
Abstract
Inflammatory arthritis involves a diverse range of conditions in which an uncontrolled immune response occurs. A number of advances in assessment, diagnosis and treatment have been made in recent years. Drug therapies used in inflammatory arthritis aim to reduce symptoms and suppress inflammation, joint damage and disability. In rheumatoid arthritis (RA), immunosuppression is used in almost all patients, with an emphasis on early aggressive treatment to achieve clinical remission. This approach is less successful in spondylarthropathies, for which non-steroidal anti-inflammatory drugs remain first-line therapy. The use of biologic therapies has increased dramatically across a range of indications and has resulted in improved outcomes for patients. These agents are associated with an increased risk of infection, particularly tuberculosis in patients receiving tumour necrosis factor inhibitors. Alternative biologics have entered clinical practice for RA in recent years, and clinical trials using these agents, as well as novel non-biologic therapies, are in progress for RA and other conditions.
- inflammatory arthritis
- rheumatoid arthritis
- psoriatic arthritis
- ankylosing spondylitis
- drug therapy
- DMARDs
- biologics
Background
Inflammatory arthritis spans a diverse group of conditions. They are characterised by uncontrolled immune responses that result in inflammation of joints and surrounding structures. Some patients have extra-articular features and systemic inflammation. Inflammatory arthritis spans rheumatoid arthritis (RA), the seronegative spondylarthropathies – ankylosing spondylitis (AS) and psoriatic arthritis (PsA) – and some less frequent conditions (Table 1). Gout, pseudogout, inflammatory osteoarthritis, childhood arthritis and infective arthritis are considered separately, although they all involve joint inflammation.
Conditions causing inflammatory arthritis and common clinical features.
Recent advances in assessment and diagnosis
Rapid diagnosis and early therapy are essential, particularly in RA, where a ‘window of opportunity’ exists. Early treatment, ideally within three months of symptom onset, gives marked improvements in long-term outcome. Delay in diagnosis is a common problem, with major delays prior to presentation in primary care. Data from early arthritis clinics have driven prediction models for persistent arthritis and helped improve classification criteria in RA.1 Screening questions and criteria have also been developed for early PsA and AS.
High-resolution ultrasound and magnetic resonance imaging (MRI) are increasingly used in the diagnosis or assessment of patients with inflammatory arthritis. Both are highly sensitive for detecting synovitis and tenosynovitis, even in the absence of clinical signs, and are more sensitive than X-ray in detecting erosions.2 Power Doppler ultrasound (PDUS) images blood flow within small synovial vessels and is a surrogate of angiogenesis, a key pathological process in RA. It can improve prediction of RA in patients with early arthritis. Data are also promising for short-term monitoring of disease activity following therapeutic intervention (reviewed in Ref 3). Many units now use ultrasound as a routine diagnostic and prognostic assessment tool in inflammatory arthritis.
X-rays are often normal in early spondylarthropathy, but MRI is highly sensitive in detecting active inflammation in the spine and sacroiliac joints to aid diagnosis at an early stage. These inflammatory changes can also be used to predict response to biologics (reviewed in Ref 4).
The introduction of tests for anti-citrullinated protein antibodies (ACPAs) has proved to be a major advance in the diagnosis of RA. It has high sensitivity and specificity compared to rheumatoid factor. Evidence is growing that ACPA-positive disease should be considered as a distinct subset, with separate genetic risk factors and disease course (reviewed in Ref 5), including differential responses to therapy.
Overview of drug therapies
Drug therapies used in inflammatory arthritis aim to reduce symptoms and suppress inflammation and its consequences (joint damage and disability). Therapy options are dependent on clinical features: immunosuppression is less effective for spinal disease, and the extent of other comorbidities such as psoriasis and inflammatory bowel disease should be considered. Although drug treatment is important, non-drug therapies, which span advice, exercise, physiotherapy and surgery, all form crucial additional components of disease management.
Controlling symptoms of inflammatory arthritis
Conventional disease-modifying antirheumatic drugs (DMARDs), corticosteroids and biologics have central roles in controlling symptoms in arthritis. However, non-steroidal anti-inflammatory drugs (NSAIDs) and analgesics are used with these agents, with the specific intention of reducing joint pain and swelling.
