
- nuclear medicine
- dementia
- Parkinsonian syndromes
- primary brain tumours
- plaque imaging
- FDG
- FP-CIT
- ioflupane
- MIBI
Key Points
The role of functional imaging with nuclear medicine techniques in neurology is well established and continues to expand rapidly
18Fluorodeoxyglucose (FDG) is a defining biomarker in clinical dementia
Magnetic resonance imaging (MRI) assessment of regional atrophy and cerebrospinal fluid oligomer amyloid measurement are also potential biomarkers for Alzheimer's disease, but the clinical breadth of FDG in many types of dementia increases its clinical usefulness
123I-Ioflupane is well established for the diagnosis of early idiopathic Parkinson's disease and is of value in assessing dementia with Lewy body
In the difficult differentiation of recurrent primary brain tumour from benign radionecrosis, functional nuclear medicine imaging improves decision making and clinical management
If the 20th century was the century of the development of structural imaging of disease, the 21st has the potential to be that of functional imaging. Significant advances in technology now allow structural and functional data to be combined to define and subclassify clinical disease, and thus guide management.
Structural imaging is widely used to assess both tumour development and brain atrophy. Abnormalities are often seen in the final stages of disease when the clinical importance of these changes in terms of influencing outcome may be low. Functional changes occur much earlier in disease processes and, if detected, may have a greater impact on clinical care.
Most types of functional nuclear medicine brain imaging involve the use of picomolar amounts of radiopharmaceutical to image changes in receptor expression and other uptake mechanisms in the normal brain. Pathological overexpression of receptor density or loss of normality in uptake pathways reflects changes in the blood-brain barrier (BBB), glial cells and neurones. Imaging these changes at an early stage has the potential for improved diagnosis and can inform management decision making.
This review concentrates on common clinical problems for which nuclear medicine is clinically useful in routine practice. The field is advancing rapidly and future applications of new tracers will also be discussed briefly.
Dementias
Dementias are a group of diseases given a complex definition in the International Classification of Disease, 10th Edition (ICD10), highlighting the challenges faced by clinicians who investigate and manage neurodegenerative disease:
… syndromes due to disease of the brain, usually of a chronic and progressive nature, in which there is impairment of higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning capacity, language and judgment. The cognitive impairments are commonly accompanied and occasionally preceded by deterioration in emotional control, social behaviour or motivation.
Functional nuclear medicine techniques are increasingly used to diagnose dementia, the incidence of which is increasing. In the UK, over 800,000 people live with the diagnosis, imposing an economic burden of over £23 billion over and above the human cost.1
The ‘despair diagnosis’ often associated with dementia should be addressed – to the extent that the value of early diagnosis has been questioned in the absence of curative treatment. By contrast, the 2005 Department of Health strategy document, Living well with dementia2 stated:
Research shows that early intervention in cases of dementia is cost effective and can improve the quality of life for people with dementia and their families.
Preliminary data presented at the Alzheimer's Association International Conference on Alzheimer's Disease (ICAD) in 2010 (Dementia Demonstration Project) show that prompt diagnosis of dementia saves money, even early in the course of disease.3 Most agencies now advocate early diagnosis as an important factor in the successful management of dementia.
Clinical presentation
Clinical presentation is highly variable and complex. First results from the Rush Memory and Aging Project4 show that ‘…correlation of the clinical definition of disease and pathology is poor’. There is therefore a compelling role for biomarkers to guide diagnosis and management.
