
Abstract
Clinical research contributes to the evidence base for the planning of improved healthcare services and creates an excellent environment for the delivery of healthcare and the recruitment and retention of excellent and well-motivated staff. In this paper, we consider the evidence that a research-intensive healthcare system might yield improved outcomes as a result of the impact of the process of research on the provision of care. We review progress in establishing clinical research networks for cancer and the evidence of the impact of the conduct of clinical cancer research in the National Health Service.
Introduction
The development of new knowledge to underpin the planning of new healthcare initiatives is a clear and explicit product from clinical research. However, it has been hypothesised that the process of clinical research itself can result in improved outcomes directly by improving the outcomes for individual trial patients and/or indirectly by improving the quality of healthcare services in research-active healthcare institutions. The studies of benefits for individual trial patients, compared with similar patients in the same institutions, are not extensive but are broadly negative, as has been previously reviewed.1–3 This evidence is insufficient to support the hypothesis that an individual patient will benefit compared with a similar patient in that same service, and investigators should not advise patients that there are individual benefits to them from agreeing to randomisation in a randomised controlled trial (RCT) or other study. By contrast, the limited available evidence4–7 does suggest that healthcare outcomes are better in research-active healthcare systems. However, the literature to support this conclusion is modest and there is a need for further research. It is nonetheless reasonable to discuss with patients that being managed in research-active healthcare institutions is desirable. Patients should feel confident that their care will be at least as good as any elsewhere and that healthcare services in research-active National Health Service (NHS) institutions might be better.
The mechanisms by which research activity can improve outcomes are not clearly understood. Clinical research requires high-quality infrastructure, including technologies, estate and expert clinical teams. Staff have to be trained to a high standard and processes of care are systematised through clinical trial protocols. Clinical research is generally seen as prestigious and promotes recruitment and retention of high-quality staff.8 For example, the Radiotherapy Trials Quality Assurance (RTTQA) Programme designs and implements quality assurance (QA) programmes for all National Institute of Health Research (NIHR) portfolio cancer trials that include a radiotherapy component and, by doing so, enables the safe and standardised implementation of new radiotherapy protocols, which then go on to drive training and uptake of new practices and/or techniques across the NHS.
In the developing world, the consequences of research activity can be more readily demonstrated. For example, studies of cancer screening in India and sub-Saharan Africa are associated with establishing training programmes and infrastructure for clinical care that outlast the period of the trial itself.9 In this setting, there is a readily demonstrable link between the instigation of clinical research and the establishment of excellent clinical care. Examples include the development of public health policy for cervical cancer screening in India; the augmentation of trained human resources for oral, breast and cervical cancer screening in India; improved public and professional awareness and early detection of lesions and improved healthcare infrastructure for early detection, diagnosis and treatment of such lesions.9
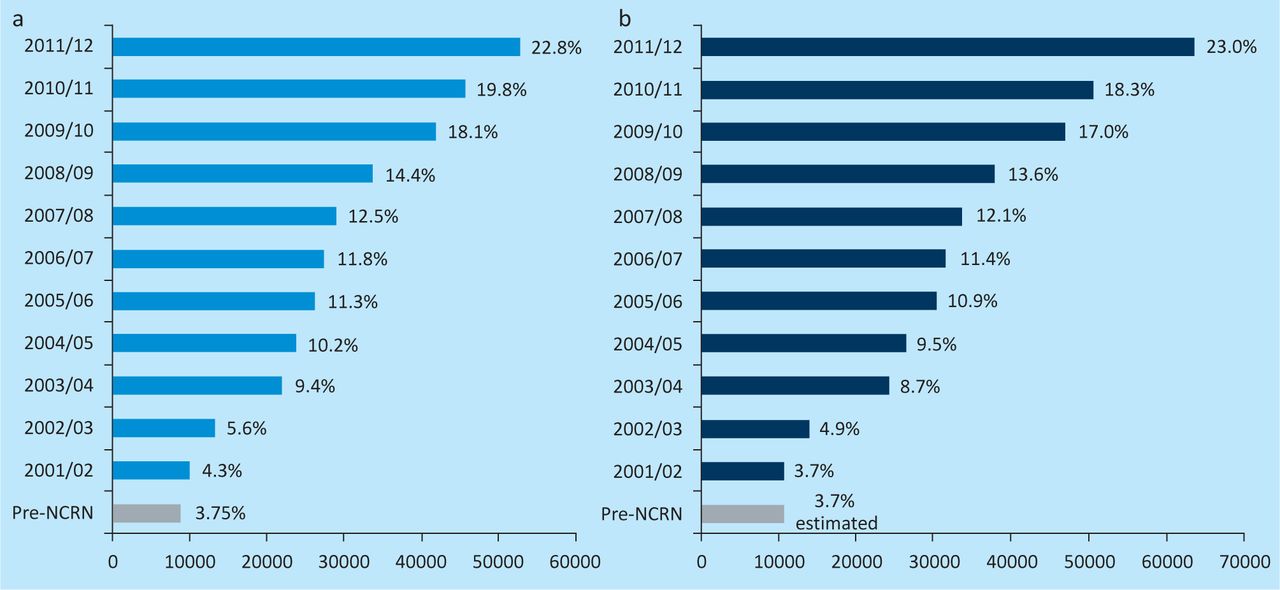
