
Gastrointestinal (GI) cancers are common, comprising almost one-quarter of all cancers diagnosed in the UK annually.1 The most commonly encountered GI cancers are colorectal, oesophagogastric, pancreatic and hepatocellular carcinoma (HCC). Each tumour type demonstrates a distinct epidemiology, presentation, spectrum of clinical behaviour and requires a unique treatment approach, so they will be discussed separately.
Colorectal cancer
Colorectal cancer is the third most common cancer and the second leading cause of cancer death in the UK, accounting for 13% of new cancer cases annually. The incidence is strongly associated with age, rates increasing rapidly over the age of 50 with 72% diagnosed over the age of 65 years. Current lifetime risks for colorectal cancer in the UK are one in 15 and one in 19 for men and women respectively.1 The recent introduction of screening for colorectal cancer in the UK resulted in a temporary increase in incidence. However, following this, a trend towards earlier stage and less advanced disease has been observed in most pilot screening areas, with a corresponding decrease in colorectal-specific mortality.2 There is significant variation in colorectal cancer risk related to heterogeneity of epidemiological risk factors such as consumption of red meat, fibre and alcohol, and patterns of obesity and physical activity. Directly attributable genetic causes of colorectal cancer such as familial adenomatous polyposis and Lynch syndrome are responsible for a small number of cases (<5%), but less well-defined genetic syndromes may also play a significant role. Patients with multiple familial cases should also be considered for genetic referral and early colonoscopic screening programmes.3
Presentation
Colorectal cancer may present with a change in bowel habit, intestinal bleeding, abdominal pain, weight loss, obstructive symptoms or anaemia. Bright red blood per rectum is more commonly associated with left-sided tumours (rectum, sigmoid and descending colon), whereas right-sided tumours more commonly present with occult bleeding. Similarly, obstructive colon tumours more frequently occur in the left and sigmoid colon, whereas right-sided tumours are often more insidious in nature. Jaundice, hepatomegaly, ascites and pulmonary signs are indicative of advanced disease.
Investigation and staging
Clinical evaluation should include complete history (including family history) and physical examination, laboratory tests to include full blood count, electrolytes, liver function and carcinoembryonic antigen, in addition to full colonoscopy and computed tomography (CT) to evaluate for metastatic disease. Patients with rectal cancer should also undergo endoscopic ultrasound (EUS) or magnetic resonance imaging (MRI) for local evaluation of rectal staging prior to initiating therapy.
Colorectal cancer staging is performed according to the tumour, node, metastasis (TNM) classification of the American Joint Commission on Cancer staging system or, more commonly (but less comprehensively), according to the Dukes classification system:
Dukes A tumours are restricted to, but do not fully penetrate, the bowel wall
Dukes B penetrate the bowel wall
Dukes C demonstrate locoregional lymph nodal spread, and
Dukes D are associated with distant metastasis.
Management
Surgery. The type of surgical resection is dictated by the location of the lesion within the bowel. Stage I lesions (equivalent to Dukes A) are managed with resection only. Patients with locally advanced rectal cancer benefit from local downstaging with 5-fluorouracil (5-FU)-containing chemoradiation prior to surgical resection.4
Chemotherapy. Following resection, consideration should be given to adjuvant chemotherapy to decrease the risk of recurrence due to residual microscopic disease.
For fit stage III (node-positive) patients (equivalent to Dukes C), adjuvant chemotherapy is routinely offered in the form of a six-month course of fluoropyrimidines (oral or intravenous) plus or minus oxaliplatin.5,6 For patients with stage III disease, the absolute risk reduction with combination chemotherapy is 8–13% (the incremental benefit due to oxaliplatin representing about 3–4%). The survival advantage associated with adjuvant chemotherapy declines with age and reduced benefit is seen for the addition of oxaliplatin in those over 70 years.
