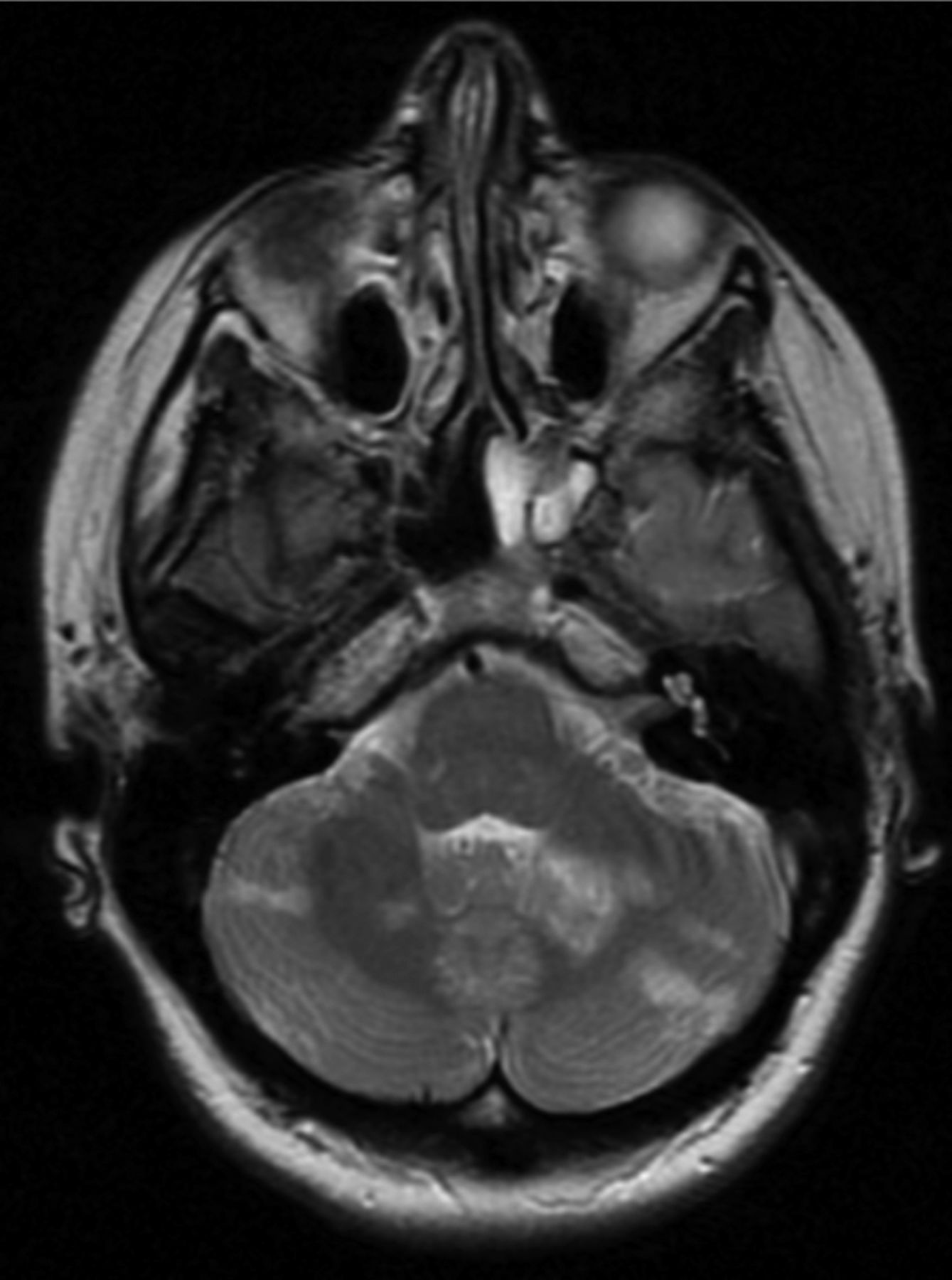
T2-weighted magnetic resonance image of the brain–multiple foci of abnormal enhancements are visible throughout both cerebellar hemispheres.

