
Abstract
The role of cardiac computed tomography (CT) in the assessment and management of patients with suspected cardiac chest pain has been formally recognised in NICE guidance 95. When the technique and patient selection are appropriate, cardiac CT is a valuable diagnostic tool, particularly for patients with a low to intermediate pre-test probability of coronary artery disease. The physician must be aware of the implications of the recent guidelines; hence, we present an illustrated synopsis on the current technique and the indications for the use of calcium scoring and cardiac CT in the assessment and management of patients with suspected cardiac chest pain.
Introduction
Coronary artery disease (CAD) is a leading cause of morbidity and mortality. Across Europe, the annual incidence of hospital admission for myocardial infarction (MI) is in the range of 90–312/100,000.1 There are over 124,000 MIs and more than 50,000 premature deaths resulting from cardiovascular disease annually in England and Wales.2
Invasive coronary angiography (ICA) is the current reference standard for imaging the coronary arteries. Recent advances in multi-detector row computed tomography (MDCT) and magnetic resonance imaging (MRI) mean that the clinician now has access to a range of imaging modalities with which to investigate both patients with acute coronary syndromes and those with chronic symptoms.
The National Institute of Clinical Excellence (NICE) recently published guidance on the investigation of chest pain of suspected cardiac origin.3 The guidelines formally recognise the role of coronary CT in the management of chest pain. Referring physicians must be aware of the current indications and limitations of this established technique.
This article summarises the indications for and role of coronary CT as defined in the NICE guidelines, before discussing the technique further and highlighting how CT results influence patient management.
NICE guidance and coronary CT
Used appropriately, coronary CT is a useful and safe clinical tool. Nevertheless, the ready availability of high-end technology is no substitute for optimal pre-test clinical assessment, and the recent NICE guidance highlights the importance of a full clinical assessment and accurate selection of candidate patients for CT.3 In the guidance, the assessment and diagnosis of patients with chest pain of suspected cardiac origin is covered by two separate diagnostic pathways. The first, for patients with acute chest pain in whom acute coronary syndrome (ACS, including MI and unstable angina) is suspected, stresses that early CT should only be considered to rule out alternative diagnoses, such as aortic dissection or pulmonary embolism. It is not a diagnostic test for ACS and there is no role for coronary CT in these patients.
It is the second diagnostic pathway, for patients with intermittent stable chest pain and suspected stable angina who might or might not have previously confirmed CAD, in which a role for coronary CT is defined. The aim of the pathway is to diagnose angina, not to simply screen for CAD. The investigation aims to diagnose either myocardial ischaemia (by non-invasive functional testing) or luminal stenosis (by anatomical imaging). To some extent, the choice of test depends upon the local availability of equipment and expertise.
Exercise electrocardiogram (ECG) is not recommended for the diagnosis or exclusion of stable angina and is not used for diagnosis in patients without a history of CAD. As with any test, its sensitivity and specificity depend on disease prevalence in the tested group. The sensitivity and specificity of exercise ECG varies with clinical history, extent of disease and treadmill performance. The consequence is low accuracy in those with a low pre-test probability (poor sensitivity), so a negative test is unhelpful. Conversely, if the patient has typical angina, an exercise test is not helpful in excluding or confirming angina as a negative test is likely to be a false-negative (poor specificity).
In patients with a >90% likelihood of CAD, the diagnosis of angina is assumed. In those with a <10% likelihood, the diagnosis is deemed unlikely and not requiring further investigation unless symptoms persist. Nevertheless, risk factors must be addressed. All other patients without previously confirmed CAD are offered appropriate diagnostic investigation, the choice of which depends on their estimated likelihood of having CAD (Table 1). We emphasise that these likelihood percentages refer to the probability that significant CAD (ie >50% luminal stenosis) is the cause of the symptoms, as almost all patients (and particularly asymptomatic elderly patients) have CAD that is often of no clinical significance. The estimated likelihood of having CAD is determined by clinical assessment, 12-lead ECG, and typicality of symptoms, age, sex and risk factors as shown in the NICE guidance.
Recommended diagnostic investigations for patients presenting with stable chest pain (NICE).
The NICE guidance advocates use of coronary CT in patients with a likelihood of CAD of 10–29%. In these patients, the purpose of imaging is to rule-out CAD. Coronary CT has a high sensitivity (98%) and specificity (85%)4,5 and a high negative predictive value (99%).6,7 Its positive predictive value, however, is potentially low (as low as 48%) because CT can overcall stenosis severity and local coronary calcium may obscure the lumen leading to overestimation of severity.6 There is a lack of long-term prognostic studies of patients with stable chest pain, but the absence of a >50% stenosis on coronary CT is associated with a low myocardial event rate.8 The high sensitivity and high negative predictive value of coronary CT support its role in ruling out CAD.
In patients with a high pre-test probability (>61%) of significant CAD, a rule-in test is required and ICA is recommended as the most cost-effective method of imaging the coronary arteries, allowing simultaneous revascularisation. Coronary CT is more likely to be indeterminate or inaccurate in these patients than in those with a lower pre-test probability of CAD because of the greater likelihood of coronary artery calcium burden.9 In addition, as many of these patients will have significant stenoses (that might benefit from revascularisation), performing a CT will merely lead to a delay in treatment and additional unnecessary costs. In patients with a moderate pre-test probability of CAD (30–60%), non-invasive functional imaging is recommended as the most cost-effective test to detect myocardial ischaemia.