The general risk of recurrence is much lower for stage II (Dukes B) tumours (15–20%), depending on T stage and other adverse prognostic factors such as emergency presentation, lymphovascular invasion and lymph node yield. Accordingly, the benefit from adjuvant chemotherapy is less for these patients (absolute benefit approximately 3.5% and no additional gain with oxaliplatin). Stage II patients who display mismatch repair deficiency do not appear to benefit from adjuvant 5-FU-based chemotherapy and it is recommended that this status is checked prior to initiating therapy in this patient group.
Metastatic colorectal cancer
Patients who present with metastatic colorectal cancer may benefit from metastatectomy and surgical resection with curative intent if metastases are limited in number and amenable to surgery. However, such patients are in the minority and most patients with stage IV disease (equivalent to Dukes D) are treated with palliative systemic chemotherapy. Patients fit to be treated with combination chemotherapy and novel biologic agents targeting angiogenesis (bevacizumab) or the epidermal growth factor receptor (cetuximab or panitumumab) have a median survival of almost two years, representing almost a doubling of overall survival in the past decade.7,8
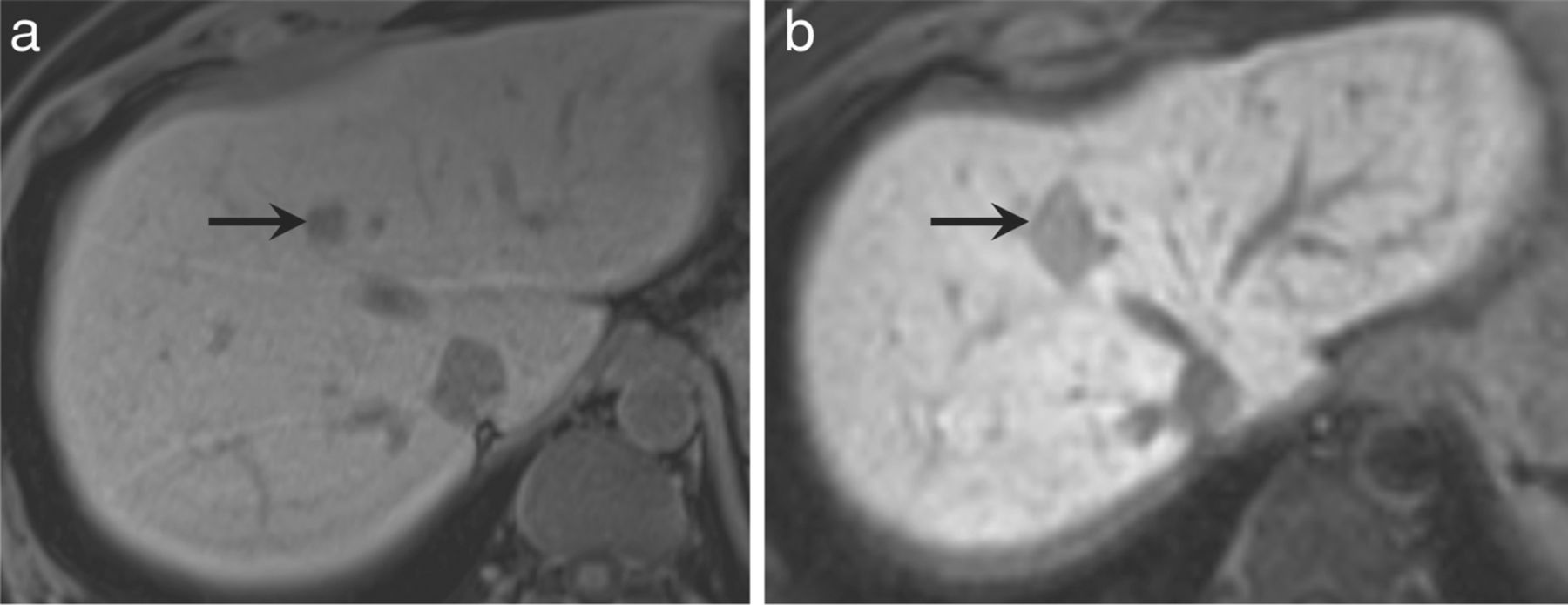
Additionally, local control of disease and chemotherapy-free intervals may be provided for selected patients with limited (usually single-organ) metastasis by non-surgical regional treatment approaches such as radiofrequency ablation (RFA) of lung and liver metastases or selective internal radiation therapy using yttrium microspheres injected into the hepatic arterial circulation (Fig 1).9,10

Radiofrequency ablation (RFA) of colorectal liver metastasis. Axial T1-weighted delayed post-contrast images: (a) pre- and (b) post-RFA of a solitary liver metastasis. The RFA lesion encompasses the entire metastasis with a margin to achieve adequate ablation. The RFA defect has a clearly demarcated low signal intensity rim due to the presence of haemosiderin. The central coagulative necrosis returns high signal intensity on T1-weighted images.