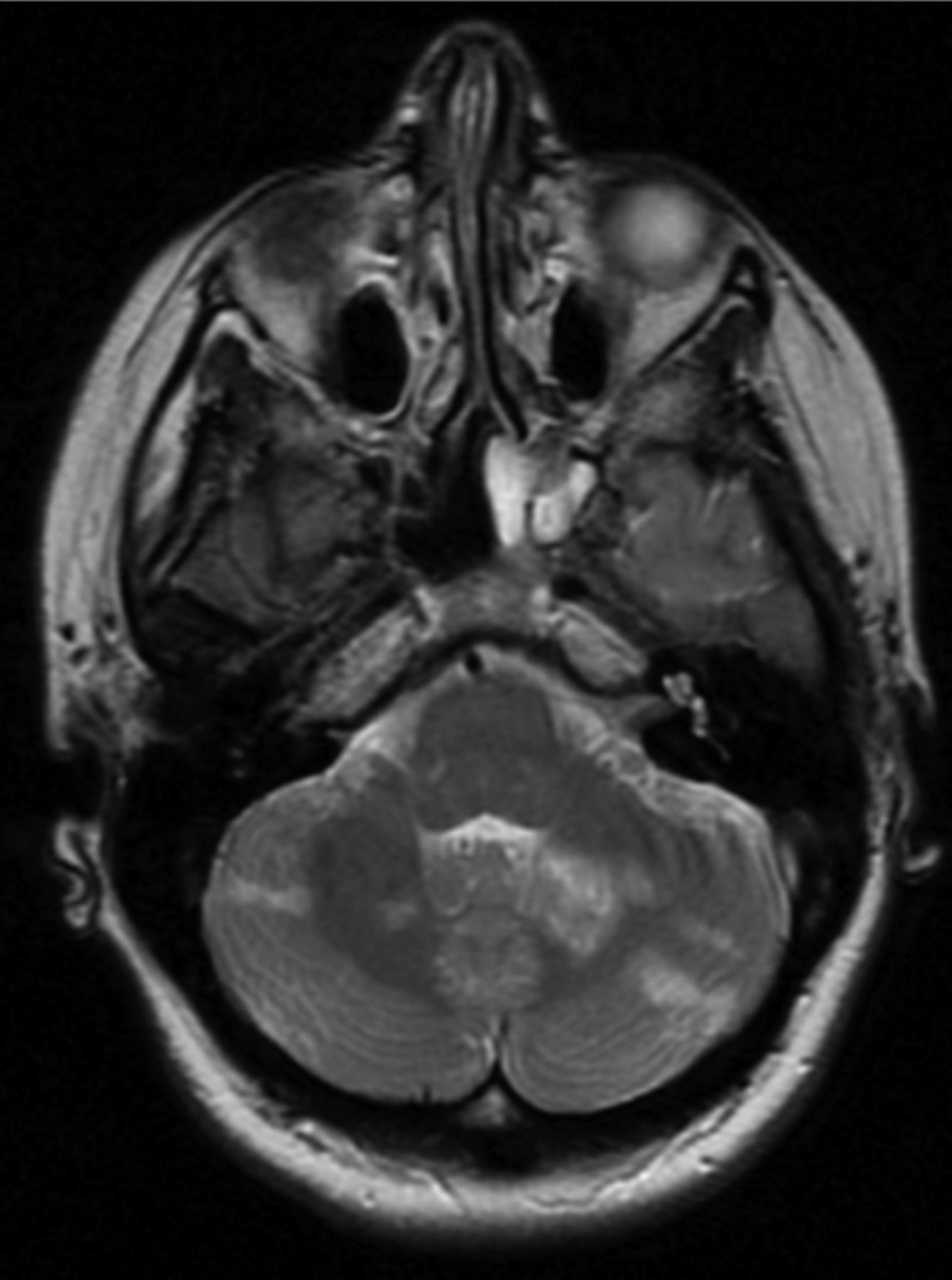
T2-weighted magnetic resonance image of the brain–showing foci of abnormal enhancement in the right occipital lobe.
Discussion
While VAD can occur spontaneously, some studies have shown that it occurs in relation to mild or significant trauma in up to 83% of cases.3 A literature review conducted between 1990 and 2004 showed that the main mechanisms of injury associated with VAD included: distraction/extension, distraction/flexion and lateral flexion injuries.8 VAD has been reported as a rare consequence of whiplash9 as illustrated in this case report. Due to the wide and variable symptoms, VAD is commonly misdiagnosed as musculoskeletal pain10 at presentation which can lead to a delay in treatment. Commonly vertebral artery dissection is diagnosed using MRI T1-suppressed axial images.11 It is generally accepted that VAD leading to ischaemic stroke is managed by anticoagulation10 or antiplatelet therapy.
Conclusion
VAD is a relatively common cause of stroke in the young and can present with a wide variety of musculoskeletal and neurological symptoms. Awareness of the condition is important in assuring that the diagnosis is not missed. Thorough neurological examination (including visual field testing) with appropriate imaging is essential in diagnosing those patients with suspected VAD. Neglecting these steps can delay treatment of patients and affect prognosis. To date, there are no current emergency guidelines available for the management of patients with VAD.
- © 2011 Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.