A key component of the support for clinical research in the NHS in the UK has been the development of clinical research networks (CRN).10–12 These were established sequentially in cancer, mental health, dementias and neurodegenerative diseases, diabetes, medicines for children, stroke, primary care and a comprehensive network, and are now collectively referred to in England as the NIHR CRN. In 2010–11, 564,698 people were entered into NIHR CRN portfolio studies, representing more than a doubling of previous documented recruitment; this also means that approximately 1% of the population of England entered trials or studies in each year.13 In 2012, 98% of NHS organisations are currently active in research, and we are unaware of any healthcare system with a comparable level of engagement in research. All of the CRNs have evidence of their individual success in increasing research activity within the NHS. The longest period of observation relates to cancer in the National Institute for Health Research Cancer Research Network (NCRN) (Fig 1), 11 which we discuss further here.

National Institute for Health Research Cancer Research Network (NCRN) studies between 2001 and 2012. Overall recruitment to NCRN portfolio studies in (a) England and (b) the UK as a whole, as a percentage of new cancer cases.
The development of infrastructure for clinical research in the NHS in England was closely integrated with the development of cancer networks, which provided an innovative planned approach to the provision of cancer services, especially to ensure multidisciplinary team working, specialised care and appropriate provision in primary, secondary and tertiary care. The reorganisation into cancer services gathered momentum during the late 1990s. A proposal to promote clinical cancer research by providing infrastructure support within the NHS was brought forward in 1999 and resources were provided by the Department of Health for the development of the NCRN from 2000. Each of the then 34 cancer networks was provided with resources to recruit staff and provide support for the delivery of the clinical research portfolio of clinical trials and other well-designed studies. Local cancer research networks were led by clinicians with network managers. A close partnership between clinicians and managers was a strong theme in this leadership. Network staff included clinical research nurses, other clinical research practitioners and staff in radiology and pathology and pharmacy who were all crucial to the delivery of the clinical research portfolio. The cancer networks and, therefore, cancer research networks covered the country and were closely integrated. NCRN is led by a national coordinating centre, which is responsible for the overall performance management of the NCRN and supports national initiatives to develop the research portfolio and develop the workforce. The organisation sought to achieve a balance between national consistency and local ownership of the initiative. Although the NCRN was responsible for a national portfolio of trials and other well-designed studies, local networks were able to select those parts of the portfolio that suited their strengths and the commitment of their clinical staff. The networks were actively managed with targets set by the Department of Health for patient recruitment and, as the organisation developed, priorities were set for randomised clinical trials and for the delivery of clinical studies and trials within the timespan allotted by the research funder and with the number of patients necessary to achieve their scientific goals. The initiative in England was linked to similar initiatives with slightly different models in Wales, Scotland and Northern Ireland, and integrated working at the UK level was a priority. The recruitment of patients into NCRN portfolio studies in England and across the whole of the UK is shown in Fig 1.
