
Key points
Sleep-disordered breathing is common in obesity
The pathophysiology of obesity-related respiratory failure is complex
Diagnostic sleep studies should be performed to confirm the diagnosis, and appropriate respiratory management strategy implemented
The burden of obesity in the UK has increased significantly over the past 15 years. In 2008, the Health Survey for England demonstrated that 25% of the population were obese.1 Furthermore, only 36.8% of the population were considered to have a normal body mass index (BMI) and 61.4% were classified as either overweight or obese, with a year-on-year increase in the percentage of overweight and obese adults. The cost of obesity to the NHS, currently estimated to be £4.2 billion, is predicted to double by 2050.2
Obesity is associated with comorbidities such as systemic hypertension and diabetes mellitus, but over recent years the clinical effect of obesity upon the respiratory system has been highlighted. In addition to exertional breathlessness and limited exercise capacity, the adverse changes in pulmonary mechanics due to obesity can impact on patients with concomitant chronic respiratory illnesses, including asthma and chronic obstructive pulmonary disease. More importantly, it can result in sleep-disordered breathing, including obstructive sleep apnoea (OSA) and obesity-related respiratory failure (ORRF). This article reviews the respiratory complications of obesity, with particular attention to the changes in pulmonary mechanics and sleep-disordered breathing as these have significant clinical consequences.
Changes to pulmonary mechanics in obesity
Obesity has significant effects upon the pulmonary mechanics. BMI has a direct relationship with the degree of airways resistance and work of breathing, and is inversely correlated with thoracic lung volumes. Specifically, the reductions in functional residual capacity (FRC) and expiratory reserve volume are associated with early airway closure and resultant gas trapping, causing ventilation-perfusion mismatching and subsequent hypoxia. Obesity also imposes a restrictive defect due to the mass loading on the chest wall, with resultant reduction in chest wall compliance. Studies in anaesthetised obese patients have demonstrated a direct relationship between the degree of obesity and static lung compliance because of the reduction in FRC. Finally, breathing at low lung volumes causes expiratory flow limitation due to early airway closure with the generation of intrinsic positive end-expiratory pressure, again resulting in an increased work of breathing.
All these changes are further exaggerated during sleep due to the negative impact on the pulmonary mechanics of obese patients adopting the supine position.3–5
Sleep-disordered breathing
Sleep-disordered breathing is common in obese patients, with studies estimating the prevalence of OSA as 2–24% of the population.6,7
Obstructive sleep apnoea syndrome
OSA is defined as recurrent partial or complete upper airway obstruction during sleep. The clinical features have been discussed in a recent review article in this journal.8 Patients presenting with symptoms of OSA (eg snoring and witnessed apnoeas) should be screened for daytime hypersomnolence using the Epworth Sleepiness Scale.9 The combination of daytime symptoms and OSA is required to confirm the diagnosis of OSA syndrome.
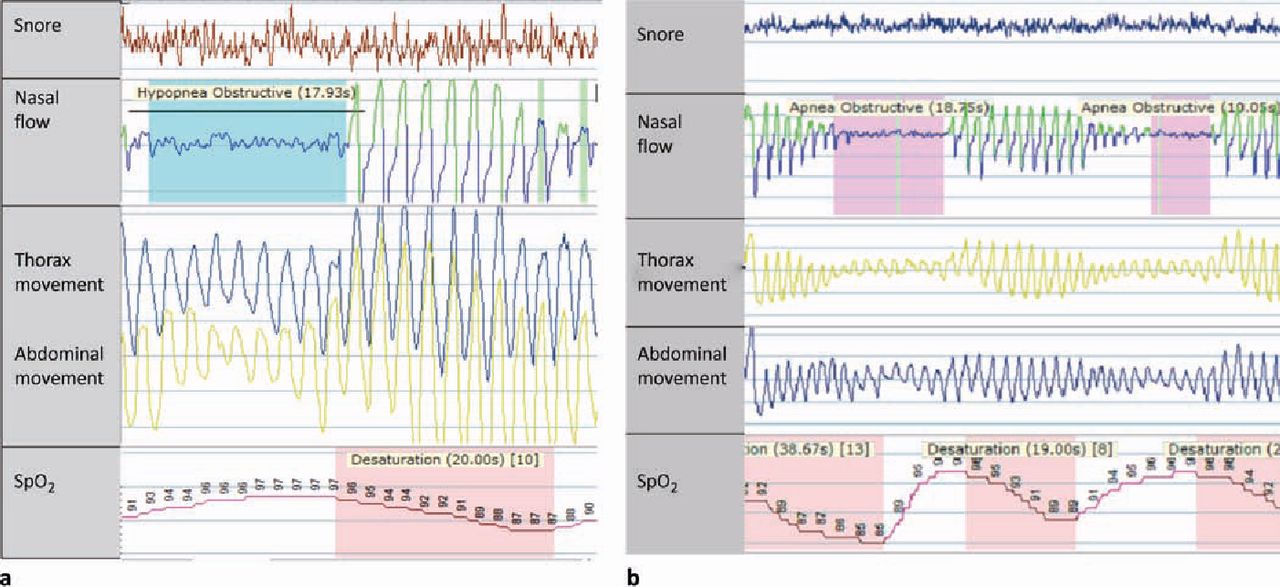
The diagnostic gold-standard for sleep-disordered breathing is nocturnal multichannel respiratory polysomnography (Figs 1a and 1b). Understandably, this type of complex monitoring study requires staff with extensive training and expertise, with significant associated costs, and has limited use throughout the UK. However, overnight home oximetry, which can be delivered to the patient's home as part of a remote monitoring service, is a relatively cheap and useful alternative which can both detect sleep-disordered breathing and also monitor the effect of treatment.