Non-steroidal anti-inflammatory drugs
Non-steroidal anti-inflammatory drugs reduce signs and symptoms of inflammation without having any disease-modifying effects. In spondylarthropathies, NSAIDs are first-line therapy for patients with pure axial disease or minimal peripheral joint involvement. They improve spinal and peripheral joint pain and function, with cyclooxygenase 2 (COX-2) inhibitors being equally effective for spinal pain. Individual variation in response is observed, so successive NSAIDs or COX-2 inhibitors may be required: there is no clear evidence that a single NSAID is superior (reviewed in Ref 6). NSAIDs are often used long term, so the risk of gastrointestinal bleeding and cardiovascular toxicity should be considered.
Analgesics
The evidence base for analgesics in inflammatory arthritis remains poor, with multiple small, poor-quality studies. Some evidence suggests that weak opioids are effective in RA up to six weeks, but adverse events are common.7 Despite common use of neuromodulators and antidepressants in musculoskeletal pain, results in patients with RA are conflicting. Nefopam and oromucosal cannabis reduce pain compared with placebo, but are associated with frequent adverse events. Capsaicin reduces pain; although local burning is common, this leads to withdrawal in only 2% of patients.8 No evidence shows a benefit from antidepressants for pain or depression up to one week, and evidence of benefit in the medium term (up to six weeks) is conflicting.9 Many patients use combination analgesics, but these approaches have not been assessed in patients receiving DMARDs.10 Further studies in this area clearly are needed.
Long-term suppression of inflammation
Disease-modifying antirheumatic drugs
Disease-modifying antirheumatic drugs reduce symptoms and systemic inflammatory responses and limit progression of joint damage. The most commonly used DMARD is methotrexate, either as monotherapy or in combination with other DMARDs or biologic therapies. Sulfasalazine and leflunomide are also used and have similar efficacy to low-dose methotrexate. Intramuscular gold, hydroxychloroquine, ciclosporin, minocycline, azathioprine and tacrolimus are also disease modifying but are used less commonly due to reduced efficacy and increased toxicity compared with methotrexate.11
Combination DMARDs are recommended early in the disease course in RA, preferably within three months of the onset of symptoms,12 to take advantage of the ‘window of opportunity’ for early control of disease. Use of DMARDs with either steroids or biologics is effective in early disease, although combinations of conventional DMARDs and steroids are more cost effective than early biologics. Various DMARD combinations are used in clinical practice, commonly ‘triple therapy’ (methotrexate, sulfasalazine and hydroxychloroquine) or dual therapy combinations, with only small increases in toxicity.13
In spondylarthropathies, there is less support for DMARDs for spinal symptoms and they are not recommended in the absence of peripheral arthritis. Methotrexate has been used to treat psoriasis for many years and some evidence supports its use in peripheral arthritis. In a recent study, methotrexate did not significantly improve arthritis compared with placebo and may not be truly disease modifying in PsA at doses up to 15 mg/week.14 However, higher doses are used in clinical practice and methotrexate remains part of international guidelines. Sulfasalazine produces significant benefits for both peripheral arthritis and axial disease. Ciclosporin has been used successfully to treat psoriasis and is also effective for peripheral arthritis. Its use is limited by toxicity and frequent withdrawal due to adverse events. Leflunomide (20 mg/day) is clinically effective for both peripheral arthritis and psoriasis, with response rates of 59% versus 30% for placebo. Improvements are also seen in function and quality of life.15
Studies in patients with AS suggest a small effect of sulfasalazine on spinal stiffness and erythrocyte sedimentation rate (ESR), with possibly greater effects in those with early disease or peripheral arthritis; it may also prevent anterior uveitis.16
Corticosteroids
Corticosteroids have been used to treat RA for more than 60 years. In the short term, steroids reduce synovitis and improve signs and symptoms of arthritis. They reduce progression of joint damage in early RA17 and are recommended in combination with DMARDs in early disease.12 In established disease, benefits are less clear cut and evidence indicates that disease modification is reduced.18 However, steroids are recommended for short-term use during flares, as bridging therapy while DMARDs are adjusted and by intra-articular injection into active joints. The timing of steroid dosing may influence symptom relief: modified-release prednisolone given at night is associated with less morning stiffness than immediate-release prednisolone, with a comparable safety profile.19
Systemic corticosteroids are used less frequently in PsA due to the risk of flares of skin disease (particularly pustular psoriasis) on withdrawal. Corticosteroids are not recommended for long-term therapy in AS or PsA, but intra-articular injections may be helpful and are a good approach in patients with mono- or oligoarticular peripheral arthritis.