In very low pre-test probability patients, incidental coronary calcification without flow-limiting stenosis reduces the usefulness of coronary CT. In such patients, it is as yet unclear whether CT provides advantages additional to those offered by basic testing and clinical acumen. If, however, there remains concern that the pain of a patient with a low pre-test probability of CAD might be of cardiac origin, coronary calcium scoring is likely to be cost-effective as a first-line test strategy, helping to discriminate those who have CAD from those who do not.
Patient selection
A candidate for coronary CT according to the guidelines might be a 66-year old lady who is referred to the cardiology clinic with a three-month history of exertional dyspnoea and chest pain. The pain is not typically crushing, neither is there radiation to the shoulders, neck or jaw. Symptoms typically last between 3 and 5 min and are relieved by rest. Before the onset of these symptoms, the patient has been fit and well. The remainder of the patient's history is unremarkable with no cardiac risk factors (in particular reference to the NICE guidance, there is no history of diabetes, smoking or hyperlipidaemia). The physical examination and resting 12-lead ECG are normal.
This patient has a history that suggests atypical angina (see Box 1) and has a likelihood of CAD of 20% (based on the NICE guidance). She should be offered an investigation such as coronary CT to exclude CAD. Contra-indications to coronary CT include those of any contrast-enhanced CT, including inability to lie flat, significant renal impairment or contrast allergy. Dysrhythmias, tachycardia and inability to breath-hold for about 5 sec reduce the quality of the images obtained. Pacemakers and heart valves are usually fine as any beam-hardening artefact that they cause is not usually significant enough to preclude assessment.
The differentiation between typical angina, atypical angina and non-anginal chest pain (NICE).

Performing coronary CT
Pre-medication (often beta-blockers if the patient is not already taking them) is usually prescribed prior to coronary CT to reduce the heart rate. On arrival in the imaging suite, the patient will be talked through the procedure by a radiographer and asked questions regarding allergies, previous medical history and medications. Intravenous access will be obtained. The patient will be able to ask questions of the radiographers and will be accompanied into the CT scanning suite, where they will be asked to lie supine on the CT scanner couch and will be connected to ECG electrodes. These are attached to the CT scanner and enable ECG-gated image acquisition. Further intravenous beta-blockers (often metoprolol) are commonly used to reduce the heart rate to about 60 beats per minute, enabling optimum image acquisition. IV metoprololol takes up to 20 minutes to reach peak plasma effect. Blood pressure (BP) should be monitored during the administration of beta blockade and nitrates. Usually, no more medication is given if BP is <100mmHg systolic.
Once the patient is fully prepared, the recommended first step in coronary CT is the generation of a calcium score (Fig 1). This score is usually obtained by a ‘prospectively’ gated unenhanced study of the heart. An operator selects vessels with observable calcium and the computer then derives the score based on the Agatston equivalent scoring system.10

a) A scout topogram is used to plan the study. The scan range extends from below the carina to below the level of the heart. b) An unenhanced study of the heart is performed. c) This enables the generation of a calcium score. The region of red highlighted by blue demonstrated calcification in the circumflex artery. The total calcium score is shown in the box at the bottom left of the image.
If the decision is made to proceed with CT coronary angiography (CTCA), administering sublingual nitrate prior to the scan improves visualisation of the coronary arteries. Sublingual nitrate takes 5 to 6 minutes to reach peak plasma effect.11,12 Nitrate should be avoided if the patient is taking a phosphodiesterase inhibitor (such as sildenafil (Viagra)), which could precipitate pronounced hypotension. A medium bore cannula (ideally 18 gauge) in an antecubital fossa facilitates high flow (5–7ml/sec) of viscous iodinated contrast (350–400mg/ml strength) to achieve optimal coronary artery opacification. A test bolus using a small volume (20ml) of contrast can be administered and the density of contrast in the ascending aorta tracked over time. This determines the patient's circulation time and hence the optimum time for triggering the scan to ensure maximal opacification. This method is usually preferred to the bolus-tracking technique, in which the main injection is given and the scan triggered when sufficient contrast is seen in the ascending aorta; this can be problematic in patients with haemodynamic impairments such as severe valvular regurgitation, ventricular dilatation or ventricular impairment. For a diagnostic CTCA, approximately 70–100ml contrast is required.
Initial studies showed that the use of high iodine concentration agents at high flow rates resulted in better vessel attenuation,13 but lower volumes, rates and concentrations can also achieve good results.14,15 The ideal attenuation required for accurate vessel imaging is approximately 400 Hounsfield units.15 Greater volumes of contrast at higher flow rates are often needed when imaging larger patients who have heart failure; this could raise concerns about volume overloading and renal dysfunction.
Variation in the patient's heart rate during breath-holding will also be assessed prior to scanning to ensure that this is <10% as greater variability degrades image quality. Scanning is performed in relaxed inspiration because of the physiological effects of elevated intrathoracic pressure (Valsalva manoeuvre), which can reduce the inflow of contrast medium.