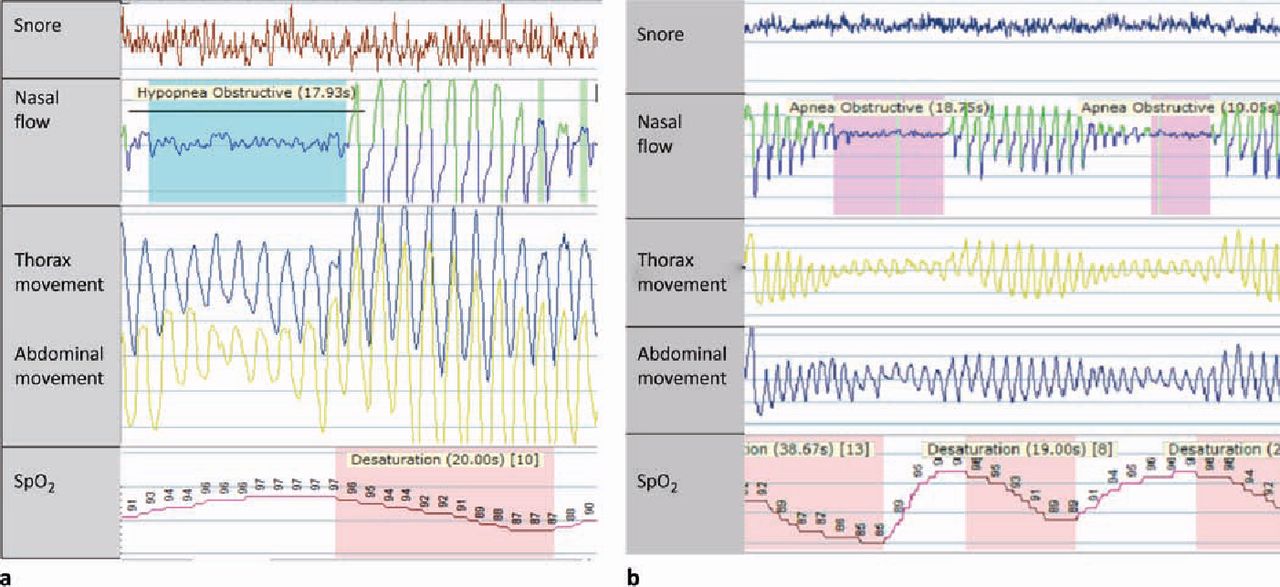
Multichannel respiratory polysomnography study from an obese patient with a body mass index of 35 kg/m2 with episodes of choking during sleep, witnessed apnoeas and daytime symptoms of hypersomnolence (Epworth Sleepiness Scale 14/24): (a) characteristic hypopnoea, with over 50% reduction from baseline in nasal flow and thoraco-abdominal movement, but some effort is still present; (b) characteristic obstructive apnoeas with complete cessation in nasal flow. An obstructive event is shown by paradoxical thoracic wall movement (thorax and abdominal bands moving in opposite directions) with reduction in airflow (hypopnoea) or absence of airflow (apnoea). Both hypopnoeas and apnoeas are followed by a fall in oxygen saturations (SpO2).