Diagnosis
(18F)-Fluoro-deoxyglucose PET/CT
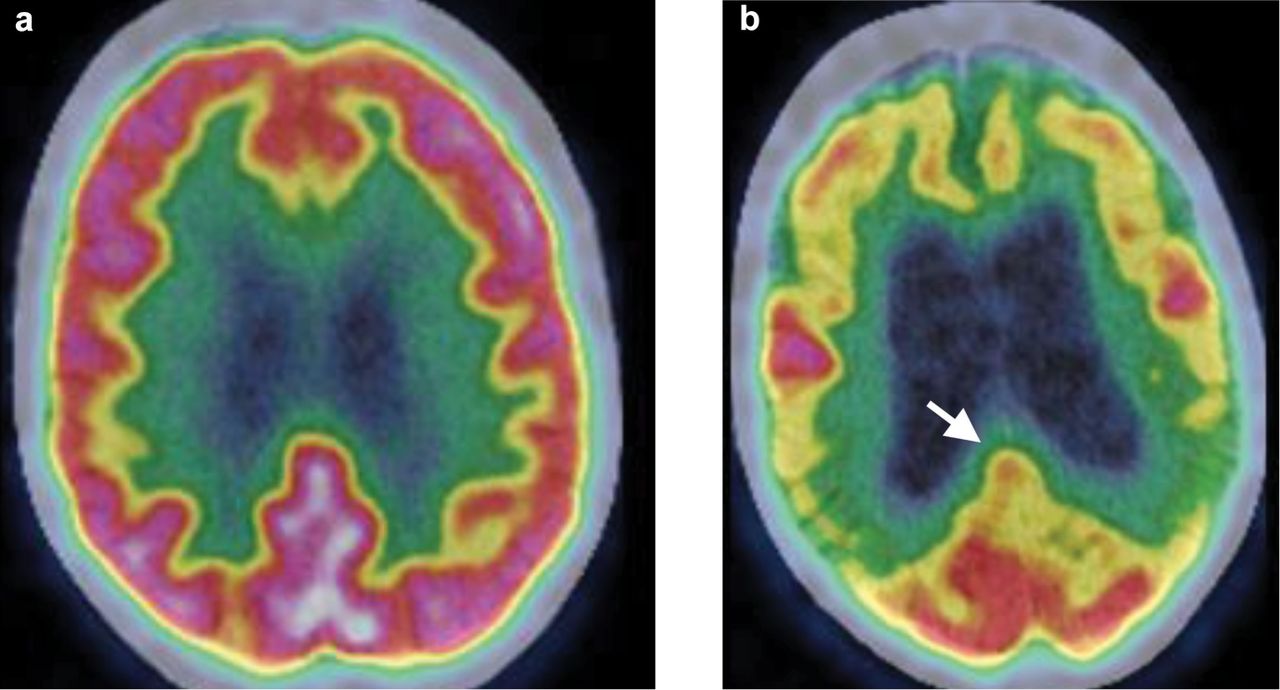
The most important radiopharmaceutical in the diagnosis of dementia is (18F)2′-fluoro-2′-deoxy-D-glucose (FDG). Its distribution is assessed using a combined PET/CT scanner (Fig 1). This technique images altered expression of glucose transporters (GLUT) in the BBB, glial cells and neurones. FDG has a major role in characterising ‘intrinsic neurodegenerative dementias’ such as:
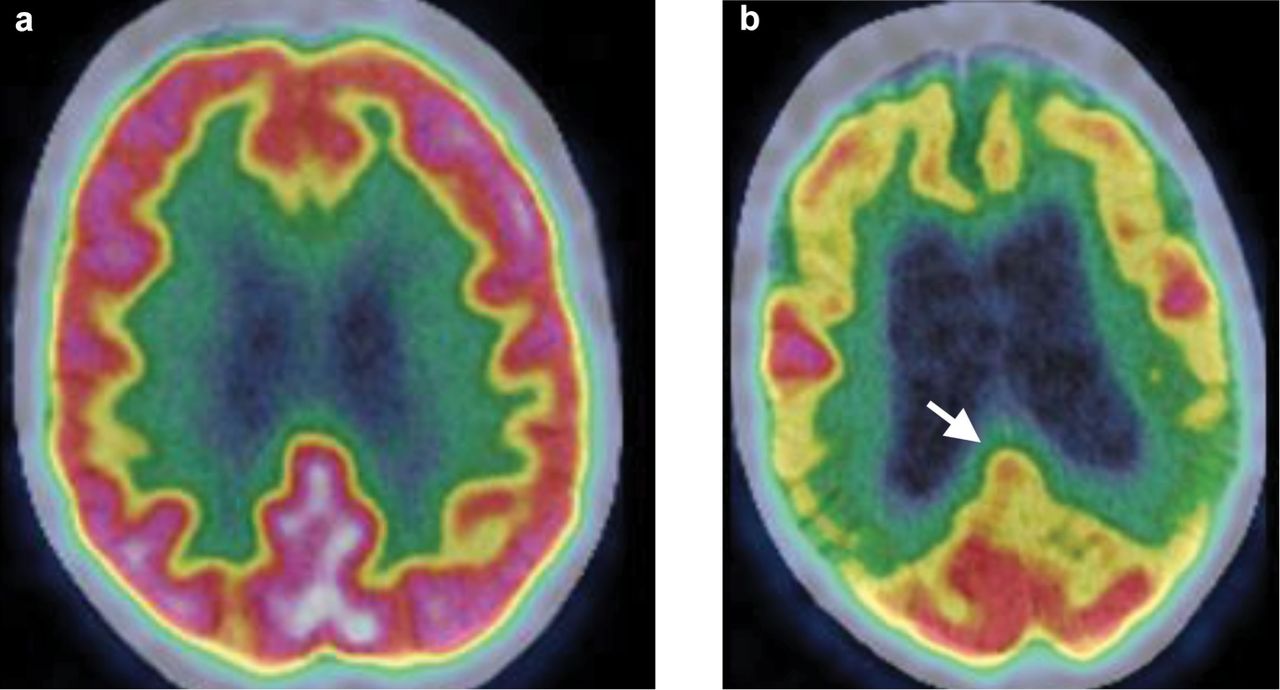
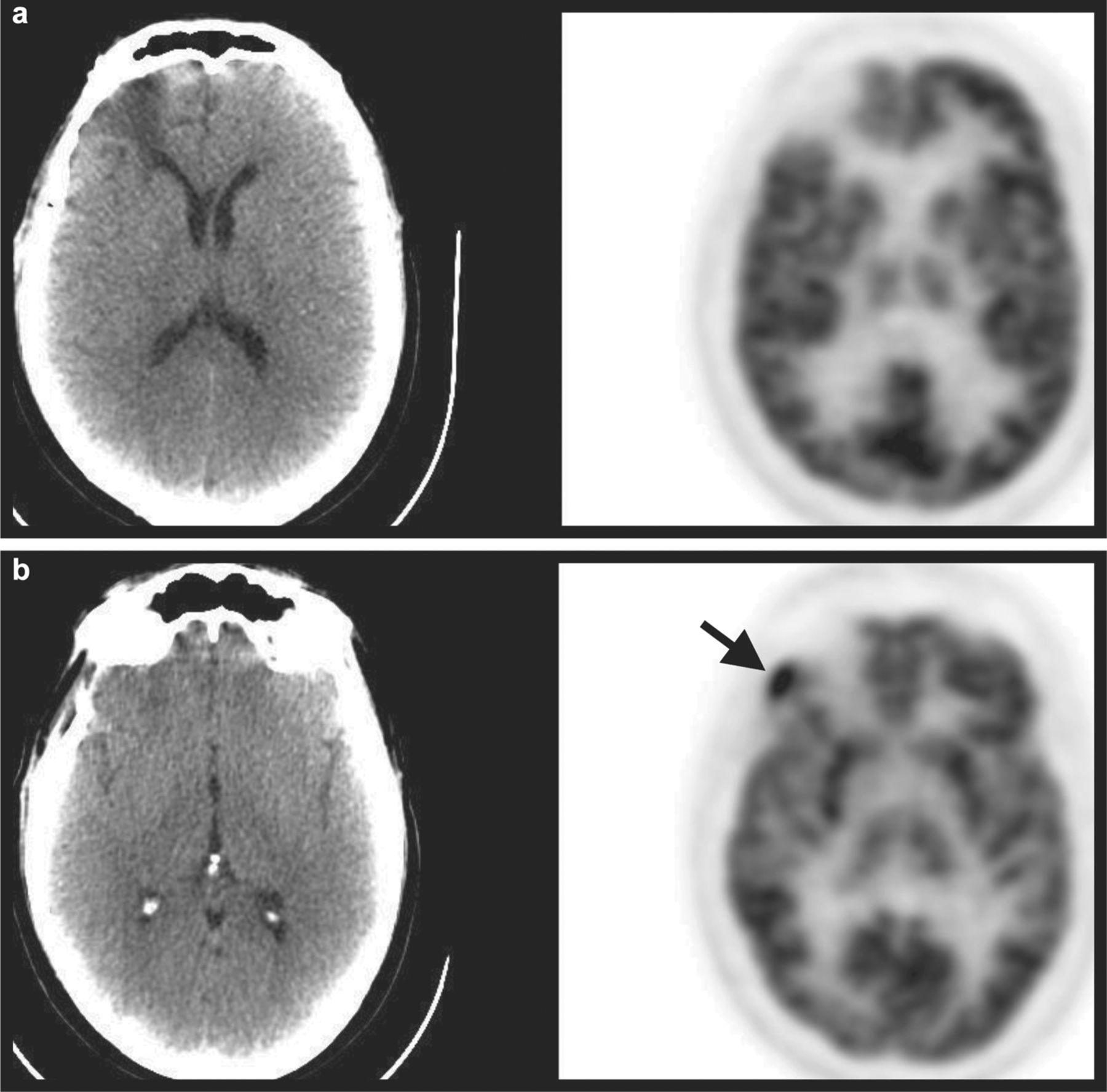