ECG-gating enables the collection of data from the same point in the cardiac cycle over consecutive heart beats, which are then used to generate images. Motion-free images can be obtained by reconstructing data captured during those periods of the cardiac cycle when there is least motion (usually mid to late diastole). ‘Step’ reconstruction artefact is much less of a problem with later-generation scanners that have more detector rows (‘slices’), eg 128 and 320, as these machines are able to image more of the cardiac volume with one rotation, resulting in fewer ‘slabs’ of data to be combined to form an image. The evidence used to formulate the NICE guidance was based on studies that used at least 64-slice CT.
The technique most commonly implemented in coronary CT is retrospective ECG gating, in which data are acquired continuously but only those from specified periods of the cardiac cycle are reconstructed, rather like frames of a movie. Retrospective gating should be used with ECG-gated tube current modulation. This avoids exposure to the full ionising radiation dose required for scanning during those parts of the cardiac cycle when diagnostic data are unlikely to be obtained, ie during ventricular systole. The full dose is used only in mid to late diastole as this is the period when cardiac motion is least and so the most useful data will be obtained.
Other dose-reduction techniques, such as lower kilovoltage (kV) scanning in slim patients, are also required to reduce the radiation exposure in this potentially high-dose scan. Prospective gating can lower the dose further.16 When this technique is used, an axial block of data are acquired in mid-diastole during one heartbeat, then the table position changes. A second acquisition is then performed to image the next part of the volume, and the table moves again until the coronaries have been covered fully (this is called the axial sequential technique and