
Abstract
The prevalence of obesity is rising worldwide, with the UK having the highest prevalence in Europe. Obesity is associated with significant morbidity and has substantial healthcare implications, with current projections estimating that by 2030 obesity will cost the NHS approximately £2 billion each year. Lifestyle modification remains the cornerstone of anti-obesity treatment, but drugs can be introduced as adjuncts to assist and maintain weight loss. Some 1.45 million obesity-related prescriptions were dispensed in 2009, highlighting the high demand for obesity pharmacotherapy. At present, the lipase inhibitor orlistat (Xenical) is the only UK-approved long-term medical therapy for obesity. Double-blind clinical trials have shown that orlistat significantly increases weight loss compared to placebo, but the array of adverse side effects associated with orlistat limits its tolerability. The need for more effective and better-tolerated anti-obesity medications is clear and six therapies have reached phase-III trials.
Background
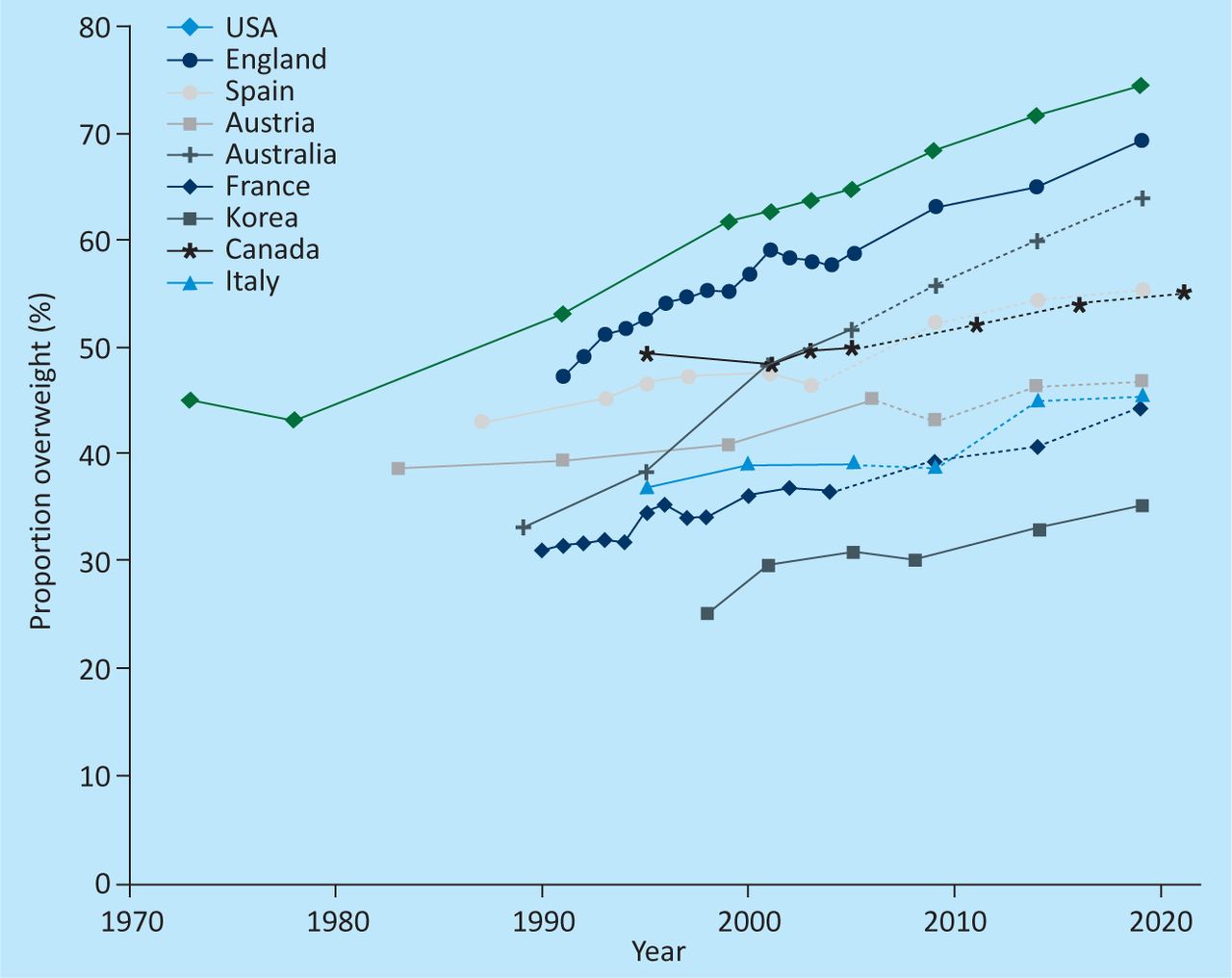
The incidence of obesity is rising worldwide and the UK is amongst the worst-affected countries, with 30% of adults in the UK being obese. In addition, 30% of UK children aged 2 to 15 are overweight or obese.1 The prevalence of obesity in the UK population is projected to reach 50% by 2050 (Fig 1),2,3 with the cost of this condition and its associated co-morbidities predicted to cost the NHS some £2 billion per year by 2030.3

Past and projected overweight trends by country.2
The terms ‘overweight’ and ‘obese’ are defined as having a body mass index (BMI) greater than 25 kg/m2 and 30 kg/m2, respectively. These values should, however, be used with caution as BMI is not a direct measure of adiposity. The National Institute of Clinical Excellence (NICE) recommends that waist circumference (above 88 cm for women or 102 cm for men being considered raised) is used in conjunction with BMI when describing the extent of obesity and predicting the extent of associated health risks.4