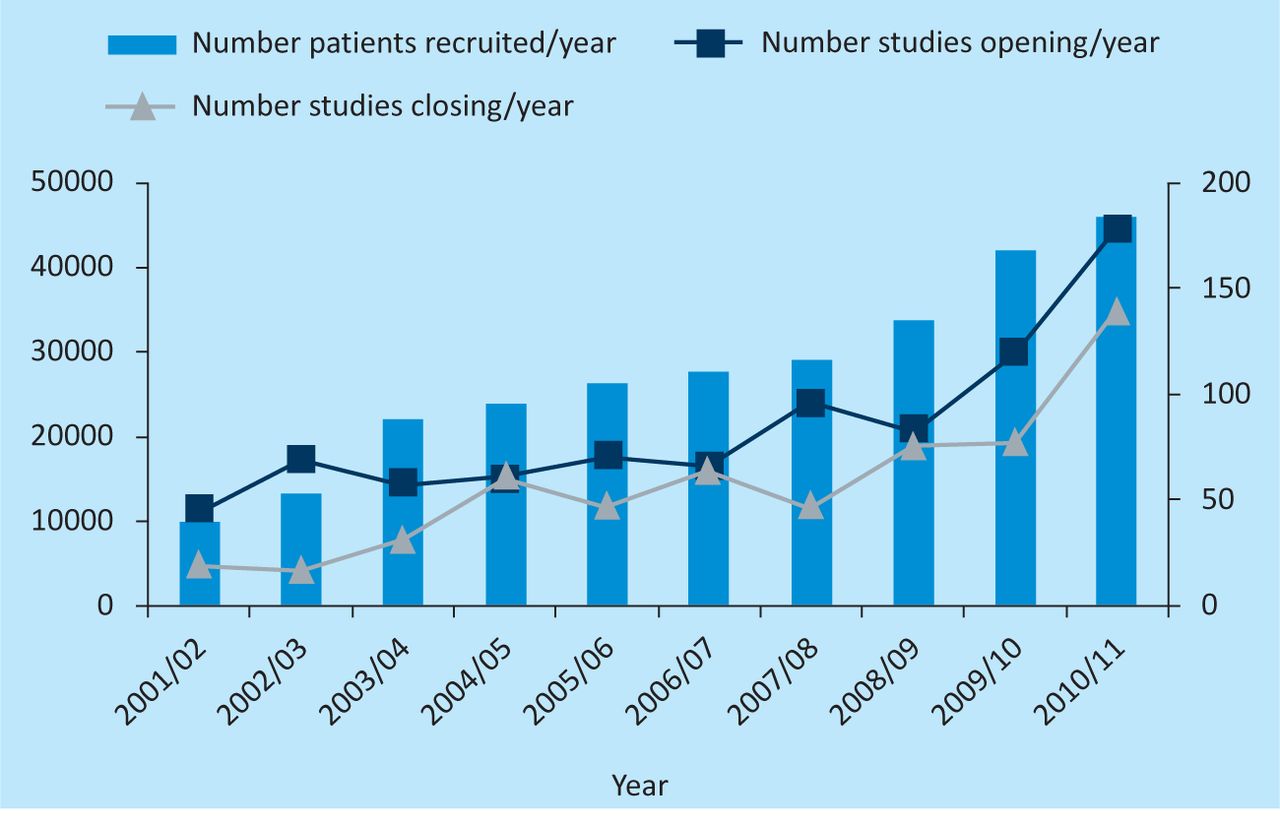
There is clear evidence of a continuing remarkable increase in recruitment and of an achievement well beyond the original goal of doubling recruitment into RCTs and other well-designed studies. The increasing recruitment was widely spread across the whole of the UK, including rapidly increasing clinical research activity in parts of the country that had previously seen little or no such activity. Although there were increases in study numbers and recruitment in the traditionally strong areas of clinical cancer research, such as breast cancer and haematology, there was also substantial growth in the recruitment into trials in rare diseases. The peer-reviewed research portfolio has steadily grown, with increasing study numbers opening each year and being completed in a timely way (Fig 2). The route by which studies and trials enter the portfolio is tightly defined and quality assured by the funders of the individual study and/or trial. The trials must conduct research that has undergone high-quality peer review at an international and/or national level for it to enter the portfolio. However, once this has been done, there is no additional process of scientific peer review by the network. The job of the network is to promote the development of the portfolio through supporting clinical studies groups (CSG) in all major cancer sites and special topics, to accept studies peer reviewed by funders, and to deliver the research within the NHS.