fewer sequential volumes are needed with wider detector-row scanners). This technique does not allow functional analysis and is susceptible to distortion in patients whose R-wave-to-R-wave interval varies. This technique should be employed carefully and selectively as any significant motion artefact can render the study non-diagnostic in inexperienced hands. Further issues concerning dose are discussed in Box 2.
Some of the issues concerning dose.

Whichever gating technique is employed, the area to be scanned will be delineated on a ‘scout’ view (low-dose topogram of the chest). For a typical coronary CT, this covers the volume from just below the carina to below the level of the heart. The contrast injection is started and the scan is triggered once optimum contrast opacification has been achieved. Prior to this, the patient will be asked to breathe in and hold their breath for the few seconds it takes for the scan to be performed. The patient will then be disconnected from the ECG electrodes and their tolerance of the scan confirmed. Because of orthostatic effects of beta-blockade and nitroglycerin administration, the patient will be asked to get up slowly. After a brief period of observation in the department, the patient is free to leave. The entire CT scan should take less than 10–15 minutes and often the greatest delay comes with the necessity to administer iv beta-blockers to reduce heart rates that are too high. Pre-medication with oral beta-blocker is thus recommended. Curved multiplanar reformats and 3D volume rendered images can then be obtained to assist in the assessment of the coronary arteries (Fig 2).
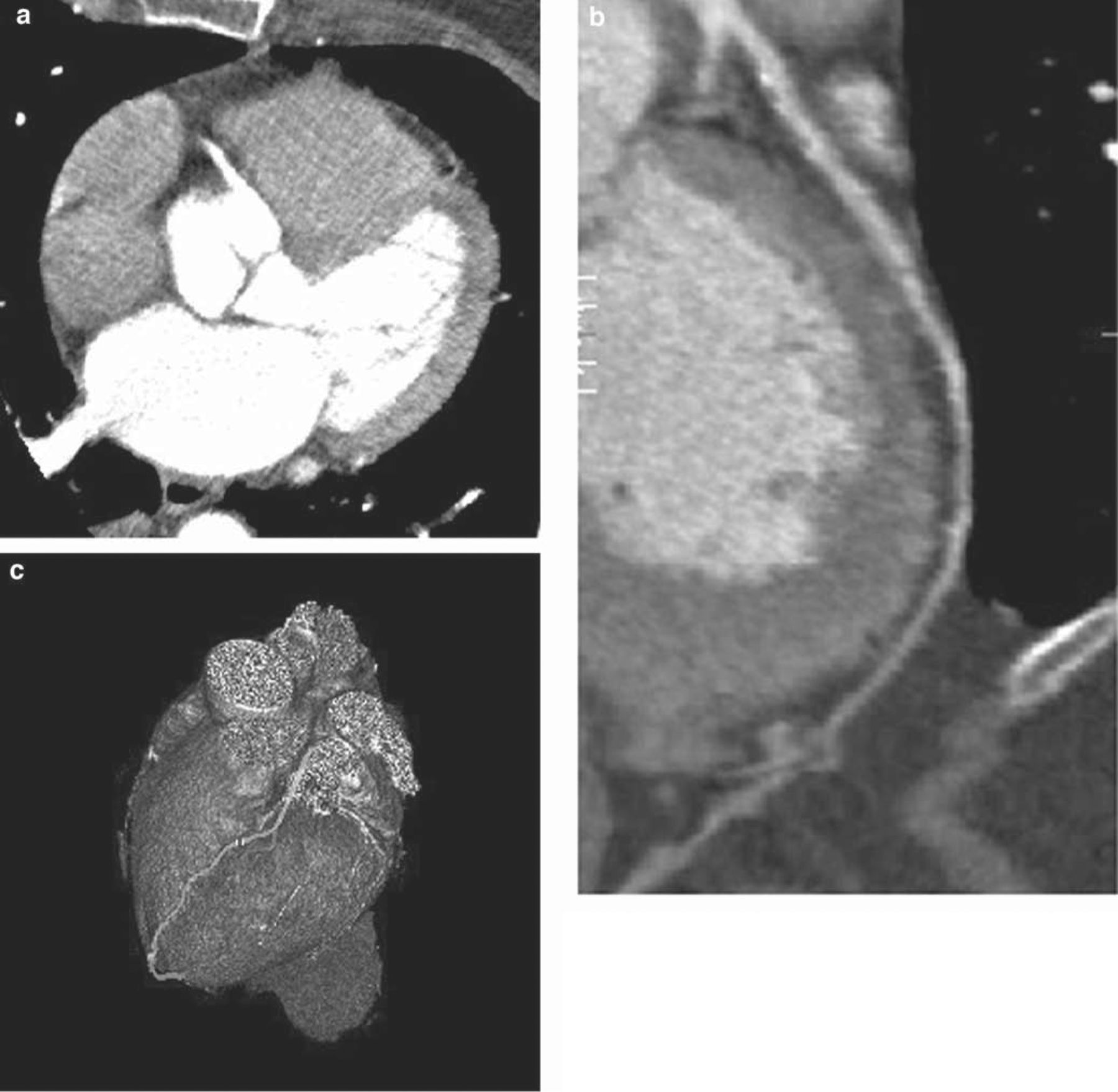
a) A further helical acquisition following iv contrast is performed to obtain the coronary angiogram. b) Curved multiplanar reformats can be generated allowing visualization of the coronary artery in a single plane, in this case the left anterior descending (LAD) coronary artery. c) 3D volume rendered coronary angiogram with the LAD highlighted in yellow.