The development of obesity is characterised by the interplay of nature and nurture. Genetic factors that are known to predispose individuals to obesity were probably once advantageous in resource-deficient environments, where energy-conservation was essential for survival. With modern environments providing cheap energy-dense foods combined with increasingly sedentary lifestyles, these adaptive responses result in unnecessary retention of energy-rich adipose tissue.5 This increased mass, and the released chemokines, are deemed responsible for obesity-related morbidity and mortality from conditions such as type 2 diabetes, cardiovascular and liver disease, and cancers.4
A growing body of evidence suggests that maternal obesity might increase the offspring's propensity to obesity in adulthood through epigenetic alteration of fetal physiology.6 This is especially important in the UK, where about one in five women of reproductive age are obese,7 as failure to address maternal obesity might be leading to developmental programming effects that will further compound the growing epidemic.
The financial implications of treating obesity itself are extensive, even without incorporating the huge costs of treating its co-morbidities and addressing its socioeconomic impacts. Almost 2 million prescriptions for obesity therapy were dispensed in 2009 (11 times more than the 127,000 in 1999)4 and the cost of the prescribed drugs (the ‘net ingredient cost’) has increased from £6.6 million in 2000 to a peak of £51.6 million.4
This review focuses on current treatment, recent changes in anti-obesity pharmacological agents and forthcoming interventions.
Current interventions
At present, lifestyle modifications, adjunct pharmacotherapy, and endoscopic (intra-gastric balloons and endosleeve)8,9 and surgical interventions are the mainstays of management of obesity and its sequelae.10 The clinical benefit of moderate weight loss (5–10% of total body weight)11 is manifest in improved quality of life and reduced risk of related morbidities.
Although lifestyle modification remains the cornerstone of anti-obesity intervention, it only produces short-term weight loss as patients have generally experienced significant weight regain after just two years.12 Consequently, NICE guidelines indicate the use of adjunct pharmacotherapy.13
Anti-obesity medications in current or recent use can be categorised according to one of three modes of action:14
inhibitors of fat absorption
inhibitors of the endocannabinoid system
modifiers of central nervous system neurotransmission of norepinephrine, dopamine and serotonin.