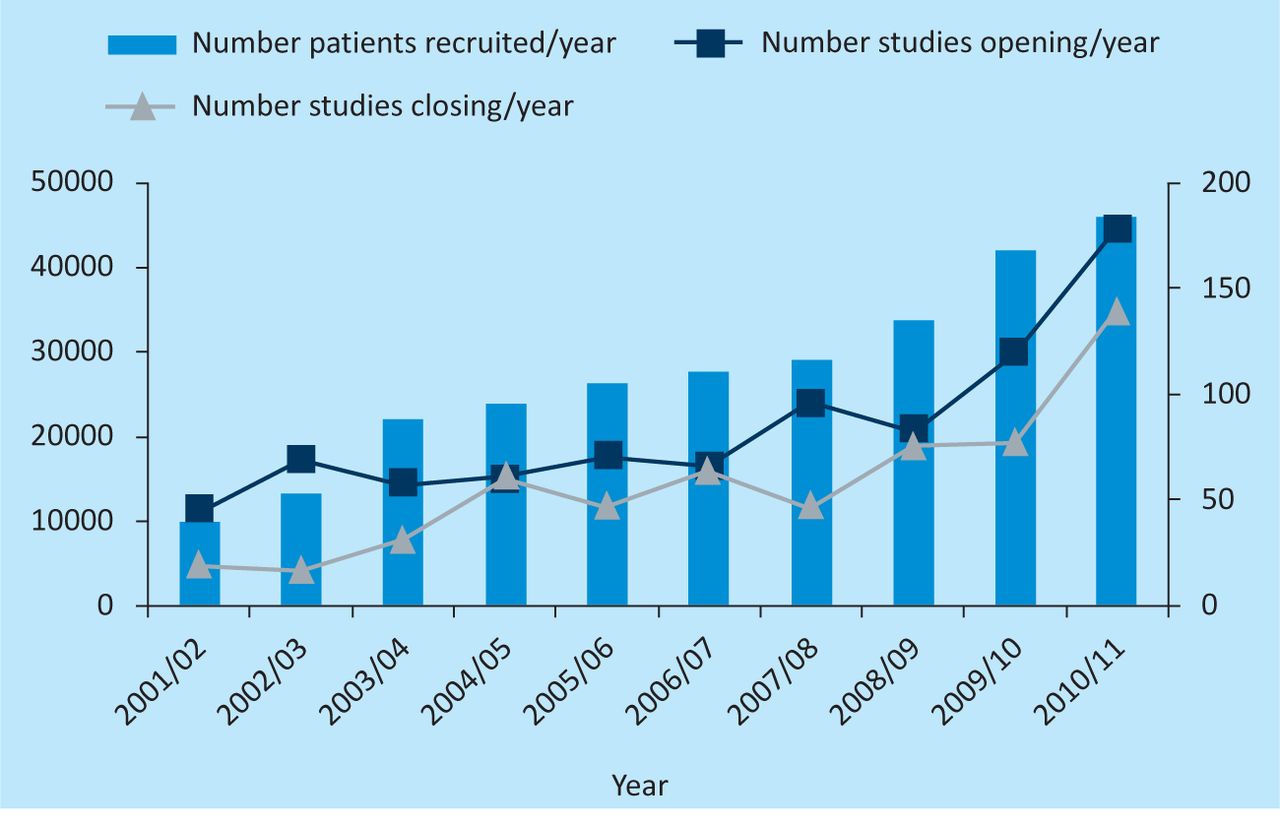
The absolute number of patients recruited per year into NCRN portfolio studies (left axis) and the number of studies in the portfolio and open and closing in each year (right axis). NCRN = National Institute for Health Research Cancer Research Network.