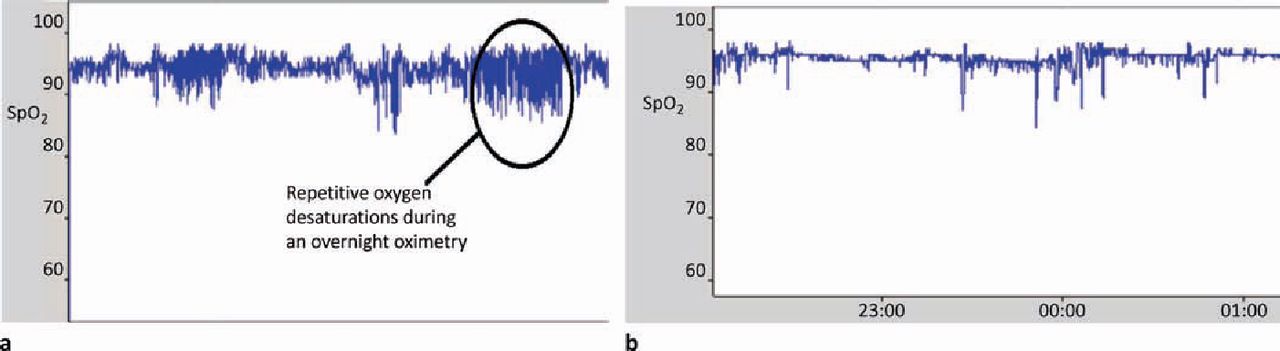
The mainstay of treatment for moderate to severe OSA syndrome is continuous positive airway pressure (CPAP), with studies demonstrating improvements in symptoms, mood, cognitive function and quality of life (QoL) measures. Mandibular advancement devices can be used in mild OSA syndrome but they are less effective than CPAP.10 Upper airways surgery is not recommended as treatment for patients with OSA, but those with tonsillar enlargement should be referred to a surgeon for consideration of removal. In addition, weight loss through self-motivation, optimised medical therapy and bariatric surgery is essential as this can significantly improve sleep-disordered breathing and, in some cases, be curative (Figs 2a and 2b).11
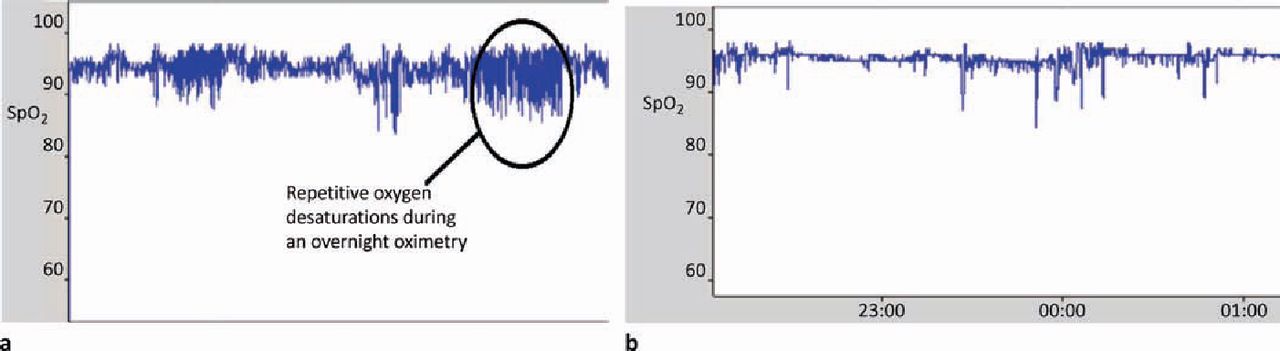
An obese middle-aged man with a BMI of 35.7 kg/m2 presented to clinic with snoring and daytime somnolence. Overnight oximetry demonstrated rapid repetitive oxygen desaturations, with a 4% oxygen desaturation index (ODI) of 51.2 events/h (a). He was commenced on CPAP and advised to lose weight. One year later the patient was less somnolent and his BMI had fallen though self-motivation to 28.3 kg/m2. A repeat study performed without CPAP treatment showed a markedly improved overnight oximetry study, with a 4% ODI of 8.2 events/h (b). CPAP was discontinued. Overnight oximetry: (a) rapid repetitive desaturations and resaturations from baseline, indicative of intermittent upper airways obstruction; (b) resolution of rapid repetitive desaturations and resaturations. SpO2 = oxygen saturations.
Obesity-related respiratory failure
ORRF encompasses three distinct clinical conditions:
severe OSA with associated hypercapnia
lone obesity hypoventilation syndrome (OHS)
combined OSA and OHS.
The traditional clinical approach has been to group these three conditions as OHS. However, this term does not clearly characterise the major underlying cause of the hypercapnic respiratory failure (eg OSA, OHS or a combination of both); therefore, the use of the term ORRF is clinically more useful, in particular in terms of clinical management.
Hypercapnic OSA, lone OHS and combined OSA and OHS.
The pathophysiology of hypercapnic respiratory failure in obese patients is not entirely clear as only one-third of obese patients develop chronic hypercapnic respiratory failure. In addition, it can be difficult to differentiate between eucapnic and hypercapnic OSA based on symptoms alone. Clinicians should be aware of the clinical features suggestive of OSA complicated by hypercapnia such as a high BMI and apnoea-hypopnoea index (AHI).12,13 The cause of hypercapnia in these patients with severe OSA has been shown to be a consequence of a reduced hypercapnic ventilatory response at the end of an apnoeic episode.14
Obesity hypoventilation syndrome.
