
Key points
A normal stress myocardial perfusion scintigraphy (MPS) indicates the absence of functionally significant coronary artery disease (CAD)
Sensitivity and specificity values of MPS of at least 80–90% for angiographically significant CAD
MPS for the assessment of myocardial ischaemia and scarring is an integral part of clinical guidelines and appropriateness criteria in many clinical settings
A normal MPS indicates a 0.7% annual risk of infarction and cardiac death, similar to that of the general population. An abnormal MPS confers approximately a seven-fold increase in annual coronary events. The likelihood of an event increases with the extent and severity of the inducible perfusion abnormalities
Observational studies suggest that if more than 10% of the myocardium is ischaemic by MPS, clinical outcome is better with revascularisation than with medical therapy. The reverse is true if less than 10% is ischaemic
Positron emission tomography (PET) is an accurate standard for quantitative myocardial perfusion and viability
PET is the only modality for which randomised data exist demonstrating that patients with severe left ventricular dysfunction whose therapy is guided by fluoro-deoxyglucose/PET have better outcome than with standard care
Nuclear cardiology has grown significantly in recent years because of developments in imaging hardware, software and tracers. Alongside these technical developments, there has been an increasing appreciation of the role the functional information provided by nuclear techniques can play in clinical cardiology to the point of improving patient outcome. This brief review discusses the principles of nuclear cardiology and its clinical applications, emphasising the role of myocardial perfusion scintigraphy (MPS).
Instrumentation
Most nuclear cardiology studies are performed using a conventional gamma camera with a sodium iodide detector and single photon emission computed tomography (SPECT). A new generation of cameras is now available which use cadmium zinc telluride detectors and have higher sensitivity and resolution.1 There has also been increasing interest in cardiac positron emission tomography (PET). Both SPECT and PET cameras have been combined with computed X-ray tomography (CT), offering not only more accurate attenuation correction but also making possible evaluation of coronary calcification and coronary anatomy in the same sitting with myocardial perfusion.2
Techniques
Assessment of myocardial perfusion
Radiotracers. Three tracers for MPS are commercially available (Table 1):
Common radionuclides used in myocardial perfusion scintigraphy.
thallium-201
technetium-99m-MIBI, and
technetium-99m tetrofosmin.
For PET perfusion imaging, rubidium-82, which is produced by a generator, is the most commonly used tracer, but the shorter lived perfusion tracers such as oxygen-15 water and nitrogen-13 ammonia are used in centres that have an on-site cyclotron.
Stress tests (Table 2). The most commonly used technique is dynamic exercise. However, exercise may be difficult in those with limited mobility or may be contraindicated in patients with left ventricular (LV) outflow tract obstruction or left main stem coronary disease. Furthermore, certain conditions such as left bundle branch block (LBBB) and permanent pacing can be associated with stress-induced perfusion abnormalities at high heart rates in the absence of obstructive coronary artery disease (CAD).3 For such patients, pharmacological manipulation of myocardial perfusion and oxygen demand is a valuable technique and is the default method of stress for PET perfusion studies. Pharmacological stress is accomplished with adenosine or dipyridamole; dobutamine is used where vasodilators are contraindicated in patients with, for example, sinoatrial disease or persistent asthma.3
Summary of stress test protocols.
High-risk imaging variables.
To avoid the side effects of vasodilator stress, agonists with a high selectivity for the adenosine A2A receptors responsible for the coronary vasodilator effect of adenosine have been developed. The only one commercially available is regadenoson and this has been used increasingly in the UK since 2011.4
It is also possible to combine stress techniques, the commonest pairing being dynamic exercise up to 75 W with either adenosine or dipyridamole. This increases sensitivity for the detection of perfusion defects and their visibility and also reduces the vasodilator side effects.
