
Introduction
Alcohol was identified as a major risk factor contributing towards the global burden of disease in 1990.1 Today, it is the third leading cause of preventable and premature disease and disability worldwide,2 although it is the leading risk factor in middle income countries.3 Alcohol accounted for 3.8% of deaths globally (2.5 million people) and 4.6% of the global burden of disease (as measured by disability life years lost) in 2004.4 This equates to about half the number of deaths attributed to tobacco and approximately parallels the global burden of disease contributed by smoking and hypertension.2
Despite the clear and striking evidence related to the negative clinical, social and economic global impacts of alcohol, there is a distinct dichotomy between this knowledge and policy formation leading to implemented practice. In general, alcohol is under-recognised as a clinical and public health threat and most countries do not have adequate strategies in place to tackle alcohol-associated harms. Policies are often fragmented and do not reflect the magnitude of the health and social burdens alcohol harms place on society. Indeed, lesser health risks often have a higher policy priority. Advocacy for an alcohol policy is not seen as politically attractive and therefore, the political will to address this health hazard is almost universally lacking. Furthermore, commercial organisations carry significant strength in the alcohol debate and weaken many national and international policies, although this conflict between commercial and social interests has been largely addressed in the developed world in terms of tobacco-related health harms.
The World Health Organization (WHO) first recommended member states develop strategies to reduce the harmful use of alcohol in 1979.5 Today, 31 member states report having a national alcohol policy,3 however, the WHO's global alcohol strategy to reduce the harmful use of alcohol, endorsed by the 63rd World Health Assembly in 2010, is the first tangible global step to introduce an effective national and international response. This strategy aims ‘to reduce the harmful use of alcohol by giving guidance for action at all levels and setting priority areas for global action via a portfolio of policy options and measures that could be considered for implementation and adjusted as appropriate at national level, to take into account regional variations (eg religion, culture, public health priorities, resources, capacity and capability)’.6 In addition to this, the idea of a Framework Convention on Alcohol Control has been floated at the international level and is supported by the American Public Health Association, the Indian government, leading medical journals and the World Medical Association.7 Both proposals support an urgent need to put pressure on governments to recognise, adopt and scale-up appropriate policies.
Medical professionals are key in this initiative; not only is it their responsibility to address these issues as the frontline interface with individual patients and their families on a daily basis but, in addition, advocacy from expert medical professionals, together with non-governmental organisations, would hold ministries of health accountable for the lack of action. Pressure on governments to support initiatives at local, national and international levels is needed. The previous success of the tobacco campaign was, in part, centred on the unyielding medical pressure and smoking cessation advice at any opportunity available. This pressure and awareness needs to be translated to the alcohol arena.
This paper gives a background to the need for an international alcohol policy, such as the WHO global alcohol strategy. Furthermore, it focuses primarily on the individual medical professional's viewpoint and their essential role in the policy debate, particularly in relation to engagement in both advocacy and educational issues surrounding alcohol policy. Medical healthcare interventions to reduce, indeed in some instances prevent, the harmful consequences of alcohol use are crucial and have previously been neglected. Recognition and action by the medical community as part of an effective integrated pathway, incorporating psychological and social elements, is required. The effectiveness of any strategy is wholly dependent on the context and success in one arena does not always translate to other settings. Generic guidance can be provided using evidence-based strategies underpinning the policy, but regional and national adaptation to incorporate a wide variety of cultures and ensure effective local implementation is required. There is an urgent need to ‘upscale the issue in a downstreaming environment’, particularly given the current economic climate.