At present, orlistat is the only anti-obesity drug approved by the European Medicines Act (EMA) and the Food and Drug Administration (FDA). This drug is a pancreatic lipase inhibitor that binds to lipase in the gut lumen, preventing the hydrolysis and normal metabolism of dietary fat (triglycerides)15 and hence reducing its absorption. In a recent Cochrane meta-analysis (n = 6196 patients) of 13 double-blind, placebo randomised controlled trials (RCTs),14 participants receiving orlistat (120 mg, three times daily) in conjunction with appropriate lifestyle modifications lost, on average, 2.9% more (95% confidence interval (CI) 2.5–3.4%) than those given a placebo. Sub-analysis further demonstrated that 26% of those given orlistat lost ≥10% of total body weight, while 30% this group lost ≥5%. In the placebo group, just 14% lost ≥10% and 19% lost ≥5%. However, long-term treatment resulted in similar levels of weight regain in those who took orlistat and placebo.14 ‘Xendos’, a four-year double-blind placebo-controlled RCT of 3,305 non-diabetic Swedish obese patients showed that orlistat reduced the risk of developing type 2 diabetes by 37.3% (primary outcome) compared to placebo (lifestyle modification).16 Additionally, orlistat has been shown to modestly improve risk factors of obesity-related co-morbidities, such as blood pressure, glycaemic profile and lipid parameters, in adolescents and adults.14
The majority of the adverse events associated with orlistat are mechanistically related to the malabsorption of fat within the gastrointestinal tract: steatorrhoea, bloating, and malabsorption of fat-soluble vitamins such as vitamin A, D, E and K. In a meta-analysis of 14 double-blind, placebo RCTs, 80% of orlistat patients reported at least one gastrointestinal event, with an absolute frequency 24% greater than in those given placebo alone (95% CI, 20–29%). The most common side effects are faecal urgency, fatty or oily stool and oily spotting, at frequency rates of 15–30% in most studies, and these can be associated with faecal incontinence and abdominal discomfort.14 Outside the rigours of clinical trials, these side effects are even more ubiquitous. The absorption of fat-soluble drugs (amiodarone, ciclosporin, warfarin and thyroxine) has also been shown to be affected. Furthermore, the EMA is currently reviewing reports of possible liver toxicity linked with orlistat.17
Withdrawn pharmacotherapy
Many anti-obesity medications, like drugs in most fields of pharmacotherapy, have been withdrawn after licensing because of safety concerns and adverse events that outweigh the modest benefits of treatment (Table 1).18
Initially approved pharmacotherapy and their current status. 18.
Two anti-obesity drugs have been approved by NICE but subsequently withdrawn: Rimonabant in 20094 and Sibutramine in 2010.13
Phase-III clinical trials
There are currently a multitude of Phase-III potential anti-obesity pharmacological innovations.
Monotherapy
Lorcaserin is a selective 5HT2c agonist that affects serotonergic pathways within the hypothalamus. 5HT receptors have been targeted by anti-obesity drugs, but these agents were withdrawn because of non-specific reactivity that evoked cardiac valve disease and pulmonary hypertension.19
BLOOM (Behavioural modification and Lorcaserin for Overweight and Obesity Management), the phase-III clinical trial of lorcaserin, was conducted over two years. The BLOOM trial enrolled 3,182 overweight or obese patients (with at least one co-morbidity, though diabetes was excluded) who received 10 mg lorcaserin or placebo twice a day, alongside lifestyle modification.19 At the end of year one, 47.5% of those receiving lorcaserin compared to 20.3% of those receiving placebo (p<0.001) lost >5% of their baseline body weight, and 22.6% of those receiving lorcaserin compared to 7.7% of those receiving placebo (p<0.001) lost >10%. Additionally, lorcaserin significantly reduced waist circumference, BMI, fasting glucose, fasting insulin, glycosylated haemoglobin levels, total cholesterol, LDL cholesterol, triglyceride levels, C-reactive protein, fibrinogen levels, and systolic and diastolic blood pressure. More profound weight loss was observed in year two. Possible side effects of locaserin included headache, dizziness and nausea, but these were not significantly different to the side effects reported by the placebo group.