Oesophagogastric cancer
Oesophageal cancer
Oesophageal cancer, of which there are about 8,000 cases in the UK annually, comprises two distinct disease entities:
1. Squamous cell carcinoma (SCC) of the oesophagus commonly occurs proximally and is strongly associated with social deprivation, alcohol and tobacco use. Its incidence has declined significantly in recent decades.
2. Adenocarcinoma occurs most often in the distal third of the oesophagus and is associated with obesity, reflux and a history of Barrett's oesophagus. Incidence rates have increased dramatically in western countries in the past 30 years, with UK rates now amongst the highest globally.1
Investigation. Oesophageal SCC and adenocarcinoma frequently present in a common manner with dysphagia and weight loss, but distinct treatment approaches are required. Patients with localised disease should undergo investigation with CT to evaluate for metastatic spread prior to consideration of a radical treatment approach. EUS is valuable both to determine the extent of local invasion and to evaluate suspicious lymph nodes using fine-needle aspirate. Fluorodeoxyglucose-positron emission tomography scan may also be useful to detect occult metastases not seen on CT in up to 15% of adenocarcinoma patients (Fig 2).

Fluoro-deoxyglucose-positron emission tomography (a and c) demonstrates multiple bony metastases from oesophageal cancer not seen on computed tomography (b).
Management. Patients with SCC are treated with a combined platinum-based chemoradiation with curative intent. They may not require surgical resection if a complete pathological response is obtained at follow-up endoscopy.11,12
Adenocarcinoma is a less radiosensitive disease and more likely to be associated with occult distant metastatic spread. These patients appear to benefit less from a localised chemoradiotherapy approach. In the UK, most of them undergo pre-operative chemotherapy followed by surgical resection.14 Oesophagogastrectomy may be associated with significant complications and mortality in addition to substantial postoperative morbidity. Thus, surgery should be performed only on fit patients at high-volume surgical centres with appropriate expertise in order to minimise these risks.
Gastric cancer
Gastric cancer occurs in almost 8,000 patients per year in the UK. Adenocarcinoma of the cardia (upper third) of the stomach shares a common aetiology and incidence with adenocarcinoma of the distal oesophagus. Distal (antral) gastric cancers (which have decreased in incidence) are associated with Helicobacter pylori infection and dietary factors such as high intake of preserved or smoked foods and low intake of fruit and vegetables.
Investigation and staging. Staging of patients with gastric cancer is similar to that for oesophageal cancer, with the addition of pre-operative laparoscopy to detect occult peritoneal metastases prior to initiating treatment with curative intent.
Management. In the UK and Europe, fit patients with localised disease are treated with three cycles of cisplatin-based pre-operative chemotherapy and further cycles in the postoperative setting – an approach that has increased three-year survival from 23% to 36% compared with surgery alone.13 In the US, postoperative chemoradiation is commonly employed but, given the morbidity associated with gastrectomy, fewer patients are suitable for this approach.
Unfortunately, most patients in the UK presenting with oesophagogastric cancer have advanced disease not amenable to surgical resection. Fit patients with metastatic or unresectable disease are treated with combination cisplatin-based chemotherapy, most often epirubicin, cisplatin and capecitabine (EOX), and have a median overall survival of 9–11 months.14 The addition of the anti-HER2 monoclonal antibody trastuzumab to chemotherapy for the approximately 20% of patients who overexpress the HER2 protein has led to significant increases in survival for this population.15 Symptomatic control of dysphagia using oesophageal stents also remains a useful treatment option.