Biologic therapies
Biologic therapies have revolutionised modern rheumatology practice. Tumour necrosis factor (TNF) inhibitors were the first biologic agents to enter routine use for treatment of RA. Although expensive, they are highly effective, particularly in combination with methotrexate,20 with profound effects on symptoms and radiographic progression. Similarly, TNF inhibitors control signs and symptoms of PsA, including dactylitis, enthesitis, skin and nail disease, with a significant impact on radiographic progression.21 TNF inhibitors also reduce and have effects on skin and nail disease. In AS, patients experience significant benefit at any stage of disease, although the benefit seems to be greatest in early disease. Spinal inflammation assessed by MRI improves substantially, but there is no benefit for radiographic progression. No evidence indicates that different TNF inhibitors have differential effects on enthesitis or uveitis, although monoclonal antibodies (rather than receptor fusion proteins) are recommended for patients with symptomatic inflammatory bowel disease.
In the UK, biologic use is restricted to patients with severe uncontrolled disease who have failed therapy with at least two DMARDs (or NSAIDs in the case of AS) and patients must show clear evidence of response (Table 2 and references 12, 22 and 23).
Safety
Drug therapies give a range of adverse events spanning steroid-induced osteoporosis, NSAID-related gut inflammation and infection. Assessment of the relationships is complex, as some adverse events (for example, infection) may also be due to the underlying arthritis.
Osteoporosis and osteopenia occur due to cytokine-induced osteoclast activation and osteoblast inhibition leading to net bone resorption.24 Patients who receive long-term corticosteroids are also at risk of fragility factures and often require treatment with bisphosphonates or other therapies for osteoporosis.
Use of NSAIDs poses significant risks for oseophagitis and peptic ulceration. However, hospital admissions related to ulcers have declined as a result of preventive measures, such as coprescribing proton pump inhibitors (PPIs).25 Although PPIs reduce bleeding from the upper gastrointestinal tract, NSAIDs are also implicated in damage to the large and small bowel, which causes bleeding, weight loss, perforation and bowel obstruction;26 PPIs do not prevent ulceration in these areas. NSAIDs may also exacerbate pre-existing inflammatory bowel disease in spondyloarthropathies.
DMARDs and NSAIDs have been implicated in liver damage. Frequent blood monitoring is recommended for patients receiving methotrexate, leflunomide, azathioprine and sulfasalazine, and NSAIDs are a common cause of drug-associated liver failure.27
Rheumatoid arthritis is itself a risk factor for hospital admission due to infection, and oral steroids and biologics are associated with an increased risk of hospitalisation, as well as an increased risk of mild infections.28 Cyclophosphamide and azathioprine are also associated with an increased risk of admission with infection.29 Biologic therapies are associated with more severe infections, particularly pneumonia and soft-tissue infections.30,31 Reactivation of latent tuberculosis is particularly associated with TNF inhibitors, with the highest risks reported for adalimumab and infliximab,32 so screening followed by targeted chemoprophylaxis is recommended.33
DMARDs have been linked with malignancy, particularly cyclophosphamide and chlorambucil, which are now used rarely.34 Large case–control studies do not suggest an increased risk of malignancy with methotrexate,35 but there are reported associations between TNF inhibitors and skin cancer and lymphoma.36
Recent innovations in drug treatment
Several major advances in the treatment of inflammatory arthritis have been made in the last decade. Outcomes in early RA have improved with intensive early combination DMARD therapies. The ‘biologics revolution’ has also continued: several non-TNF biologics have reached the clinic and research to develop novel non-biologic DMARDs continues.