The scale of the problem
In 2004, WHO estimated that over two billion people worldwide consume alcohol and 76.3 million people had diagnosable alcohol misuse problems.8 Importantly, these figures are likely to be underestimates of the overall harm caused by alcohol, in part due to fact that evidence is largely restricted to high-income countries, with sparse or limited data from low or middle income countries. In addition, recent evidence suggests that the harmful use of alcohol contributes to the health burden caused by some communicable diseases, eg tuberculosis and HIV/AIDS,6 which further hinders accurate assessment of the global burden of alcohol-related harms. Furthermore, WHO estimates that nearly 30% of alcohol consumption worldwide is unrecorded,3 which is often not reflected in alcohol-related statistics but which will significantly impact resources utilised. Very few countries investigate levels of unrecorded consumption, but estimated levels suggest one-third of Russian alcohol consumption, eight litres of alcohol per annum for the average Ukrainian and 90% of East African consumption is unrecorded.8 Unrecorded alcohol production includes home production, travellers' imports, smuggled imports, below legal level alcohol beverages or alcohol preparations designed for alternative uses (eg industrial, chemical, technical or medical). Local and traditional alcoholic beverage production often lacks any regulation or monitoring for quality, strength and safety, which can lead to impurities, toxic components or higher potency beverages causing further health harms or death. Beverages made informally are often cheaper than commercially produced drinks and, therefore, the harmful consequences differentially affect the poorer segment of society and low income countries.
Drinking patterns
The burden of alcohol-associated disease is not equally distributed worldwide: alcohol has a unique geographical and sex distribution pattern. The majority of the worldwide population abstains from alcohol,3 however, some parts of the world have a longstanding tradition embedded in the culture of consuming it. Universally, alcohol causes more harm to males than females, reflecting the differing patterns and quantity of alcohol consumption.3 Overall, the heaviest toll of alcohol harms fall on men in Africa, in middle income countries in the Americas and in a few high income countries.2
Alcohol is the leading risk factor for morbidity burden in low mortality developing countries (compared to developing world with high mortality patterns, for example Africa and parts of southeast Asia, [where underweight, unsafe sex and unsafe water sanitation/hygiene are currently the leading factors, although it is predicted that alcohol attributable burden will increase with economic development])9 and the third highest risk factor in developed countries.
Alcohol is a major risk factor contributing to health inequalities and disproportionately affects low-income countries, where poor people have a higher relative burden of disease attributed to alcohol consumption, compared to high income countries and higher earners. Although the prevalence of drinking increases with increasing income,9 harmful and heavy alcohol consumption is associated with lower socioeconomic status, social withdrawal and marginalisation.10 Heavy alcohol consumption leads to decreased human capital, lowers achievement in schools and hence subsequent economic earnings,11 which in turn exacerbates poverty, widening the inequalities gap further.
The global average alcohol consumption is 6.13 litres of pure alcohol per year (per person aged 15 years or older), however, adults in the European Union, the highest consuming region, drink an average of 13 litres per year–2.5 times higher than the global average.3 Some evidence suggests that a low mortality risk level is around at two litres per year.12 This high consumption rate is compounded by increases in the alcohol strength by volume (bv): 5% bv lager has largely replaced 3.5% bv beer and 10–12% bv wine by 14–15% bv wine)13.
Problems faced by physicians
The health harms
The harmful consequences of alcohol are broad and encompass health and social problems for the drinker, the drinker's family, friends and community, in addition to general society (Table 1). These problems are well documented and are encountered by clinicians on a day-to-day basis. Alcohol harms are related to both the volume of alcohol consumed and the pattern of drinking, and often present at a relatively young age group (15–59 years).6 More than 60 types of harmful consequences are attributed to alcohol (disease and injury, Table 2, Fig 1), with a further 200 exacerbated by alcohol.3 Many of these consequences are preventable, or partially preventable with an appropriate enforced alcohol policy (eg ∼80% of liver death rates).14 Physicians must recognise and address these issues in order to develop successful strategies targeted at an individual, local or population level. These consequences are associated with substantial social and economic costs.
Alcohol use definitions
Key health harms associated with alcohol.