Image interpretation. Myocardial perfusion – and hence tracer distribution – is uniform in normal myocardium (Fig 1). A defect indicates reduced perfusion in viable myocardium, reduced amount of viable myocardium or a combination of both. If a stress defect returns to normal in the resting images, this indicates the presence of an inducible perfusion abnormality. Areas of infarction show a defect in both stress and rest images and the depth of the defect indicates the amount of myocardial loss (Fig 2). Another important feature is that less marked LV dilatation in the resting stress images implies extensive inducible ischaemia and is associated with an adverse prognosis.

Normal myocardial perfusion scintigraphy using thallium-201 with three selected short axis slices and central horizontal and vertical long axis slices after stress (left) and rest (centre). All parts of the left ventricular (LV) myocardium having high tracer uptake are shown in orange and white. The polar plots (right) show all parts of the LV myocardium in a single circular image. These can be compared with normal databases to assess the depth and extent of abnormalities and the overall ischaemic burden.
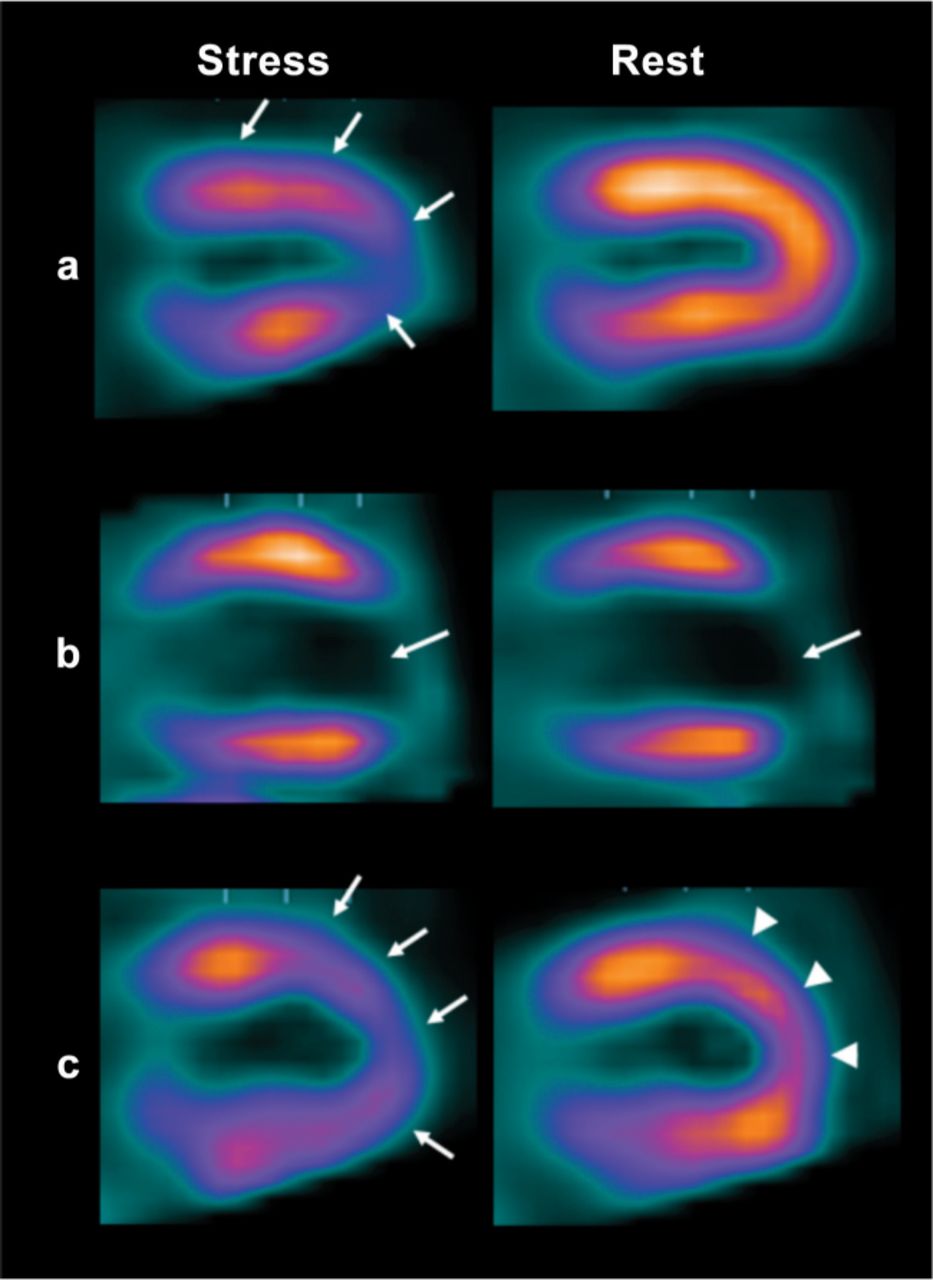
Patterns of myocardial perfusion shown from central vertical long axis slices. (a) Inducible perfusion abnormality without myocardial scarring. There is reduced tracer uptake on stress imaging (arrows), severe at the apex and mild in the anterior wall, which returns to normal at rest. (b) Myocardial infarction. Uptake is absent at the apex on stress images, remaining unchanged on rest imaging (arrows). (c) Partial thickness myocardial infarction with superimposed inducible ischaemia. There is moderate reduction of tracer uptake in the apex and apical anterior and inferior walls (arrows) on stress imaging. Images acquired at rest show improvement in these areas, but the anterior wall and apex fail to return to normal, indicating partial thickness myocardial damage (arrowheads).
Other nuclear cardiology techniques