Pancreatic cancer
Cancer of the pancreas is diagnosed in over 8,000 patients per year in the UK and remains one of the most lethal malignancies, with overall five-year survival below 5%.1 These poor survival outcomes reflect both the infiltrative nature of the disease, which is frequently unresectable or metastatic at presentation (only 10–15% of patients are operable), and the underlying chemorefractory status of the tumour. Patients may present with weight loss, abdominal or back pain, or painless obstructive jaundice which may be relieved by biliary stent placement.
Key points
Colorectal cancer is the third most common cancer in the UK and the second leading cause of cancer death. Recently initiated screening programmes demonstrate early signs of decrease in colorectal cancer-specific mortality
Survival for patients with metastatic colorectal cancer treated with cytotoxic chemotherapy and biologic agents now extends up to two years (almost doubled in the last decade)
Careful patient selection and centralisation of surgery in high-volume centres are essential to optimise surgical outcomes for patients undergoing oesophagogastrectomy. Neoadjuvant, peri-operative or postoperative treatment increases survival for patients with operable gastro-oesophageal cancer
Early involvement of palliative care services for patients with metastatic pancreatic cancer is advised in order to improve both symptom control and quality of life
Patients with unresectable or metastatic hepatocellular carcinoma with preserved liver function may benefit from treatment with the oral anti-angiogenic agent sorafenib
Investigation
Specialised pancreatic protocol CTs are necessary to delineate the anatomy of the coeliac axis in order to determine resectability.
Management
Patients with operable disease are treated with postoperative adjuvant gemcitabine chemotherapy, leading to median survival of 23 months.16 Patients with locally advanced unresectable non-metastatic pancreatic cancer are treated with combination chemotherapy, possibly followed by chemoradiation. Those with metastatic disease are treated with chemotherapy alone.17 Their survival with current combination chemotherapy regimens ranges from 6–12 months.18,19 Because of issues surrounding symptom control and nutrition, early interaction with palliative care services is advised for these patients.
Hepatocellular carcinoma
Although rates of HCC remain low overall in the UK (about 4,000 cases per year), the incidence has trebled in the past 30 years. Risk factors include hepatitis B and C infection, high alcohol intake, smoking, obesity, diabetes, haemochromatosis and non-alcoholic steatohepatitis. Presentation is frequently non-specific, with abdominal pain, fullness, weight loss and anorexia, or an abdominal mass. Signs of chronic liver disease may also be present.
Treatment of gastrointestinal cancers.
Investigation
Assessment of liver function is a key component in the evaluation of the patient with HCC as this will impact significantly on treatment choices. Serum alpha-fetoprotein is also a useful marker in over half of patients. Triphasic CT, gadolinium-enhanced MRI and ultrasound may all be used to assess resectability.
Management
Partial hepatic resection may be performed for patients with solitary lesions, no evidence of vascular invasion or portal hypertension, and adequate hepatic function. Given the risk of tumour seeding, no biopsy should be taken provided that the tumour meets radiologic criteria for diagnosis.
If resection is not possible, or the patient has compromised liver function but meets the Milan criteria for transplant (a solitary lesion <5 cm or up to three lesions with none >3 cm in size, with no evidence of vascular invasion or regional or distant metastases), orthotopic liver transplantation may be performed.
Local ablation methods such as RFA or transarterial chemoembolisation may be considered for patients who do not meet resection or transplant criteria but only have hepatic disease.
Until recently, treatment options for patients presenting with or developing metastatic disease were extremely limited as HCC does not display chemosensitivity. However, the oral anti-angiogenic tyrosine kinase inhibitor sorafenib has improved median overall survival to almost one year (survival on sorafenib is three months longer than on placebo), but is suitable only for patients with relatively preserved liver function.20
- © 2012 Royal College of Physicians
References








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.