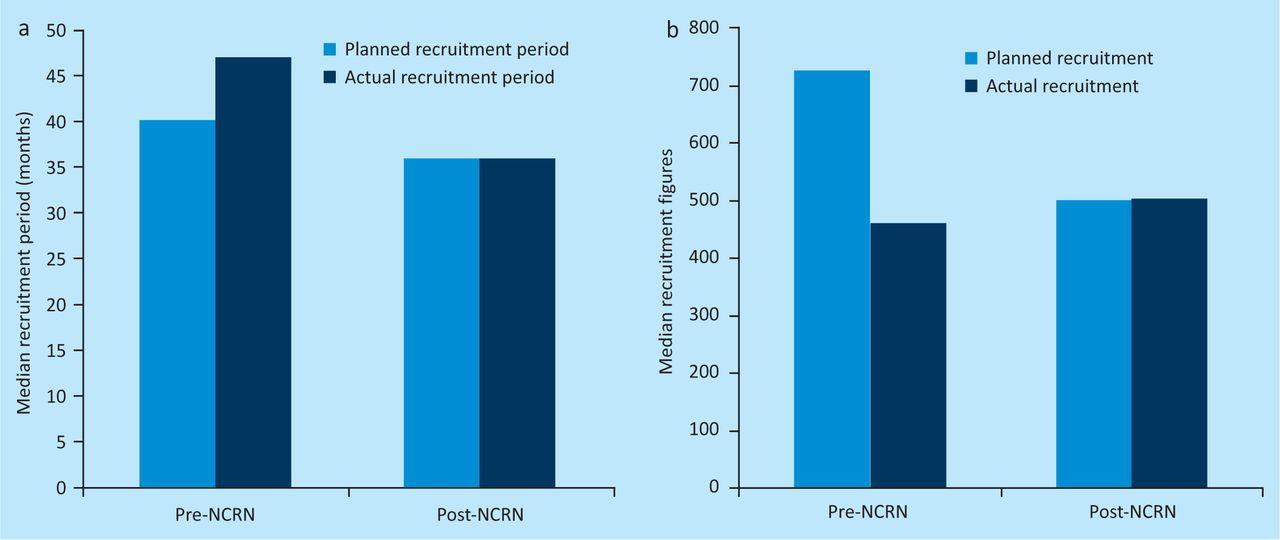
The delivery of study targets for recruitment in a timely way is an important part of the work of the NCRN and this was studied by Stead et al. (Fig 3).12

The impact of the NCRN on the speed of recruitment. (a) pre-NCRN planned and actual recruitment periods indicate that the actual recruitment period exceeded the planned recruitment period. Post-NCRN planned and actual median recruitment periods were identical. (b) pre-NCRN planned recruitment numbers and actual recruitment numbers indicate the actual recruitment fell well short of planned recruitment. Post-NCRN the actual median recruitment figures match the planned median recruitment figures.