In previous decades, assessment of LV function was commonly performed by equilibrium radionuclide ventriculography (RNV) using technetium-99m labelled erythrocytes.5 For biventricular functional assessment, a first-pass technique based on the first passage of the tracer through the central circulation is well validated.5 Both techniques have now largely been replaced by either ECG-gated SPECT of the perfusion images or echocardiography. However, SPECT blood pool imaging has some advantages, including the assessment of inter- and intraventricular synchrony from the phase image. RNV is now most commonly used for monitoring LV function in patients receiving potentially cardiotoxic chemotherapy such as doxorubicin and trastuzumab.5
An emerging tool for clinical studies is a norepinephrine analogue, iodine-123 metaiodobenzylguanidine (mIBG), which allows imaging of sympathetic myocardial innervation and provides prognostic information in patients with heart failure independently of other risk predictors such as LV ejection fraction and brain natriuretic peptide.6
Assessment of myocardial metabolism in combination with myocardial perfusion is a relatively common examination in heart failure patients for identification of myocardial hibernation. Glucose metabolism is most easily imaged using 2-fluoro-deoxyglucose (FDG) labelled with fluorine-18.7
Clinical applications
Myocardial perfusion scintigraphy
The National Institute for Health and Clinical Excellence recommends imaging of coronary function using, among other procedures, MPS in patients with a pretest likelihood of disease of 30–60%. When CAD is already known to be present, MPS may be considered in symptomatic patients and coronary angiography should follow if significant ischaemia is present.8 All guidelines emphasise the accuracy of vasodilator stress with MPS in patients with LBBB, paced rhythm, resting ST-segment depression greater than 1 mm or pre-excitation. Normal stress MPS indicates the absence of functionally significant CAD. A recent meta-analysis showed sensitivity and specificity of 85–90% and 70–75%, respectively, for the detection of angiographically significant CAD.9 In practice, specificity is higher than this level because some of the studies suffer from post-test referral bias.