Calcium score
There are clear recommendations in the NICE guidance regarding the implications of the calcium score and the need for further investigation.3 The calcium score is discussed further in Box 3 and the implications of calcium scores of zero, 1–400 and >400 are as follows:
The calcium score.
Outcome 1: calcium score of zero
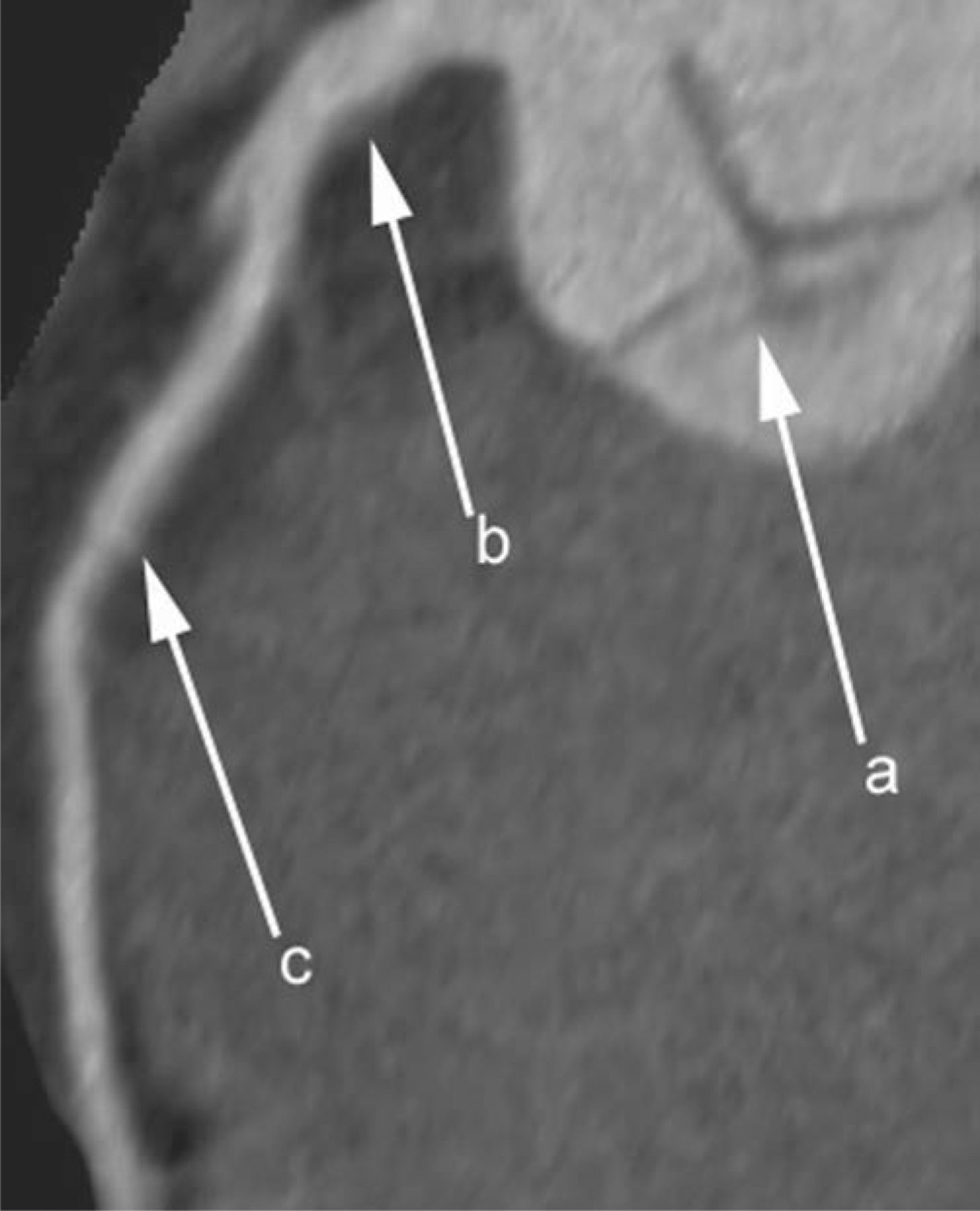
A calcium score of zero confers excellent cardiovascular prognosis and is taken to exclude CAD with a high degree of accuracy – sensitivities of up to 99% have been recorded.17 Other causes of chest pain should be considered and no further testing for CAD is required. Nevertheless, some controversy surrounds this score: it does not completely rule out atherosclerosis as non-calcified fibrolipid plaque, such as that shown in Fig 3, can be missed.18 Calcium score was initially developed for use in asymptomatic patients and although the false-negative rate associated with scores of zero is not known, recent studies have identified significant CAD in acute symptomatic patients with a score of zero.19,20 Medical therapy should be optimised and imaging considered on a case by case basis – some centres will still proceed to CTCA particularly in young symptomatic patients who are more likely to have non-calcific atherosclerosis. Others advocate retesting, although the interval for retesting patients with a zero calcium score should not be in less than 4–5 years.21
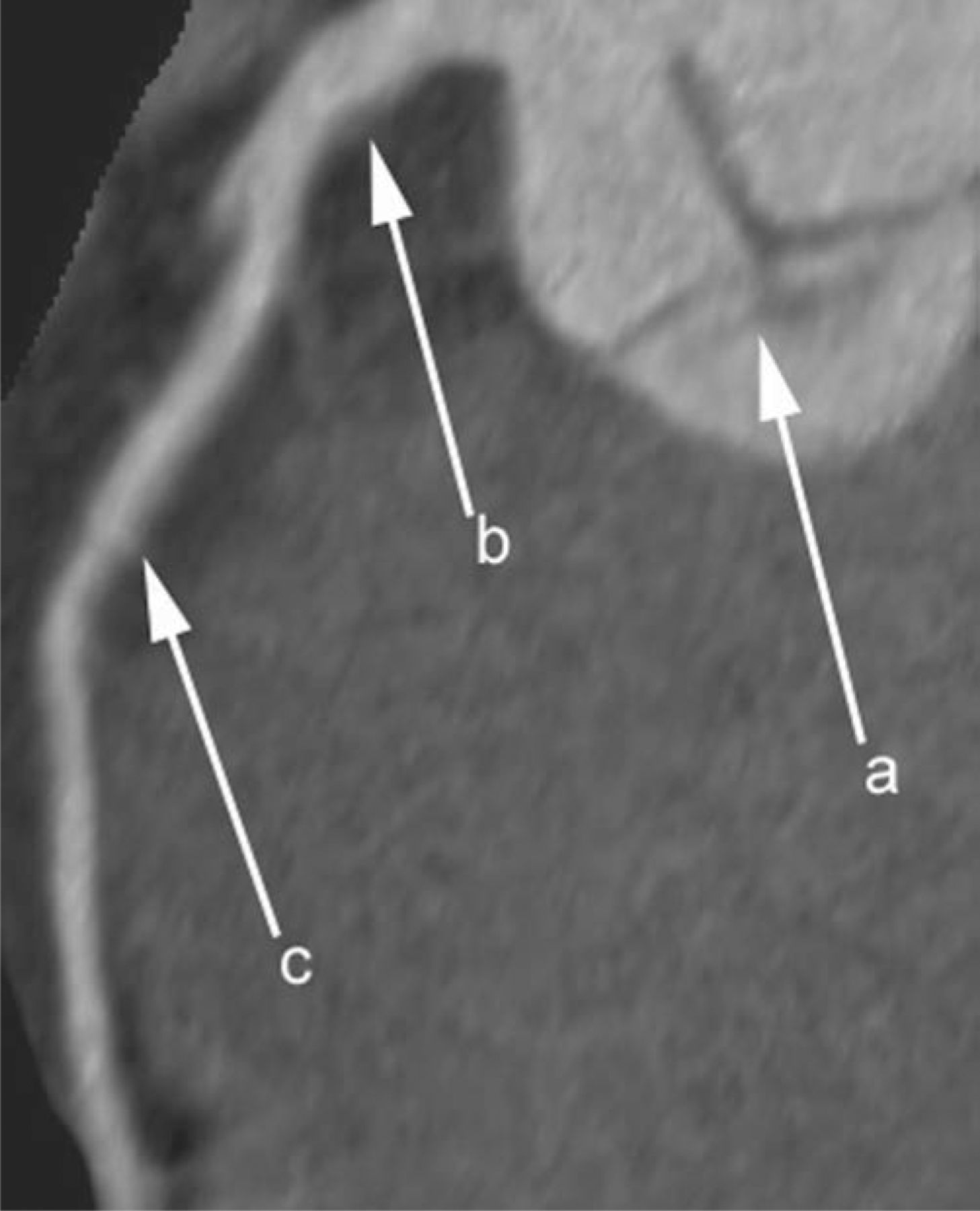
Multiplanar reformat of CTCA demonstrating shallow fibrolipid plaque in the left main stem and no coronary artery calcification. a = aortic valve, b = shallow plaque in left main stem, c = left anterior descending (LAD) coronary artery. The patient had atypical chest pain and a calcium score of 0. He was discharged and medical therapy optimised.