Axial images of FDG PET distribution in the brain at the level of the body of the lateral ventricles. Both patients presented with possible early dementia and MMSE scores of 28/30. (a) Normal comparative distribution of activity in the frontal and parietal lobes, with no significant loss of activity. (b) Clear evidence of disease with severe loss of activity in both temporoparietal lobes and moderate activity in the frontal lobes. Between these regions, there is relative maintenance of activity in the sensorimotor cortex on both sides – a good clinical indicator of the presence of an intrinsic neurodegenerative dementia on the scan. Activity is also maintained in the occipital lobes. There is also loss of comparative activity in the posterior cingulate gyri (white arrow), a relatively specific regional sign for the presence of Alzheimer's disease.
Alzheimer's disease (AD)
dementia with Lewy Body (DLB) (previously Pick disease, but now a broader and more accurate disease spectrum of alpha-synucleinopathies) (Fig 2)
frontotemporal dementia (FTD) and its variants.
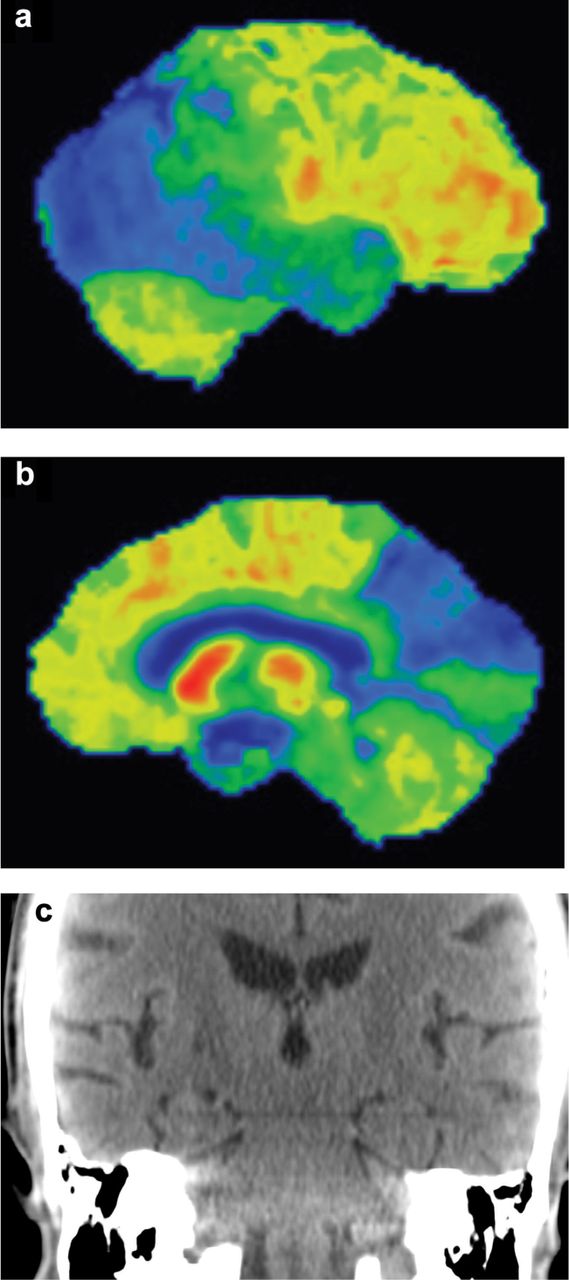
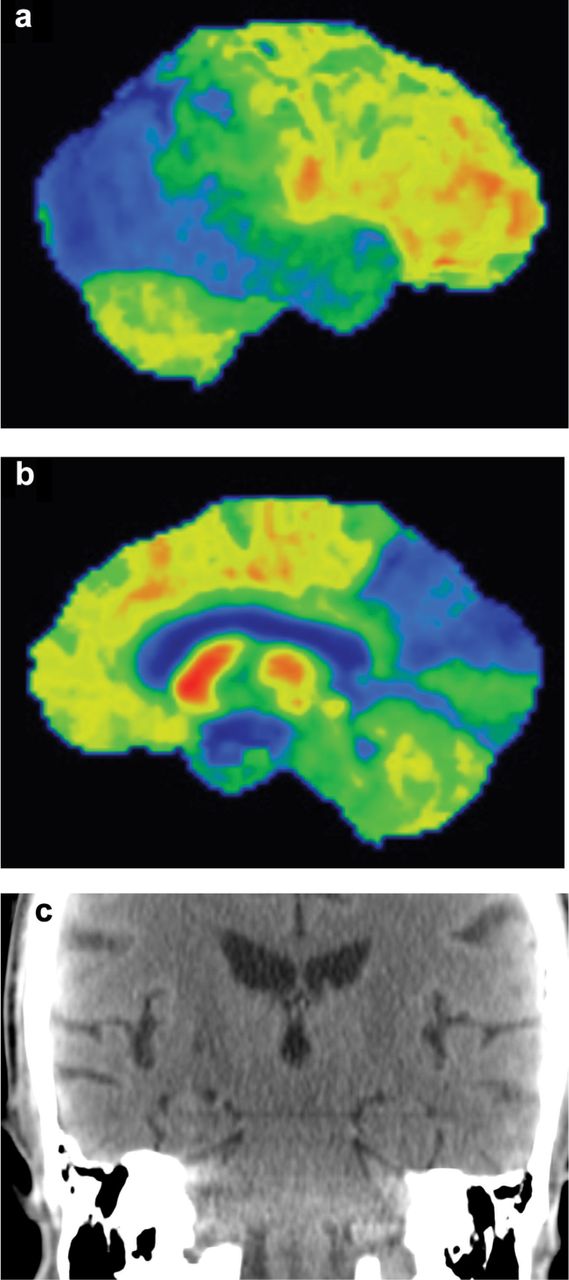
Image of the semi-automated assessment of FDG activity in the brain in which the observed activity is subtracted from a bank of age-matched controls, showing lateral (a) and medial (b) images of the right hemisphere. There is loss of activity in the temporoparietal right lateral lobe, with further loss in the occipital lobe. Changes in the occipital lobe are the most accurate discriminator of the presence of dementia with Lewy body (DLB). (c) With the development of multislice PET/CT scanners, coronal reconstructions of the brain allow assessment of the medial temporal lobe volumes, graded normal in this patient, adding further evidence to the diagnosis of DLB rather than Alzheimer's disease.