Although the prevalence of OHS is relatively unknown, estimates indicate 0.4% of the North American population are affected.15 It is associated with increased healthcare utilisation, morbidity and mortality; physicians must be alert to the possibility of this diagnosis in obese patients.16,17 Prolonged desaturation episodes, not associated with apnoeas and hypopnoeas but rather with hypoventilation, are observed during polysomnography. These are demonstrated by reduced thoraco-abdominal movement and flow associated with a desaturation and rise in carbon dioxide. The mechanisms underlying OHS are not fully understood. Although an imbalance between the neural respiratory drive, respiratory muscle load and respiratory muscle capacity results in alveolar hypoventilation and hypercapnia, the contribution of each has not been measured. Studies have shown that the increased respiratory muscle load is due to an increase in the resistive, elastic and threshold load (Table 1).
Components of the respiratory load contributing to obesity-related respiratory failure.
The changes in lung volume and respiratory system compliance in people with simple obesity are all more evident in OHS. There is an increased load on the diaphragm as a result of the increased abdominal pressure and reduced abdominal compliance. This in turn reduces the caudal excursion of the diaphragm and therefore reduces alveolar ventilation. In simple obesity, subjects tend to breathe more rapidly at lower tidal volumes as a strategy to reduce the respiratory muscle load and avoid hypoventilation. However, this response is absent in patients with OHS, resulting in hypoventilation. Studies have demonstrated neural respiratory drive is elevated in simple obesity compared with non-obese subjects,18 a response which may be altered in those with OHS.19 Both hypercapnic and hypoxic ventilatory challenges are blunted in OHS patients compared with simple obese patients, such that there is less ventilation for a given level of oxygen and carbon dioxide.20 Furthermore, hypercapnia and hypoxia cause sleep fragmentation which may further blunt the hypercapnic and hypoxic ventilatory response.21
Studies estimate that up to 30% of patients with OSA have OHS.22 The mechanism of hypercapnic respiratory failure in these patients is presumed to be a combination of a blunted hypercapnic ventilatory response at the end of an apnoeic episode and an imbalance between the increased respiratory muscle load and reduced respiratory muscle capacity, resulting in alveolar hypoventilation. However, more studies are required in this area.
Respiratory management of obesity-related respiratory failure
The respiratory management of patients with ORRF is not straightforward and a clear management strategy must be established. Studies have suggested that both CPAP and bilevel non-invasive ventilation (NIV) are useful modes of treatment for OHS.23,24 NIV maintains upper airway patency, reduces respiratory muscle loading and improves gas exchange leading to an improvement in daytime symptoms and QoL.
A practical and rational approach to management is the following (Fig 3):
consider CPAP therapy alone for the treatment of hypercapnic OSA, although the reduction in PaCO2 is more rapid with bilevel NIV
bilevel NIV is required for lone OHS, and
combined OSA and OHS patients should be considered for bilevel NIV.

Respiratory management strategy for obesity-related respiratory failure. ABG = arterial blood gas; BMI = body mass index; CPAP = continuous positive airway pressure; OHS = obesity hypoventilation syndrome; OSA = obstructive sleep apnoea.* Patients with lone OHS will need to continue bilevel non-invasive ventilation.
Conclusions
It is evident that the impact of the obesity epidemic extends beyond the metabolic and cardiovascular complications. The respiratory complications of obesity are common and clinicians should determine if obese patients have features of snoring and excessive daytime somnolence. These patients should be screened for sleep-disordered breathing with home oximetry monitoring or, if required, respiratory polysomnography–bearing in mind that half of all patients with a BMI above 40 kg/m2 have OSA25 and one-third of obese patients have hypercapnic respiratory failure. Clinicians should consider a daytime arterial blood gas measurement in patients with sleep-disordered breathing with a high AHI, a low vital capacity and a low clinic SpO2.
Although there is an increase in our understanding of the respiratory complications and treatment of obesity, there are still unanswered questions, in particular, the pathophysiological mechanisms underlying hypercapnic respiratory failure and the optimum respiratory management. However, more importantly, clinicians and the healthcare policy makers need to develop major strategies to prevent and effectively manage obesity.
Competing interests
The authors acknowledge financial support from the Department of Health via the National Institute for Health Research (NIHR) comprehensive Biomedical Research Centre award to Guy's & St Thomas' NHS Foundation Trust in partnership with King's College London and King's College Hospital NHS Foundation Trust.
- © 2012 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}