Outcome 2: calcium score 1–400
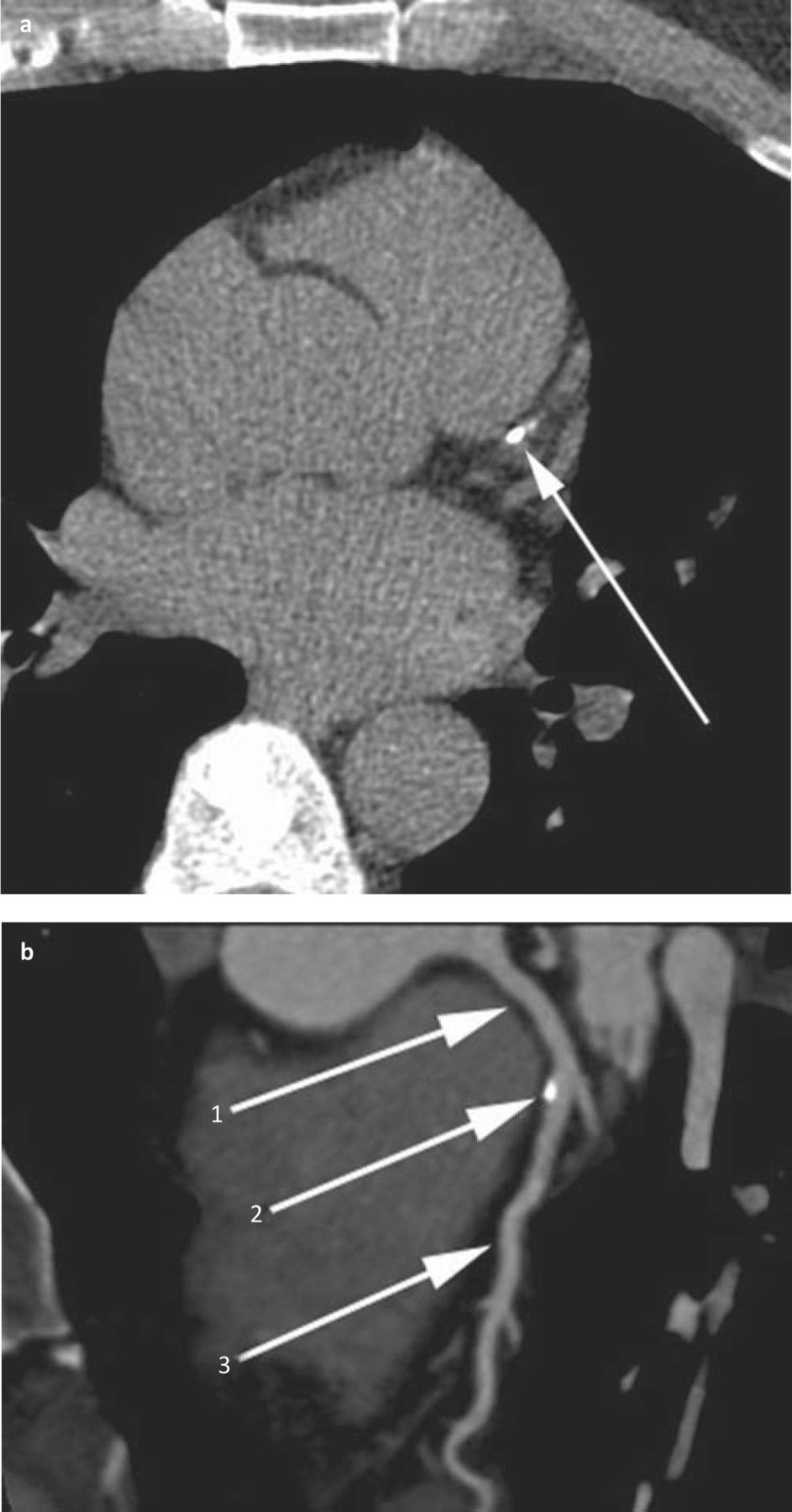
If the calcium score is between 1 and 400 the recommendation is to proceed to formal CTCA. The patient whose coronary CT is shown in Fig 4 had atypical chest pain and CTCA excluded significant CAD. The patient was discharged on optimised medical therapy.