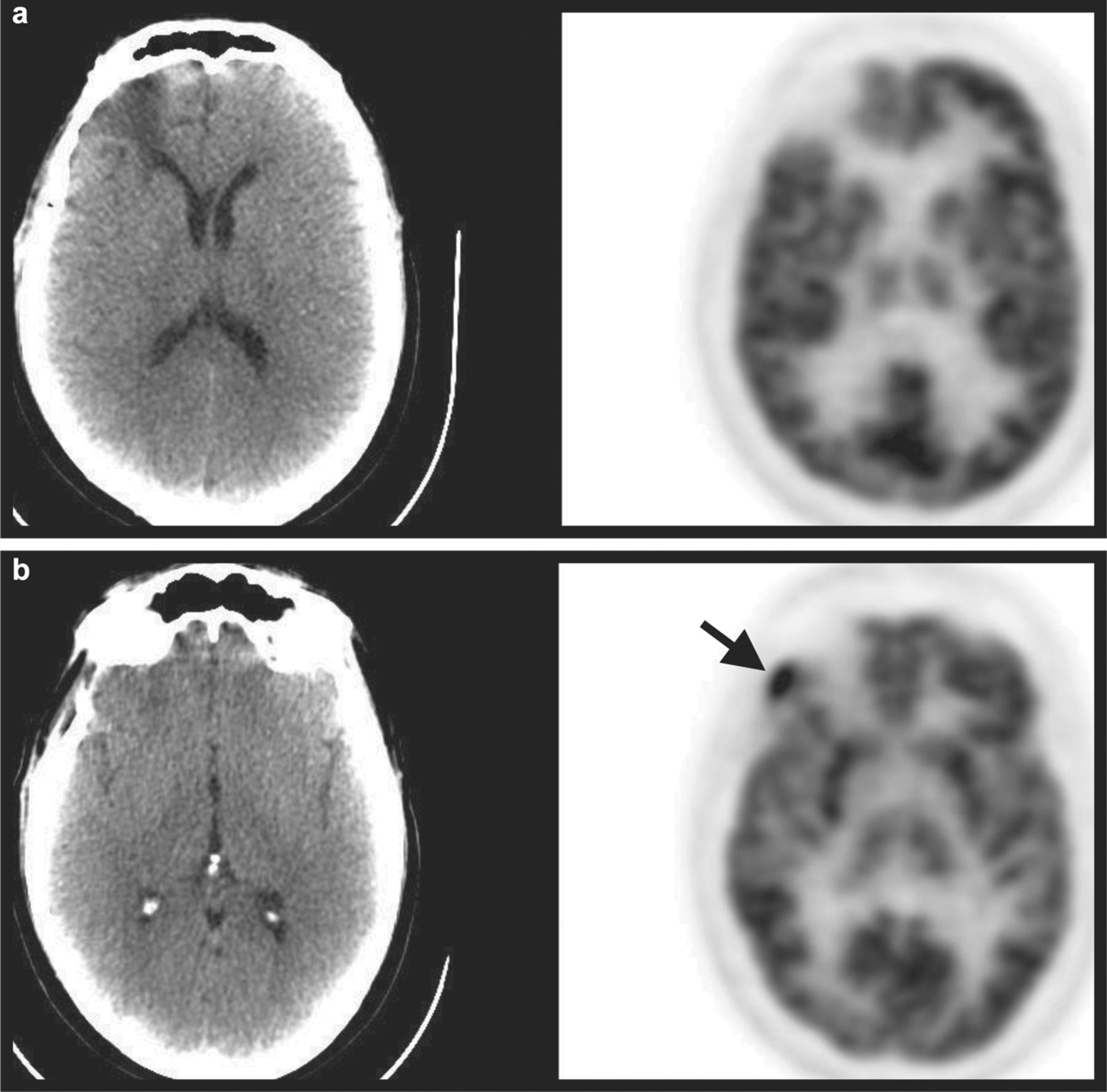
Two axial PET/CT images in a patient with a past history of high-grade oligodendroglioma of the right frontal lobe previously treated with chemoradiotherapy. An MRI had shown equivocal findings, with clinical suspicion of recurrent disease. (a) Low attenuation radionecrosis is seen with no abnormal FDG uptake in this area. (b) Abnormal FDG uptake is seen in the inferoposterior aspect of the previous treatment field (arrow), confirmed as recurrent disease on PET-guided biopsy.
