
Lesson
A 39-year-old slim, fit and healthy female, with no known cardiovascular risk factors, presented with severe chest and back pain of sudden onset, radiating to the throat. This was associated with numbness in both arms, shortness of breath and palpitations, and was followed immediately by loss of consciousness and limb jerking lasting approximately 1 min. She continued to have ongoing pain on regaining consciousness and complained of temporary visual loss. After 5 min, she had further loss of consciousness and a witnessed tonic–clonic seizure with a brief (45 s) respiratory arrest. She had no previous medical history and was taking no regular medication. Clinical examination was normal, with no detectable neurological or visual deficit. Her electrocardiogram (ECG) showed sinus rhythm with antero-septal ST segment elevation and inferior ST segment depression, antero-septal Q waves and some loss of R wave voltage anteriorly.
Computer tomography (CT) scanning in the admitting hospital excluded aortic dissection and subarachnoid haemorrhage, but the brain CT demonstrated a small left lentiform nucleus lacunar infarct. She was transferred urgently to our institution, where bedside trans-thoracic echocardiography revealed apical and anterior left ventricular (LV) wall akinesis and overall moderate systolic dysfunction; subsequent cardiac biomarkers were markedly raised (troponin I 71 ug/L and creatine kinase 2049 iu/L). Serum cholesterol was normal (4.0 mmol/L). Coronary angiography revealed a large volume of thrombus within the distal diagonal vessel, with visible thrombotic occlusion of the left anterior descending coronary artery (Fig 1). The right and circumflex coronary arteries were normal. Trans-thoracic echocardiography was repeated with trans-pulmonary contrast, which confirmed the absence of LV thrombus.
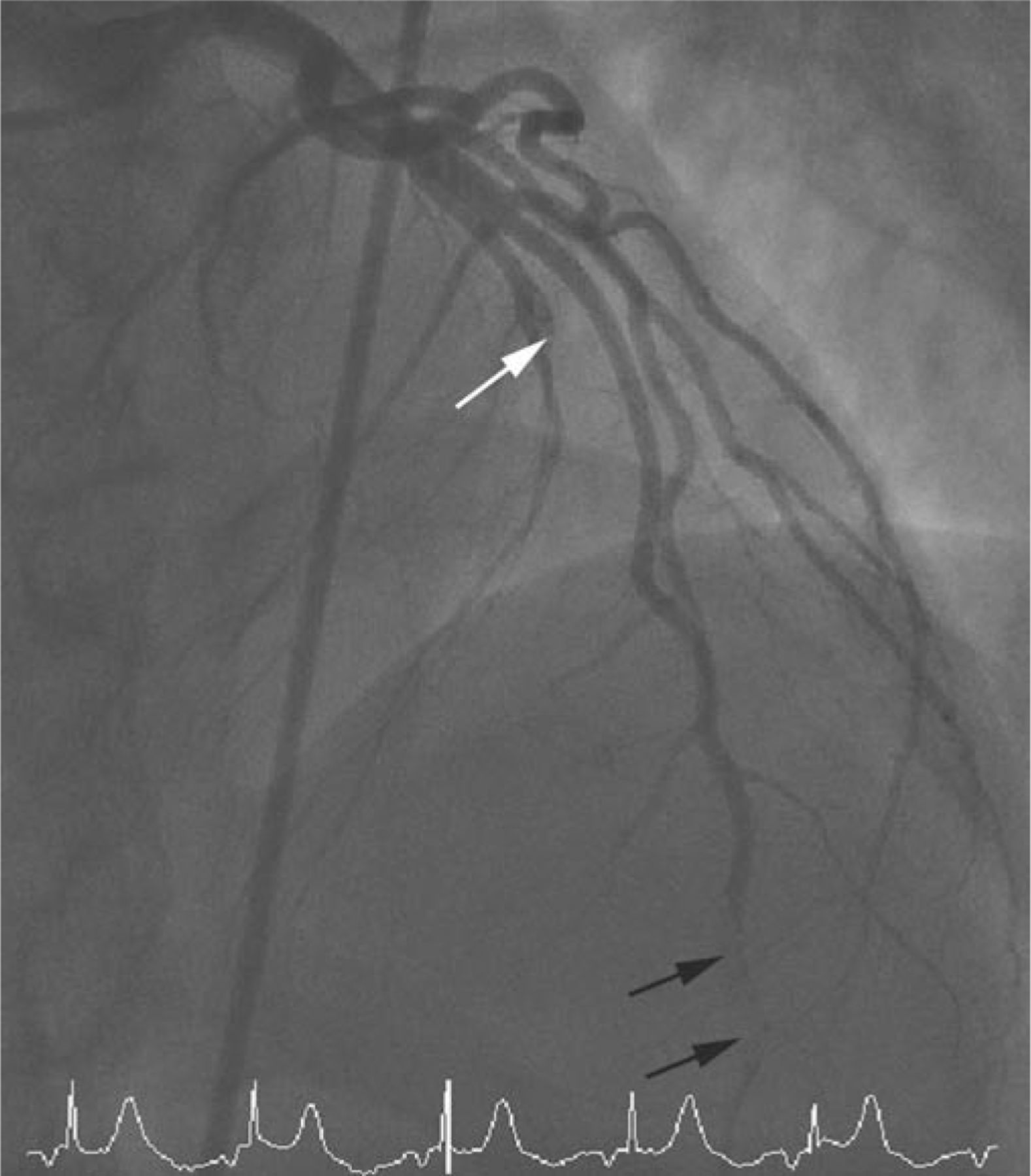
Right anterior oblique projection from the coronary angiogram demonstrating abrupt occlusion of the left anterior descending (LAD) coronary artery (white arrow) as well as a large filling defect (thrombus) in the distal portion of the diagonal branch of the LAD (black arrows).
In view of the simultaneous presence of a cerebral lacunar infarct and thrombus in two coronary arteries, paradoxical emboli were suspected. Repeat echocardiography with injection of agitated saline demonstrated clear interatrial shunting (Fig 2) and transoesophageal echocardiography (TOE) confirmed the presence of a patent foramen ovale (PFO) and no obvious thrombus in the atria or their appendages.

An apical view from the transthoracic echocardiogram following intravenous injection of agitated saline showing clear (abnormal) presence of bubbles within the left heart. LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle.
A duplex ultrasound scan showed no evidence of deep venous thrombosis in the legs or pelvis, and blood screening for inherited and sporadic thrombophilia, vasculitis and antiphospholipid syndrome was also normal. She was discharged on usual cardiovascular secondary prevention medication, as well as warfarin, and underwent successful percutaneous device closure of her PFO ovale four weeks later.
Discussion
Paradoxical embolism is a recognised complication of PFO and case reports have linked it to ischaemic stroke1,2 or acute myocardial infarction (MI).3 The differential diagnosis of a patient presenting with an acute ischaemic stroke and MI simultaneously is broad and is listed in Table 1. Initial management can be challenging, as the need to initiate anti-platelet and anti-thrombotic therapy has to be balanced with the risk of haemorrhagic transformation of the cerebral infarction. This case represents, to the best of our knowledge, the first report of ischaemic events owing to paradoxical emboli occurring simultaneously in the arterial circulations of both the brain and the heart. This case report acts as a lesson that paradoxical emboli through a PFO (ie intra-cardiac shunting) should be considered in young patients presenting with simultaneous stroke and myocardial infarction.
Differential diagnosis of a patient presenting with simultaneous myocardial infarction and stroke categorised by cardiovascular and non-cardiovascular causes.
- © 2012 Royal College of Physicians








{kind=link}
{kind=link}