Before the establishment of the NCRN, the median recruitment periods exceeded the planned periods and median recruitment numbers were less than targets. Post NCRN, these medians were both on target and 74% of trials recruited to target compared with 30% before the NCRN.12
A large number of practice-changing randomised trials have been supported through this route (Table 1).
Examples of practice-changing randomised trials that have been supported by the NCRN.
Patient and public involvement has been central to this process and over 1,000 patients have been involved in the development of clinical research and the CRNs. There is good descriptive evidence of an impact on the quality of clinical research from patient and public involvement, and work continues to improve the effectiveness of this process.14
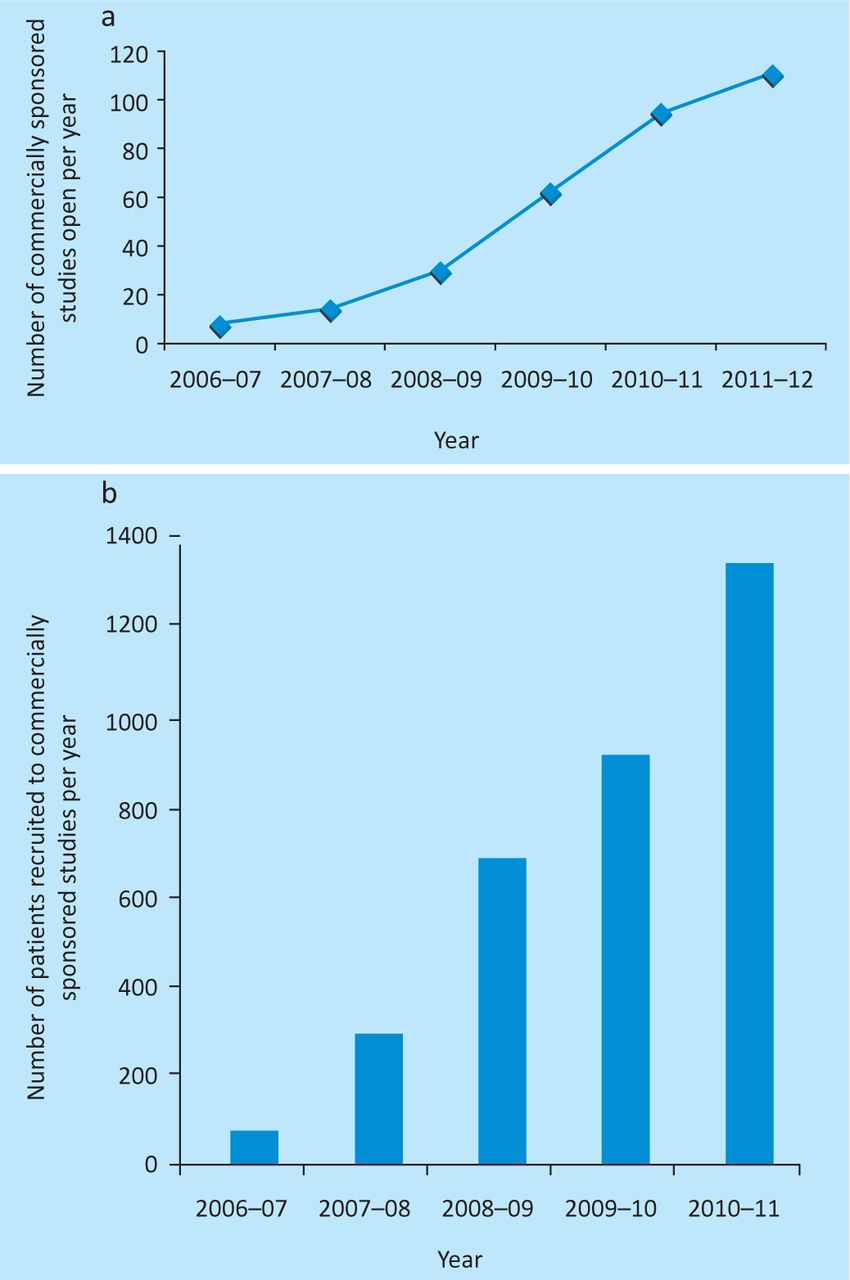
Increasingly, economic pressures to ensure best value from each new therapy, coupled with the excellent translational research opportunities in the UK, enable the focus of NIHR and CRNs to shift towards clinical research that, although increasingly sponsored by industry, can help identify the subgroups of patients in whom new therapies are most effective. This represents an opportunity for the NHS to contribute to the strength of an important part of the UK economy at the same time as improving the potential cost-effectiveness of new therapies. This new emphasis has seen a rapid growth in the recruitment of patients into industry-funded studies (Fig 4) and an impressive increase in the ability of the NHS to support pharmaceutical and biotech-sponsored studies to time and target (Fig 5).