Alzheimer's disease. In AD, the most common form of dementia, complex changes include decrease in GLUT1 and 3 on the BBB and neurones, respectively, and increased GLUT 3 on glial cells.5 These changes partly reflect the loss of excitatory glutamate synapses secondary to the neurotoxic processes associated with dementia. In AD, these neurotoxic effects derive from soluble amyloid protein from the cleavage of the amyloid precursor protein (APP).6
Other dementias. FDG also has the potential to identify early abnormalities in other forms of dementia. The Rush Memory and Aging Project4 demonstrated that most patients have mixed pathology which is likely to be increasingly recognised by the medical profession. FDG is of less value in defining vascular dementia7 and no role in the investigation of dementia arising as the result of genetically determined biochemical abnormalities, trauma, inflammatory, infective, toxic or metabolic causes. In clinical practice, FDG is rarely indicated for dementias associated with Huntington's disease, progressive supranuclear palsy, Parkinson's disease (PD)-related dementia, idiopathic thalamic degeneration or Fahr's disease.
FDG in clinical practice. A recent trial by Caroli et al8 compared automated assessments of FDG distribution in subjects with AD, mild cognitive impairment (MCI) and normal controls. The accuracy of the assessments, measured as area under the curve, in 650 subjects ranged from 0.774–0.983. This large number of assessments in an ongoing study suggests an important role for FDG in clinical practice.
A review of the literature by Bohnen et al9 shows that:
… the evidence for (18)F-FDG PET in assessment of dementia has increased with new studies that include autopsy confirmation, wide-diagnostic-spectrum recruitment in primary care settings, historical and prospective cohort studies, and multicenter data analyses.
Mosconi et al10 adopted a standardised automated analysis of FDG PET brain studies of 548patients. The study population was considered representative of the clinical situation in the memory clinic (110 normal, 114 MCI, 199 AD, 98 FTD, 27 DLB subjects). It was found that 95% of AD, 92% of DLB, 94% of FTD and 94% of normals were correctly classified.
In a retrospective study, Laforce et al11 demonstrated that FDG imaging led to a change in diagnosis in 29% of patients with suspected dementia, a reduction in unclear diagnosis from 39–16%, the clinical impact being greatest in unclear and atypical cases.
Plaque burden
Imaging of ‘plaque burden’ in AD is important because AD is partly defined by the presence of beta-amyloid plaques in the extracellular space and neurofibrillary tangles in the neurones. Their presence has recently been reconfirmed as a defining characteristic of the disease in a large review of cases with pathological confirmation.12 The study also confirmed that, although beta-amyloid plaques may play a key role in AD pathogenesis, the severity of cognitive impairment correlates best with the burden of neocortical neurofibrillary tangles.
In 25–45% of autopsy brain examinations from cognitively normal elderly people the plaque deposition is indistinguishable from AD, indicating that neuronal loss, synaptic loss and atrophy are all required for the development of neuropsychopathology.13,14
There is considerable research interest in the development of plaque imaging agents such as 11C-Pittsburgh compound B (11C-PIB), 18F-flutametamol and 18F-florbetabir. These agents are being used to define the presence of beta-amyloidosis of the brain (BAB). BAB is seen in AD and is a risk factor for its development, but is also observed in cognitively normal individuals. At present, understanding of the cascade of APP cleavage by various secretases, production of possible neurotoxic dimers, development of oligomers, fibrils, beta-pleated sheets and beta-amyloid plaques is limited.