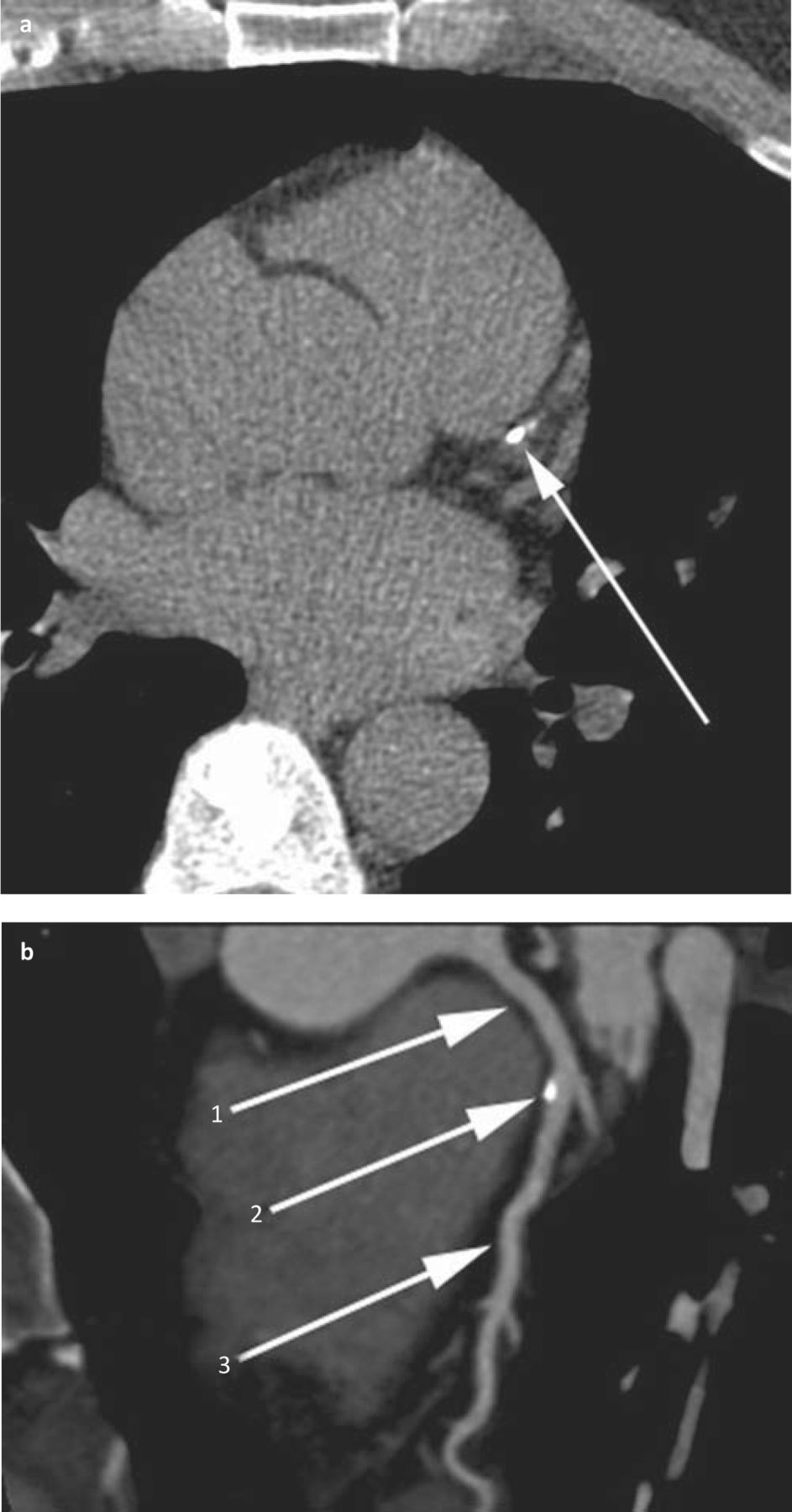
a) Axial unenhanced coronary artery score scan demonstrates calcification in the proximal left anterior descending (LAD) coronary artery (arrow). The calcium score was low (60) and so the patient proceeded to CTCA. b) Multiplanar reformat of CTCA demonstrates calcified eccentric plaque in the proximal LAD coronary artery (1 = left main stem, 2 = calcified plaque, 3 = LAD) but no stenosis. The patient has non-stenotic coronary artery disease and medical therapy was optimised.
Outcome 3: calcium score .400
If the calcium score is >400 the recommendation is to proceed to formal ICA. CTCA is unlikely to be useful in the presence of such a high calcium score.9 The patient whose coronary CT is shown Fig 5 was referred for ICA, which showed mild luminal disease but no significant stenosis.

a) Axial unenhanced coronary artery score scan demonstrates calcification in the right coronary artery (arrow) and b) heavy calcification of the LAD (arrow). The patient had a very high calcium score of over 3000 precluding accurate CTCA. The patient suffered atypical chest pain and was referred to cardiology for ICA. c) LAO cranial view of the left coronary arterial system demonstrating proximal LAD luminal irregularity (arrow) but no luminal compromise.
Other uses of coronary CT
Authorities in some expert centres might extrapolate the use of CT into intermediate pre-test probability groups (up to 60%) and there is emerging evidence to support this strategy. The use of CTCA in the emergency setting, while potentially enabling CAD to be ‘ruled out’, will also result in the detection of a cohort of patients who have sub-clinical CAD that is not the cause of their presenting chest pain. The exact role of ECG-gated CTCA in the emergency setting has not yet been fully defined and has implications for service provision and cost-effectiveness.22 Research continues regarding the cost-effectiveness of CTCA in the triage of patients with acute chest pain, but it could reduce length of stay and the number of less-reliable non-invasive tests, such as an exercise ECG, performed.