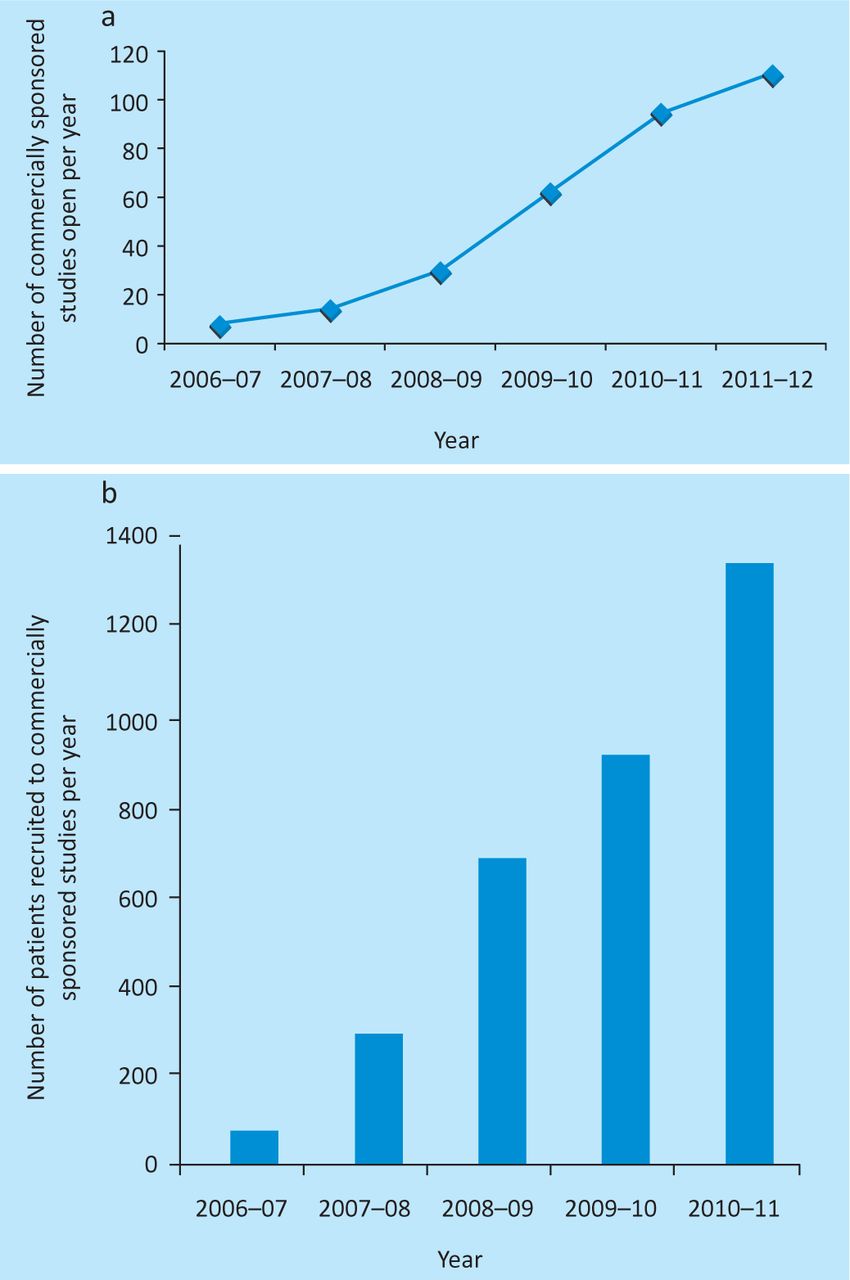
Recruitment of patients into industry-funded studies in the UK. (a) Number of commercially sponsored cancer network studies open to recruitment in-year. (b) Patient recruitment to commercially sponsored cancer network studies per year.

