
Key points
Microalbuminuria (30–300 mg/day) is the earliest marker of diabetic nephropathy and is currently used for screening
Modifiable cardiovascular risk factors should be carefully addressed
Good glycaemic control slows progression: a target HbA1c below 48 mmol/mol is recommended
A treatment blood pressure target of less than 130/80 mmHg is probably most appropriate but this remains an area of uncertainty
Angiotensin-converting enzyme inhibitors are first-line agents and reduce both blood pressure and progression of proteinuria
Diabetes is the commonest cause of end-stage renal disease in the developed world. Early diagnosis and aggressive management are essential for delaying the progression of diabetic nephropathy (DN) and preventing its associated morbidity and mortality.
The incidence of diabetic kidney disease is estimated to be 20–40% in both type 1 and type 2 diabetes. A complex interplay of genetic and environmental factors determines its development and progression (Box 1). Several studies have shown that the glomerular filtration rate (GFR) can deteriorate as rapidly as by 10 ml/min/year in diabetic patients with poorly controlled hypertension and macroalbuminuria.1
Risk factors for development of diabetic nephropathy.
Natural history and the importance of albuminuria
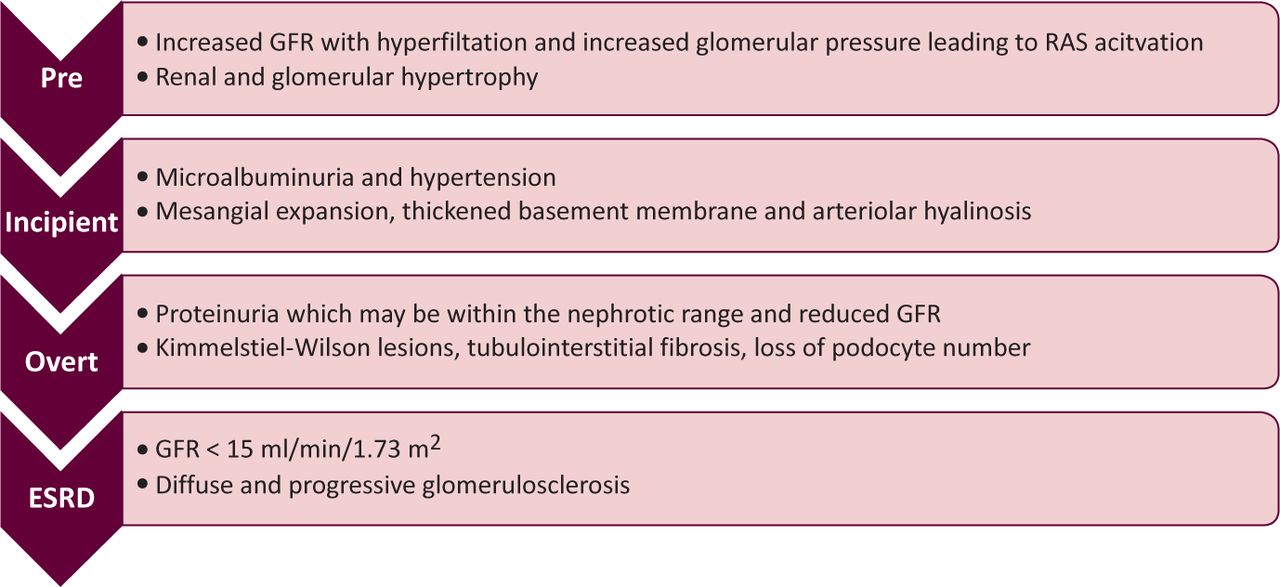
The natural history of DN has been established from studies examining type 1 diabetic patients which typically show a period of hyperfiltration followed by microalbuminuria (30–300 mg/day) and then by overt proteinuria accompanied by a decline in GFR (Fig 1).2 A similar progression is thought to underlie the evolution of nephropathy in type 2 diabetes, but confounding comorbidities, including hypertension and obesity, make a progressive pattern less clear.

Natural history of diabetic nephropathy (clinical findings and histological features) then overt proteinuria accompanied by a decline in GFR.2 ESRD 5 end-stage renal disease; GFR 5 glomerular filtration rate; RAS 5 renin-angiotensin system.
An important caveat is the recent appreciation that there is renal impairment (GFR, 60 ml/min/1.73m2) in a significant percentage of patients with both type 1 (22–24%) and type 2 (35–75%) diabetes in the presence of normal albumin excretion (although in type 2 this may be largely explained by ageing).3 Furthermore, microalbuminuria now frequently regresses, perhaps due in part to the widespread use of renin-angiotensin system (RAS) blockade.
Microalbuminuria does not therefore indicate established kidney disease but reflects a generalised and complex dysfunction of the vascular endothelium.4 As such it remains a powerful predictor of progression of both kidney5 and cardiovascular diseases.6 The establishment of overt albuminuria predicts functional decline, higher levels of albuminuria correlating with a more rapid decline in GFR.3
Diagnosis
Together with a clinical history of diabetes (usually ≥10 years), microalbuminuria is the earliest marker of DN independent of renal function. It is therefore recommended that diabetic patients should be screened annually by early morning albumin/creatinine ratio (in the absence of urinary tract infection) as well as serum creatinine and eGFR.7 There is a well established link between DN and other microvascular complications such as diabetic retinopathy and neuropathy, so extra vigilance is required in patients with these conditions. Non-diabetic renal disease may also occur and should be actively considered if there are certain clinical findings (Box 2).
When to consider an alternative renal diagnosis.