Prognosis. Numerous studies have confirmed the excellent prognostic power of MPS, its important role in risk stratification and patient management, as well as its cost-effectiveness. A normal scan is associated with an annual risk of infarction and cardiac death of 0.7%, similar to that of the general population. An abnormal scan confers around a seven-fold increase in annual coronary events. The likelihood of an event increases with the extent and severity of the inducible perfusion abnormalities.10
Asymptomatic patients. For assessment of asymptomatic patients, international guidelines support MPS if there is a family history of premature CAD and in patients with diabetes and abnormal resting ECG or increased calcium score.11 MPS is also appropriate for assessment of asymptomatic patients undergoing elective intermediate to high risk non-cardiac-surgery.12
The acute setting. In the acute setting, the American Heart Association recommends MPS in patients with an intermediate likelihood of CAD presenting to the emergency room with chest pain in the absence of diagnostic ECG changes.13 Normal MPS excludes infarction, so stress testing may then safely be considered to rule out inducible ischaemia. Conversely, an abnormal result has a high sensitivity for obstructive CAD leading to an acute coronary syndrome (ACS), particularly when associated with a regional wall motion abnormality. In patients with ACS treated with coronary stenting, MPS is useful in the evaluation of the functional significance of non-culprit stenoses. After ST elevation myocardial infarction (STEMI), stable patients who have not undergone coronary angiography can be evaluated further by MPS within two to four days of infarction, contributing to risk stratification and further management plans. European and American guidelines also support the use of MPS for the detection of ischaemia in patients with non-STEMI who are not candidates for early intervention.14,15
Myocardial viability and hibernation. MPS has been used extensively in the evaluation of myocardial viability and hibernation. A large body of evidence supports current guidelines which recommend viability assessment in patients with dyspnoea and chronic ischaemic LV dysfunction.16 Uptake of more than 50% of maximum after tracer injection under nitrate cover is accepted as a marker of viability, with a minimum of four viable segments (approximately 25% of the left ventricle) needed to predict improvement of LV function after revascularisation. The most recent meta-analysis confirmed earlier data and showed that MPS is sensitive (83–87%) but less specific (54–65%) than techniques which challenge myocardial contractile reserve, such as dobutamine echocardiography and cardiac magnetic resonance (CMR), for predicting recovery of regional function after revascularisation (sensitivity 80% for dobutamine echocardiography vs 74% for CMR; specificity 78% for dobutamine echocardiography vs 82% for CMR).17 For contrast-enhanced CMR, these values are 84% and 63%.
The usefulness of MPS in this setting has been challenged recently by the substudy of the Surgical Treatment for Ischaemic Heart Failure (STICH) trial.18 The presence of viable myocardium was associated with an increased probability of survival, but viability assessment failed to identity patients with a survival benefit from surgical revascularisation compared with medical therapy alone. The results need to be interpreted with caution because the study definition of viability included myocardial segments that were viable, but not necessarily dysfunctional, and hence not necessarily either hibernating of even ischaemic. In addition, viability assessment was performed in a non-randomised fashion in only 50% of patients, leading to the potential for significant recruitment bias.
Positron emission tomography
PET is another option for assessing myocardial perfusion and is considered the non-invasive gold standard for this indication because of its capacity to provide accurate and reproducible measures of perfusion in absolute terms (ml/g/min) both at rest and stress. Its clinical utility, however, is constrained by high cost and low availability compared with SPECT.
PET has also been used for risk stratification. Its overall prognostic value has been demonstrated in several studies. In particular, measurement of coronary flow reserve offers additional prognostic information over qualitative analysis and SPECT MPS.19 PET has also been considered for many years as the gold standard for assessment of myocardial viability and hibernation using metabolic tracers. Dysfunctional myocardial segments with higher FDG uptake compared with that of ammonia or rubidium-82 (mismatch between perfusion and metabolism) represent hibernating myocardium, while reduction of both perfusion and metabolism corresponds with myocardial scar. In cases of myocardial stunning, perfusion is normal or almost normal while FDG uptake is variable.
PET is the only modality at present for which there is good quality information from a randomised study (PARR-2) demonstrating that patients with severe LV dysfunction whose therapy was guided by FDG PET have better outcome than with standard care.20
Conclusions
Nuclear cardiology techniques and MPS in particular have proven value for the diagnosis and prognosis of CAD in a safe and cost-effective way. Experience with the techniques can be measured over decades and there is a wide body of evidence to support their integration into investigative strategies for CAD.
- © 2012 Royal College of Physicians
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.