Percentage of commercially sponsored studies recruiting to time and target in the UK
The expansion of commercially sponsored research also provides NHS patients and clinicians with improved or earlier access to novel agents, some of which will be found to provide superior outcomes. The network experience so far suggests that active academic and commercially sponsored clinical research portfolios can be highly complementary, or even synergistic, with more available studies leading to more clinicians and patients interested in participating in research, thus improving the evidence base for the NHS. Furthermore, the interactions of clinicians with pharmaceutical and biotechnology companies can make possible research opportunities and trials that would otherwise be difficult to develop or organise, such as in rare disease types. The Industry Alliance programme between NCRN and, initially, AstraZeneca, and now including GlaxoSmithKline, has established an innovative and uniquely collaborative way for academic clinical researchers and industry clinical scientists to engage productively to address research needs that have no immediate commercial applicability but are considered important to NHS clinicians. Industry has realised the potential of the NCRN and the National Cancer Research Institute (NCRI) CSGs to provide seamless expertise in clinical academic science, trial design and delivery, enhancing the speed and breadth of development of their pipeline of novel compounds. For their part, the UK clinical academic community and CRNs have welcomed the opportunity to work with novel pipeline compounds, and design and deliver innovative phase II trials, often in patient populations that would not normally have access to novel compounds.
External peer review has been very positive about the achievements of the NCRN and of the non-cancer initiatives that have followed. The direct benefits of investment by the UK Government in NHS clinical research and in clinical research infrastructure are apparent and have been the subject of positive international comment. Many factors have contributed to the success of the CRNs but we would like to highlight the effective partnership between research funders, the clinical investigator community that generates the research portfolio, CRNs embedded in the NHS, NHS host organisations and managers, and Government departments. Perhaps most crucial to the success of these developments has been the engagement of healthcare professionals of all the clinical professions in the generation and delivery of the research and the commitment of patients to the development of a successful research portfolio and evidence-based NHS and to consent to join their studies in such large numbers.
Conclusions
An actively managed national approach to developing clinical research for patients with cancer began in 2000 with the initiation of the NCRN. This is generating a large portfolio of evidence, increasingly delivered within the original planned timelines, which will inform the future of healthcare provision. In addition, it is testing the hypothesis that a research-intensive healthcare system per se, through its influence on the quality of healthcare in the host institutions, could improve outcomes for patients. This question is of considerable interest to policy makers. It increases the argument for clinical research activity in the NHS and in healthcare systems across the world and should provide some reassurance for patients and carers who are central to the provision of care and also to the development of clinical research. There has been considerable progress to date, and this has been mirrored in other subjects that have adopted this approach. Since 2006, the development of the NIHR in England, and similar parallel developments in the other nations of the UK, have provided impetus and support for clinical and applied health research across the NHS, which should bring increasing benefits to patients.
Acknowledgements
We would like to acknowledge warmly the funding for NCRN and NIHR CRN from the Department of Health, NIHR and the NCRI, the contributions of our colleagues and patients to clinical research in the NHS and the support of Sally Davies, Russell Hamilton and John Pattison for these initiatives. Janet Darbyshire was Joint Director of NIHR CRN and a key contributor to this work.
- © 2012 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}