Early intensive treatment and tight control of disease activity
Recent studies have shown the benefit of tight control of disease activity in RA (aiming for remission or low disease activity, Fig 1).37 A number of trials have evaluated treatment strategies rather than fixed drug regimens and have shown improved effectiveness with step-up DMARD monotherapy compared with standard care. Studies in early disease have often used combination DMARDs and high doses of steroids or early biologic therapies initially, and then stepped down treatment once remission or low disease activity has been achieved (reviewed in Ref 38). These strategies require frequent follow-up visits until disease is controlled but result in a rapid reduction of inflammation, reduced joint damage progression and improved functional outcomes. These benefits are maintained long after the initial period of intensive therapy.39 Use of such goal-directed strategies is feasible in routine practice in patients with early40 and established41 disease, but efficacy with these strategies requires both the treating physician and the patient to alter therapy if the selected target is not reached. These approaches are now being studied in early PsA.42
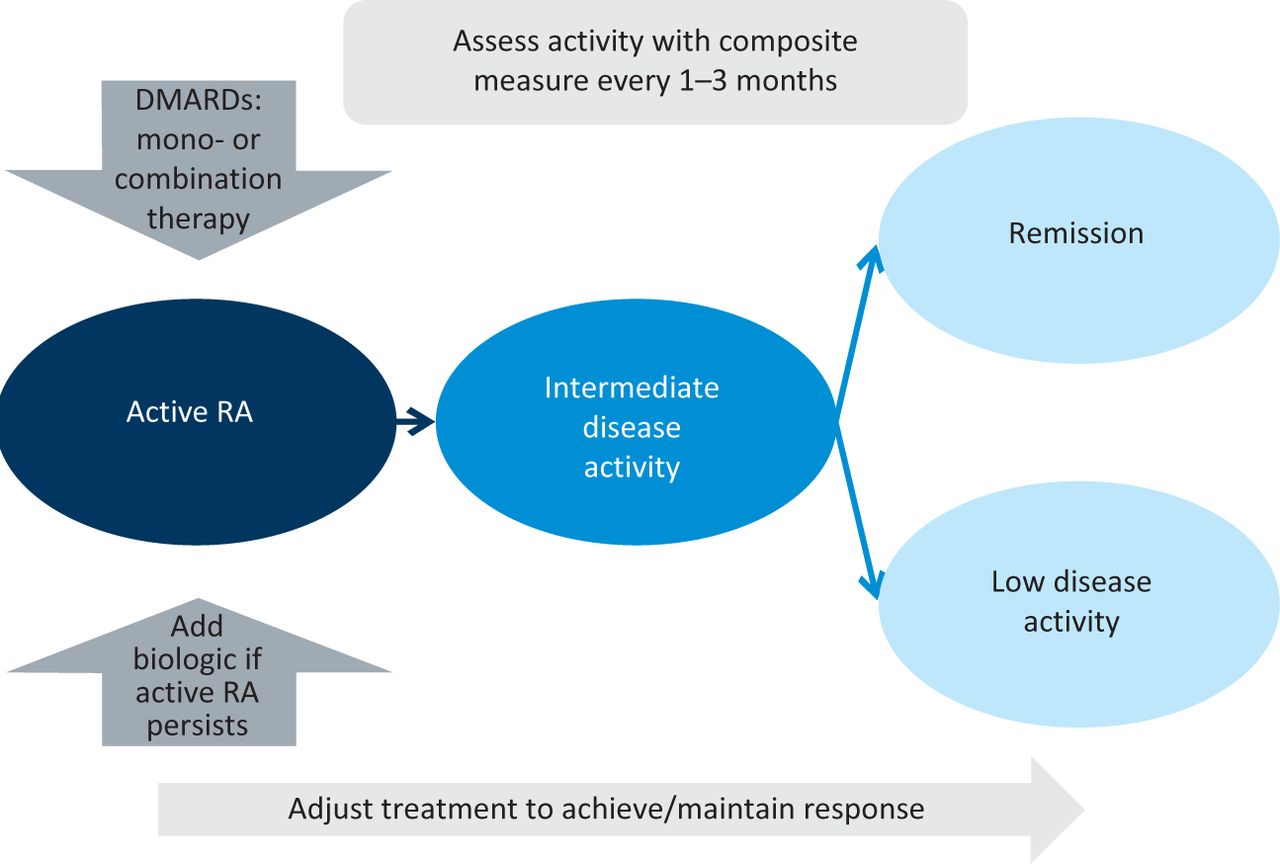
Treating to target in rheumatoid arthritis (RA). A defined treatment aim should be selected: preferably clinical remission, or low disease activity in patients with long-term disease. Patients with active disease should be reviewed frequently and disease activity should be assessed using a composite disease activity score. Therapy should be escalated if disease remains active. DMARD, disease-modifying antirheumatic drug. Adapted from Smolen et al.37
New biologics
Biologics with alternative modes of action have entered clinical use for patients with RA and inadequate responses to TNF inhibition, including rituximab (B-cell depletion), tocilizumab (interleukin 6 (IL-6)-receptor inhibition)43 and abatacept (inhibition of T cell costimulation).20
Alternative biologics have also been used in clinical trials in PsA (reviewed in Ref 44). Efalizumab, which inhibits T-cell trafficking, was effective for psoriasis but did not improve joint symptoms and it was withdrawn after reports of an increased risk of progressive multifocal leukoencephalopathy. Alefacept, an alternative inhibitor of T-cell costimulation, reduces tender and swollen joint counts, and responses were also seen with abatacept. Recent data with ustekinumab, which blocks the action of interleukins 12 and 23, have shown excellent responses in skin disease and encouraging improvements in arthritis. Clinical trials of interleukin 17 inhibitors are in progress in RA, PsA and AS.45