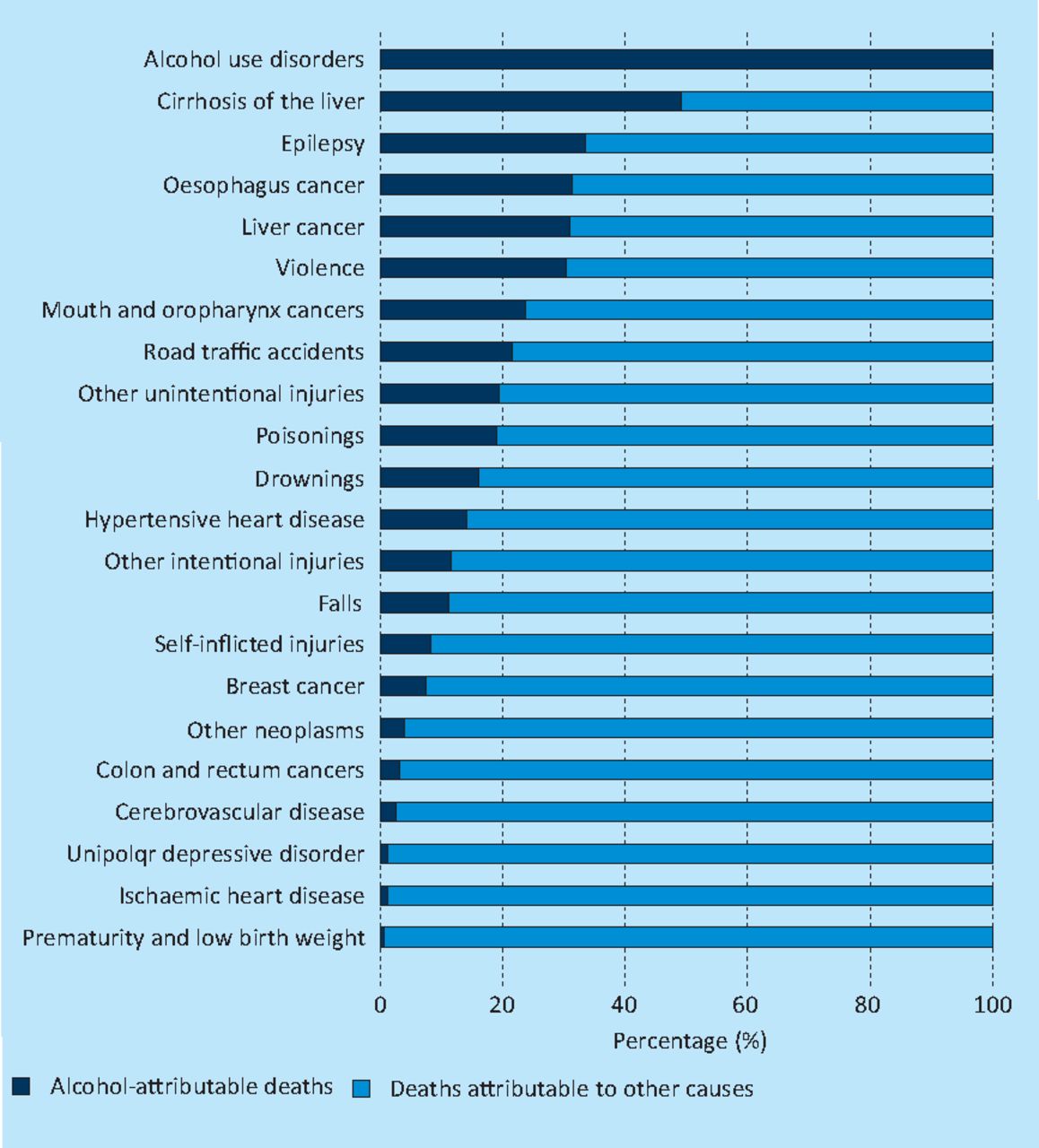
Global alcohol-attributable deaths as a percentage of total deaths by disease or injury 2004. The population-attributable fraction for diabetes mellitus is −0.1 and is, hence, not included in this figure. Reproduced from WHO Global Status Report on Alcohol 2011.3
Consumption of alcohol for health reasons should not be encouraged and this myth needs to be dispelled, as the harmful effects outweigh any medical benefit (cardiovascular disease and ischaemic stroke death protection). Health benefits are restricted to middle-aged, older adults with light to moderate, regular consumption, from countries with high cardiovascular morbidity rates,15 but the overall impact of alcohol consumption is harmful and all levels of consumption are associated with some form of risk.3 This is reiterated in the million women study, which demonstrated a 6% increased risk of cancer over the seven-year follow-up per 10 g of alcohol consumed daily.16 This fact is largely unknown and, therefore, it is misleading to suggest that people are making ‘informed’ decisions regarding their lifestyle choices.16
Passive drinking is increasingly recognised as a significant problem. It is a term relating to indirect harmful effects to a third party from alcohol use of others, for example the effect on a drinker's family, colleagues, victims of violence and traffic injuries. Indeed, domestic violence is strongly related to alcohol use, with 53% of cases linked to people ‘under the influence’.17
Policy challenges
The challenge is to reduce the harm caused by alcohol by strengthening alcohol policies globally, nationally and locally (Table 3). To do this, a multifaceted approach is needed with influence and commitment at all levels of the health, political and legal systems. The case for a strong population-level alcohol policy can be reinforced by the ‘prevention paradox’ theory, described by the epidemiologist Geoffrey Rose, where an intervention will have a small perceivable benefit to any one individual, but a large effect at the population level. Evidence-based cost-effective interventions have been demonstrated to reduce harm in an affordable manner, such as policies targeted at market controls, political reforms, production, buying power, urbanisation, migration, real price, marketing and trade.18 Most evidence centres on high-income countries, however some research (analysis and literature review) provides comparative knowledge to inform selected policy strategies globally.19 However, these policies have not been effectively implemented or gained strong political commitment to date.