It is likely that plaque imaging will play a role in the selection of ‘at risk’ patients for treatment, the leading target for therapy being beta-amyloid dimers.15 Other options may include gamma-secretase inhibitors, secretase modulators, prevention of oligomer formation, increased removal of plaque and intravenous immunoglobulin.16–18 It is not clear whether plaque burden would be expected to increase or decrease as a result of successful treatment.
Parkinsonian syndrome
The group of diseases known as the Parkinsonian syndrome includes idiopathic PD (IPD) and the Parkinsonian-plus syndromes (multisystem atrophy, progressive supranuclear palsy and corticobasilar degeneration). The pathology of IPD is defined by the presence of Lewy bodies which fall within the same spectrum of pathology observed in DLB.19 Loss of neuronal cells occurs in the substantia nigra in the brain stem (pathological stage 3–4). The substantia nigra neurones send vulnerable unmyelinated long axons into the basal ganglia to produce dopaminergic synapses where movement control is modulated by their action. Parkinsonian symptoms develop when approximately 60–70% of neuronal cells and their axons are lost.
Ioflupane ([123I]N-ω-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl) nortropane, or FP-CIT) is a radiopharmaceutical which targets presynaptic dopamine reuptake transporters in the brain, the highest density being found in the basal ganglia. A qualitative reduction in selective tracer uptake occurs in the presence of Parkinsonian syndromes and reflects the typical onset of clinical symptoms in stage 3–4 disease. In a recent review of the major multicentre ioflupane studies, an abnormal scan predicted the development of IPD at three years with an accuracy of 78–97%.20 The negative predictive value of a normal scan was 92–97%.
Ioflupane is now established as a useful study in the differentiation of essential tremor from IPD, a normal result indicating a low probability of IPD. There has been interest in using ioflupane in the differentiation of IPD from the Parkinsonian-plus syndromes, but this has proved challenging and is not considered routine clinical practice at present.21,22 It is also of value in assessing DLB.23
Primary brain tumours
A detailed summary of all the tracers developed for neuro-oncology lies beyond the scope of this review. The most clinically useful indication for nuclear medicine imaging at present is the investigation of suspected recurrence in high-grade primary brain tumours using FDG PET/CT.
The treatment of high-grade tumours involves chemoradiotherapy which induces radionecrosis in the region treated. The distinction of radionecrosis from recurrent tumour using magnetic resonance imaging (MRI) is challenging and unreliable. Higher accuracy has been shown using FDG PET/CT. In a retrospective study of 117 consecutive patients with non-diagnostic post-treatment MRI and CT examinations, the positive (PPV) and negative (NPV) predictive values of 18FDGPET for tumour recurrence were 96% and 55.6%, respectively. A negative scan was associated with significantly prolonged overall survival.24
MIBI
In an interesting study of 81 patients, 99mTc-methoxy-isobutylene-isonitrile (MIBI) was used to discriminate between radionecrosis and recurrent disease.25 This tracer is used routinely in all nuclear medicine departments, is easily available and imaged using a conventional gamma camera with tomographic capability (SPECT). The overall sensitivity, specificity and accuracy of the technique was 90%, 91.5% and 90.5%, respectively, with 91%, 100% and 95%, respectively, for detection of more difficult, low-grade tumour recurrence. In addition, MIBI proved useful in detecting anaplastic transformation of low-grade recurrent tumours.
Other PET tracers
Other PET tracers used to assess primary tumours include amino acid analogues which allow imaging of both high- and low-grade tumours. 18F-fluoro-ethyl-tyrosine was used in a study of 53 patients, of whom 43 had high-grade and 10 low-grade tumours.26 All recurrences were detected, with no false negative results and an accuracy of 100%.
18F-fluoro-dihydroxyphenylalanine (DOPA) also shows promise in the assessment of malignant glioma, particularly in patients with suspected recurrence. A prospective study of eight patients demonstrated an overall sensitivity and specificity of 98% and 86%, respectively, with PPV 95% and NPV 95%. The sensitivity of 18F-DOPA in low-grade tumours was superior to that of FDG.27
- © 2012 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.