Cetilistat, like orlistat, is a lipase inhibitor that reduces fat absorption. In a 12-week phase-II double-blinded RCT (n = 447), cetilistat in combination with a hypocaloric diet produced significantly greater weight loss than placebo, with a dose-related response for 60, 120 and 240 mg three times daily. The results are comparable to those for orlistat, with approximately 30% of those treated experiencing ≥5% weight loss compared to 17% of the placebo group. Waist circumference, total cholesterol and LDL levels were also significantly reduced by each dose of cetilistat.20 The adverse side effects of cetilistat are similar to those reported with orlistat, although such events were less frequent, suggesting better tolerability and therefore compliance.20,21
Liraglutide is a glucagon-like peptide-1 (GLP-1) analogue of the endogenous gut-derived hormone incretin. It is already known to improve glycosylated haemoglobin concentrations, beta cell function and systolic blood pressure.22 Furthermore, it has been shown to facilitate weight loss in diabetic patients in a dose-dependent manner22 and it is currently licensed as an anti-diabetic drug. Liraglutide is now being trialled in phase-III studies to assess its efficacy in promoting weight loss in obese, non-diabetic patients. Owing to its 13-hour half-life, the administration of liraglutide involves a daily subcutaneous injection. In a double-blind, placebo RCT (n = 564), non-diabetic obese participants (aged 18–65) were randomly assigned to either a placebo injection or one of four doses of liraglutide (1.2 mg, 1.8 mg, 2.4 mg or 3.0 mg daily). The responses of these participants were compared to those of people given open label orlistat (120 mg, three times daily) with life style modification. At the end of the 20-week trial, those given liraglutide had lost significantly more weight than those on orlistat or placebo, and the response to liraglutide was dose dependent (weight loss range 4.8–7.2 kg).22
The influence of liraglutide treatment on secondary outcomes was equally impressive: liraglutide (2.4 and 3.0 mg) reduced the prevalence of pre-diabetes, lowered blood pressure and significantly improved quality of life compared to orlistat and placebo.22 Liraglutide was generally well tolerated.22
Combination therapy
Contrave is a fixed-dose combination of bupropion, a non-selective dopamine and norepinephrine-reuptake inhibitor, and naltrexone, a mu-opioid receptor antagonist. Three randomised, double-blind, placebo-controlled, 56-week studies were carried out on approximately 1,650 participants.23 Weight loss in those given the combined treatment started as early as week four and was continuous; weight loss at 56 weeks was significantly greater than placebo and the combined treatment resulted in significant improvements in waist circumference, insulin resistance, and concentrations of HDL cholesterol, triglycerides, and C-reactive protein.23
The most frequent adverse event in participants given the Contrave treatment was nausea, but headache, constipation, dizziness, vomiting, and dry mouth were also more frequent in treated participants than in those given placebo.23 In light of concerns regarding psychiatric side-effects attributed to bupropion, specifically a depressed mood, a specific 24-week Phase-III trial was conducted in obese and overweight patients who had major depressive illness. Reassuringly, it was concluded that Contrave significantly ameliorated depressive symptoms.24
Qnexa is a combination of phentermine, an appetite suppressant, and topiramate, an anticonvulsant that has weight loss as a side effect. Preliminary data have shown benefits in lowering blood pressure and serum cholesterol. The first trial, ‘Equate’, assessed the effect of mid- and full-dose combinations in 756 lifestyle-modified and diet-restricted obese patients over a 28-week period. Impressively, Qnexa mid doses (7.5 mg phentermine–46 mg to piramate) and full doses (15 mg phentermine–92 mg topiramate) were associated with average weight losses of 8.5% and 9.2% of body weight, respectively.24 Placebo controls lost only 1.7%. Amongst participants on full-dose Qnexa, 66% lost ≥5% and 41% lost ≥10% of body weight, contrasting with participants on placebo, 15% of whom lost ≥5% and 7% of whom lost ≥10%.24 Further studies demonstrated an average weight loss of 10% in more than 60% of study participants over a 52-week period.24 Side effects of Qnexa included dry mouth, paraesthesia, constipation, altered taste and insomnia.24