Potential alcohol policies needed.
Policies that regulate the economic and physical availability of alcohol are effective in reducing alcohol-related harm.19 There is accumulating evidence to support the association between economic affordability and consumption of alcohol.20 In total, 75–80% of alcohol is consumed by the 20–25% of people who are misusing it and pricing policies will predominately target heavy drinkers, who purchase 15 times more alcohol, spend 10 times as much per year and pay 40% less per litre of pure alcohol (due to cheaper preferences) compared to the moderate drinker.21
Moreover, economic considerations should be evaluated in any policy decision. Estimates of the economic costs of alcohol, which include not only direct effects of alcohol use, but indirect effects, including lost work productivity and criminal justice costs, demonstrate that greater than 1% of the gross domestic product, adjusted for purchasing power parity, in high-income and middle-income countries is attributable to alcohol (excluding economic benefits).23 Latest UK data report alcohol-related costs in the region of £20–55 bn.24 However, economic modelling has suggested the potential for a total saving of approximately £15 billion over 10 years with minimum unit pricing policies (£0.50/unit).21
The international evidence base should be used to support implementation of effective alcohol policies. Finnish data demonstrated a 17% increase in alcohol-related sudden deaths (equivalent to eight additional alcohol-related deaths per week) when alcohol excise duty was reduced by an average of 33% (in order to increase cheap imports from abroad).25 In addition, important policy lessons and comparisons can be drawn between the global tobacco campaign, which has received international acclaim, in stark comparison to the alcohol campaign. Lessons learnt from this campaign can be applied to alcohol, for example, advocacy should concentrate on alcohol control measures/harm reduction; awareness of the links between increased consumption, harm and globalisation; reframing the problem; and building effective advocacy coalitions.