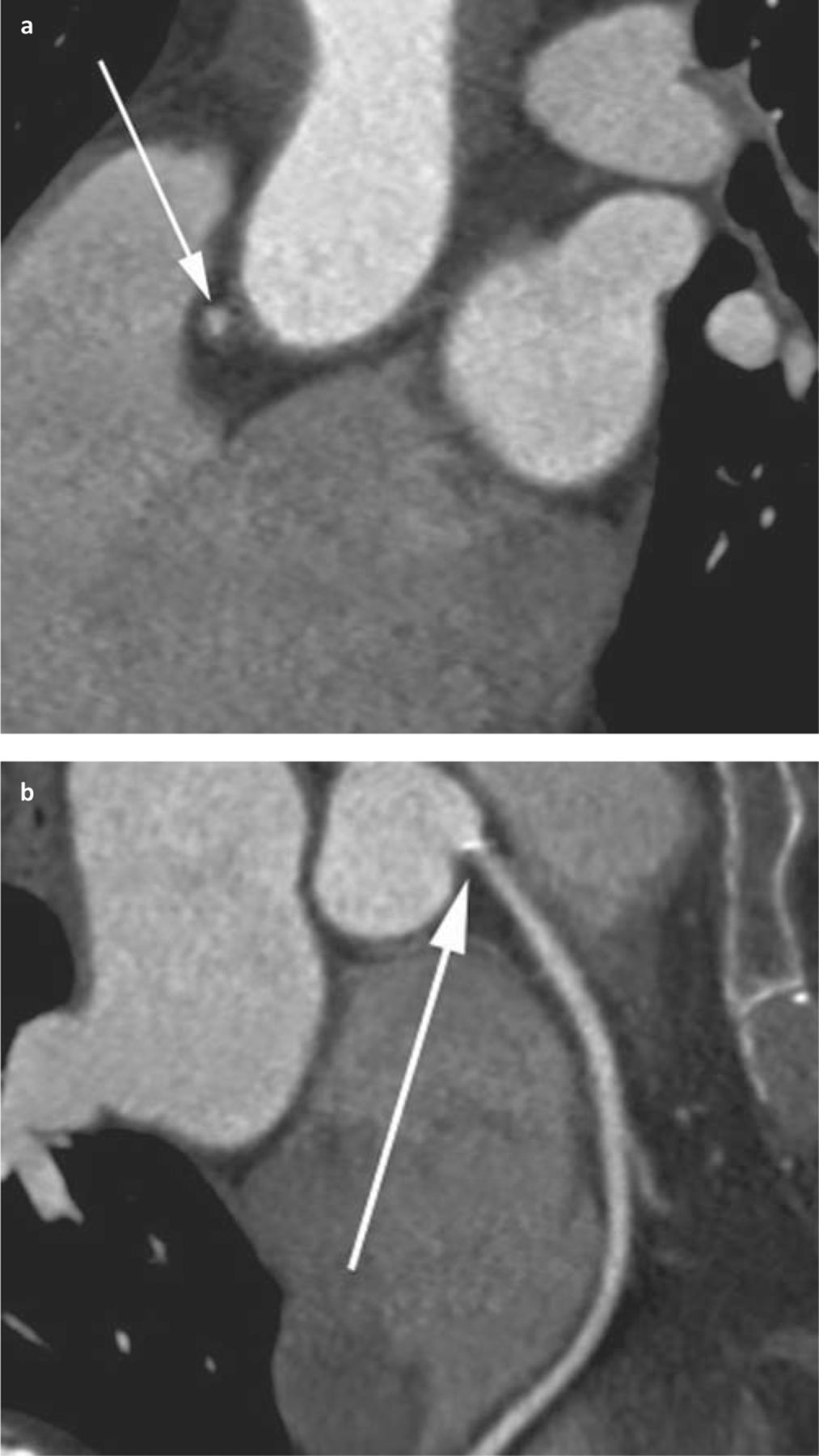
CTCA could also be used to diagnose and delineate congenital coronary anomalies,23 which may present with chest pain, or as a valuable problem-solving tool, for example after a failed catheter angiogram (eg due to dilated aortic root, suspected ostial coronary disease, coronary anomalies). Fig 6 illustrates how CTCA can be used in such a manner – a patient underwent ICA during which RCA ostial stenosis was suspected but proved difficult to delineate. CTCA accurately demonstrated the stenosis.

Axial (a) and multiplanar (b) reformat of CTCA demonstrate ostial RCA stenosis suspected but not delineated on ICA.
Conclusions
The NICE guidance defines the role of coronary CT in the diagnosis and assessment of patients with chest pain. This technique is not a substitute for thorough and accurate clinical assessment and requires adequate patient selection. It should be reserved for low- to intermediate-risk patients, predominantly to exclude significant CAD. We have illustrated the role that calcium scoring has in selecting patients who are suitable for CT coronary angiography. Encouraging short- to medium-term prognostic data now exist, but there is still a lack of long-term clinical outcome data for coronary CT. The best use of ECG-gated coronary CT in the emergency setting, and the relative cost-effectiveness of CT and the current standard of care in suspected CAD, is the subject of ongoing and future research. If used appropriately, coronary CT is a powerful and valuable clinical tool.
- © 2012 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}