Empatic is another therapy that combines bupropion and zonisamide's appetite-suppressing qualities. A pilot clinical study of 18 diet-restricted obese women with a mean BMI of 36.8 kg/m2, in which the combination treatment was compared against zonisamide in isolation, was conducted over 12 weeks. The results showed a 7.5% loss in the combination treatment, compared with just 3.1% in zonisamide alone.24 Main adverse events were headache, insomnia and nausea. Importantly, zonisamide has been associated with cognitive impairment, mood disorders and, potentially, teratogenicity and hence further testing is required before marketing.24
Discussion
The rising epidemic of obesity is rapidly becoming a healthcare catastrophe in developed countries. Its growing impact on healthcare systems is becoming unsustainable and urgent advances in treatment are needed. Obesity is still widely decried as a lifestyle ‘choice’, but even determined changes in lifestyle have very limited long-term impact on it and, pragmatically, the need for medical intervention is now clear. Surgical or endoscopic bariatric procedures are effective therapies for obesity, but bariatric surgery in particular carries significant peri-operative morbidity and mortality.10 Moreover, it is very expensive and thus restricted in many healthcare systems. Therefore, there is clearly an important role for pharmacotherapy as an adjunct to lifestyle changes in some patients, and potentially a role as a bridge to safer surgical intervention in others.
Current pharmacological intervention in obesity is limited by the availability of licensed drugs and by drug efficacy and side effects. Orlistat remains the sole medication licensed for the treatment of obesity in the UK. Although numerous studies have shown that orlistat can produce desired weight loss in the short term, maintained reduction of weight remains challenging. This is further compounded by NICE guidelines13 that recommend the use of orlistat for a maximum of two years. Moreover the efficacy of orlistat on obesity-related morbidity is ambiguous as cardiovascular outcomes and progression of type 2 diabetes remain largely unaffected by the treatment.
The development of new drugs is impeded by both the complexity of systemic pharmacotherapy and variables such as ethnicity and age. The varied distribution of metabolically active adipose tissue in different ethnic groups can affect a potential drug's efficacy, perhaps ultimately rendering it ineffective. The complex interplay of genetics, programming, environmental factors and psychosocial issues makes successful drug treatment an extremely challenging venture. In addition, as the prevalence of obesity is rising amongst children and adolescents, the demand for effective, sustainable treatments increases. At present, these groups are under-represented in drug development trials, compounding our ability to ascertain drug suitability across the patient spectrum.
The story of anti-obesity pharmacotherapy is littered with initially promising drug candidates that were eventually withdrawn because of safety concerns. This fate could engulf the new generation of drugs being trialled, but it seems likely that some will succeed. In particular, cetilistat and liraglutide appear to be suitable candidates for anti-obesity pharmacotherapy and are likely to have more robust safety profiles than other drugs that have been trialled. The results obtained from cetilistat treatment, in particular, can be likened to those obtained with orlistat but with better tolerability. This, in turn, should translate to greater patient compliance and hence better drug efficacy. We would expect cetilistat's safety to be very much comparable to that of orlistat. Liraglutide is already approved for the treatment of type II diabetes, a common obesity-related co-morbidity, causing weight loss in both diabetic and non-diabetic participants with transient tolerable side effects. The safety profile for this drug is also acceptable. The newer combination therapies also appear to carry much promise but will need extremely careful monitoring of side effects and safety in order to become acceptable as a treatment for obesity.
In conclusion, there is little doubt that obesity is a monumental challenge to health and healthcare systems and tackling it will require a multifaceted approach. This includes an important and growing role for pharmacotherapy. Existing medical therapy with orlistat is not entirely satisfactory and there have been many setbacks in anti-obesity drug development. There is, however, a glimmer of hope that a new generation of better tolerated, more efficacious and safer drugs for use in combination or monotherapy might be within reach. If both safety and long-term effectiveness can be demonstrated, we will shortly see changes in obesity management.
- © 2012 Royal College of Physicians








{kind=link}