Management
There should be a multidisciplinary approach to managing patients with DN, focusing not only on slowing progression but also on modifying cardiovascular risk factors.
Lifestyle measures
The same lifestyle measures that apply to all patients with chronic kidney disease (CKD) also apply to patients with DN, including salt restriction, smoking cessation, exercise and maintaining a healthy weight. The latter (weight) is also important in patients being considered for transplantation as both higher body mass index and poor glycaemic control are associated with adverse outcomes.8
Cardiovascular disease prevention: guidelines
Renal disease and diabetes both increase overall cardiovascular risk. Given this, the 2005 Joint British Societies’ (JBS) guidelines suggest that diabetic patients with kidney disease do not require a formal cardiovascular risk assessment as they are already at significant risk. Formal treatment should be implemented where necessary.9
These guidelines suggest the use of statins in all diabetic patients over the age of 40 or who have evidence of end-organ damage, including nephropathy, whereas the Renal Association (RA)10 and the National Institute for Health and Clinical Excellence (NICE)7 advocate an estimation of cardiovascular risk prior to initiation of statin therapy. Once initiated, the target should be a 25% reduction from baseline or total cholesterol less than 4 mmol/l. The role of statins in patients on dialysis remains to be fully determined, but current RA guidelines recommend continuing statin therapy on dialysis unless complications develop.10
JBS guidelines suggest offering aspirin to all diabetic patients aged over 50 or who have had diabetes for 10 years or longer.9 However, recent meta-analyses have questioned the benefit of aspirin in primary prevention in diabetes.11 Treatment decisions should take into account both cardiovascular and bleeding risks.12
Glycaemic control
There is robust evidence that improved glycaemic control slows not only progression but also the onset of microalbuminuria in both type 1 and type 2 diabetes.13–16 Current UK recommendations aim for a glycosylated haemoglobin (HbA1c) below 48 mmol/mol (6.5%) whilst North American guidelines aim for less than 53 mmol/mol (7.0%).17 Early attainment of good glycaemic control produces the greatest benefit.18
The way this is achieved in type 2 diabetes is probably less important, but treatment should be targeted to the individual with consideration of their own needs, hypoglycaemic awareness and renal function.
Blood pressure control and renin-angiotensin system blockade
Hypertension is part of the natural history of DN; if uncontrolled, it contributes to progressive proteinuria and loss of renal function. In both type 1 and type 2 diabetes, NICE guidelines recommend a target blood pressure below 130/80 mmHg in those with evidence of end-organ damage (eg nephropathy).7 However, the recent ACCORD study in type 2 diabetes failed to show a reduction in cardiovascular events with a target systolic blood pressure of 120 mmHg compared with 140 mmHg. In fact, some outcomes were poorer,19 suggesting that a less aggressive target may be appropriate in patients with pre-existing cardiovascular disease.20
There is strong evidence that inhibition of the RAS in the form of either angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) slows the progression of DN14 and reduces proteinuria.21,22 These drugs should therefore be the first-choice antihypertensive agents. An increase in creatinine of up to 25% (or corresponding decline in eGFR) on institution of RAS blockade should be tolerated as there is still an overall benefit in preservation of renal function. When used in combination, ACEIs and ARBs may further reduce both blood pressure and proteinuria. However, following the ONTARGET trial, which revealed a greater decline in eGFR in patients on combination therapy than on a single agent alone, this combination is not generally recommended.23 If further agents are required, a diuretic or calcium channel blocker (preferably non-dihydropyridine calcium channel blocker) may be introduced.
The benefit of RAS inhibition on progression of proteinuria cannot be explained by the antihypertensive effects alone. Thus, current guidelines recommend that normotensive patients with microalbuminuria should also be treated with an ACEI.7
Referral to specialist team
In the UK, decision whether to refer to the local nephrology unit should depend on local guidelines developed by primary care, diabetic and renal services, but NICE has implemented guidelines suggesting that all diabetic patients with an eGFR above below 30 ml/min/1.73m2 should be referred for specialist review.7
Future directions
Earlier detection methods
Proteomic studies of urine and serum have been used to identify proteins which might enable earlier detection of the development of DN. One such protein, cystatin-C, is produced at a constant rate by all nucleated cells, is freely filtered by the glomerulus and shows promise as a biomarker for early DN.24
Direct renin inhibition
Aliskiren is a direct renin inhibitor so its potential role in the management of DN seems promising. Several trials have demonstrated its efficacy in reducing proteinuria independently of blood pressure.25 The longer-term benefits and its role in current treatment regimens are yet to be elucidated.
Pancreas transplantation
Pancreas transplantation may be considered a treatment for patients with life-threatening complications of diabetes (eg hypoglycaemic unawareness).
Pancreas-alone transplantation
There were 41 pancreas-alone transplants in the UK in 2010–2011.26 These patients provide a unique insight into the effects of renewed normoglycaemia on the complications of diabetes. Early reports indicate an improvement of DN at the histological level post-transplantation.27
Type 1 diabetes
The RA has now recommended that a simultaneous kidney-pancreas or living donor transplant be considered as first-line treatment for patients with type 1 diabetes and CKD stage 5.8
Conclusions
Diabetes is the commonest cause of CKD and end-stage renal disease in the developed word and is closely associated with other microvascular diabetic complications. To date, diagnosis focuses on the presence of microalbuminuria, but in the future there may be other, more sensitive detection methods. The mainstay of treatment involves blood pressure control with inhibition of the RAS and adequate glycaemic control, and the addition of lifestyle modifications when appropriate. There is a range of new promising directions in the field of diabetes with targeted therapies and transplantation.
- © 2012 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.