No evidence currently supports efficacy of other biologics in AS. An open-label study of abatacept did not show evidence of major response,46 and rituximab was ineffective in patients who had failed to respond to TNF inhibitors, but clinically significant responses were seen in TNF inhibitor-naïve patients.47
Novel agents: small-molecule compounds
A number of orally administered small molecules (molecular weight <1 kDa) that inhibit signalling molecules involved in the inflammatory cascade are now available. Most of these compounds block kinases, eg mitogen-activated protein kinases (MAPKs), spleen tyrosine kinase (Syk) and janus kinases (JAKs).
The p38 MAPK regulates production of proinflammatory cytokines and a number of p38 inhibitors have entered clinical trials in RA. Convincing clinical responses were not seen, possibly due to dose-limiting toxicity or redundancy within signalling pathways. Inhibition of JAK and Syk seems more successful. Syk is involved in signalling through receptors on multiple immune cells. Fostamatinib is metabolised to R406, a potent Syk inhibitor, and significant clinical benefit was seen in patients with RA who had failed to respond to methotrexate. Results in non-responders to biologics were less favourable. Tofacitinib is a potent inhibitor of JAK. Clinical trials in RA have shown encouraging responses, although adverse events including anaemia, diarrhoea and infection were observed (reviewed in Ref 48). These small-molecule compounds are cheaper to manufacture than biologic drugs, but the ideal place of these agents in clinical practice and clear evidence of an effect on joint damage progression have yet to be established.
Conclusion
Drug therapy in inflammatory arthritis aims to control disease activity and prevent joint damage or loss of function. Many treatment options now exist, spanning conventional DMARDs and biologic therapies for patients with persistently active disease. Biologics have dramatically changed outcomes for patients with refractory disease and their use is increasing. Intensive strategies aimed at remission, involving combinations of DMARDs with steroids or biologics, have radically improved long-term outcomes, particularly in patients with early disease. Ongoing research is determining optimal strategies in early and established RA and evaluating the role of intensive approaches in other forms of inflammatory arthritis. Interest in new non-biologic treatments is intense and a number may soon enter clinical practice.
- © 2012 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.