In England, the National Institute for Health and Clinical Excellence has recently conducted a comprehensive evidence review producing three linked alcohol-related guidance reports, including Alcohol-use disorders: preventing the development of hazardous and harmful drinking.26 This report made a number of recommendations including the need for pricing measures; changes to the licensing, availability and marketing regulation of alcohol; and the recognition that population policy level intervention alone will not be sufficient without health practitioner interventions at the individual level to reduce alcohol-related harms.
Advertising
The WHO expert panel in 2000 stated that ‘alcohol use is unlike other threats to global health. Infectious diseases do not employ multinational public relations firms. There are no front groups to promote cholera or lobbyists for malaria’.27 A power imbalance exists between the alcohol industry and healthcare professionals, which hinders progress in this arena. The alcohol industry is globalised and dominated by a few large companies with huge resources for sophisticated advertising and marketing techniques, including new social media and electronic technologies for younger people. Alcohol companies are the UK's second biggest sports sponsor and are branded on ‘star’ sportsmen, who serve as role models for many young people. Predatory/aggressive marketing is likely to increase sales, consumption and associated harm in most societies. Alcohol marketing is targeted at countries with growing economies, and hence increasing disposable income, and unregulated trade policies, such as Brazil, Russia, India and China.28 In the UK, the government's budget for alcohol education is dwarfed by the alcohol advertising budget of the drinks industry (45 times higher at £600–800 million/year).
The role of the health professional
Health professionals are in a unique position to be able to inform the alcohol debate and work together for concerted action as an effective advocacy coalition (eg the Alcohol Health Alliance (AHA) in the UK).29 Internationally, a formal professional clinical network is urgently needed to adopt this model and act together to reduce alcohol as a global problem.
Medical professionalism encompasses the responsibility to speak out, to show leadership and voice advocacy. It is a clinician's responsibility to not only look at the individual patient in front of them but also wider afield and recognise the broader impact of alcohol health harms and health inequalities. As Rudolf Virchow stated in Die medizinsche Reform ‘The physicians are the natural attorneys of the poor, and social problems fall to a large extent within their jurisdiction’. An important first step is to educate clinicians to ensure that they are aware of the strength of evidence base and encourage collaborative action to implement change. However, this is easier said than done and the level to which doctors can engage depends on circumstances and career stage. Doctors who show effective leadership can contribute significantly to the vision and aspiration. Therefore, health professionals, as a community, are one crucial component in the campaign to reduce the harm of alcohol. In addition, they should mobilise other stakeholders outside the health sector including engaging local politicians, the media, public health agencies, international development organisations, academic institutions, civil society and the private sector.
Conclusion
The public health and economic consequences of alcohol are well recognised, but to date policies to decrease alcohol-associated harms have, in many countries, been poorly considered, weakly implemented and often failed. A global perspective on such issues is urgently needed, backed by international and national political leaders, with access to fiscal, technical and human resources appropriate for the severity of this issue.
Alcohol-associated problems are entirely avoidable and a significant scientific knowledge base exists to inform policy on the health benefits and cost-effectiveness of strategies and interventions to prevent and reduce these harms. Acknowledgement of the varying characteristics associated with alcohol use in different societies and cultures is needed, together with recognition of the need for an integrated international and multiprofessional approach to tackle the diverse effects and consequences.
The WHO global alcohol strategy is the first cross-sector international initiative to encourage healthy debate and formulation of effective public health orientated policies (Table 4). This initiative demands political will, which requires the strong support, advocacy and endorsement of health professionals. An aggressive healthcare stance against the commercial interests of the drinks industry giants is needed. ‘Health must be foremost in policy decisions and not take a back seat to commercial interests.’30 Medical bodies must step up to the mark and play a key role in future developments, if the harm of alcohol is to be effectively reduced, as has been seen with tobacco as a consequence of international, multiprofessional targeted policies.
Five objectives of the WHO global alcohol strategy.6
Acknowledgements
We are grateful for the advice of the World Health Organization, Department of Mental Health and Substance Abuse.
- © 2012 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.