
What lies beneath the surface?
This reports describes the development of a rash in a 43-year-old man with asthma, who was admitted to the respiratory clinic with dyspnoea, leucocytosis and a productive cough. His symptoms progressed and he was admitted to the high-dependency unit for respiratory support. The incisional biopsy taken from his rash was paramount in the diagnosis of systemic vasculitis. Of equal importance was recognition of eosinophilia and pneumonitis in this young man and initiation of immunosuppressive therapy. The key message from this particular case was the importance of early diagnosis of Churg-Strauss syndrome, in which a rash is combined with marked peripheral eosinophilia and signs of respiratory distress. Early intervention will reduce the risks of morbidity and mortality in patients with this rare, life-threatening syndrome.
Lesson
A 43-year-old, male, heavy goods vehicle (HGV) driver was referred to the dermatology clinic from the accident and emergency department with a five-day history of a widespread, itchy, maculopapular, erythematous rash. Previously fit and well other than a recent diagnosis of asthma, he had developed a generalised illness, with symptoms including lethargy, myalgia, loose motions, decreased appetite and coryzal symptoms two weeks prior to presentation. The asymmetrical, diffuse, itchy exanthem had initially involved only the legs but later spread to the abdomen, groin and upper limbs. The illness was associated with a cough productive of green sputum and disproportionate breathlessness. The patient had no history of recent tropical travel, no environmental exposure to hazardous environmental agents at work, no relevant sexual history and no recent dietary changes and he took no regular medications. He had no relevant family history and had stopped his 25-a-day smoking habit at the onset of his illness.
On examination, the patient was apyrexial and had a slightly scaly maculopapular rash on the abdomen and limbs, with some areas of confluence (Figs 1 and 2). The rash was initially felt to be in keeping with a diagnosis of erythema multiforme or to be related to an over-the-counter medication the patient had taken for his flu-like symptoms. An incisional biopsy was taken and he was then referred to the medical team at the Countess of Chester Hospital in view of his extreme dyspnoea. By this time he was hypoxic (oxygen saturation 87%), his respiratory rate was 18 breaths per minute and auscultation of his chest revealed right-sided coarse crepitations.

Trunk showing vasculitic rash, including biopsy site.

Left lower limb demonstrating cutaneous vasculitis.
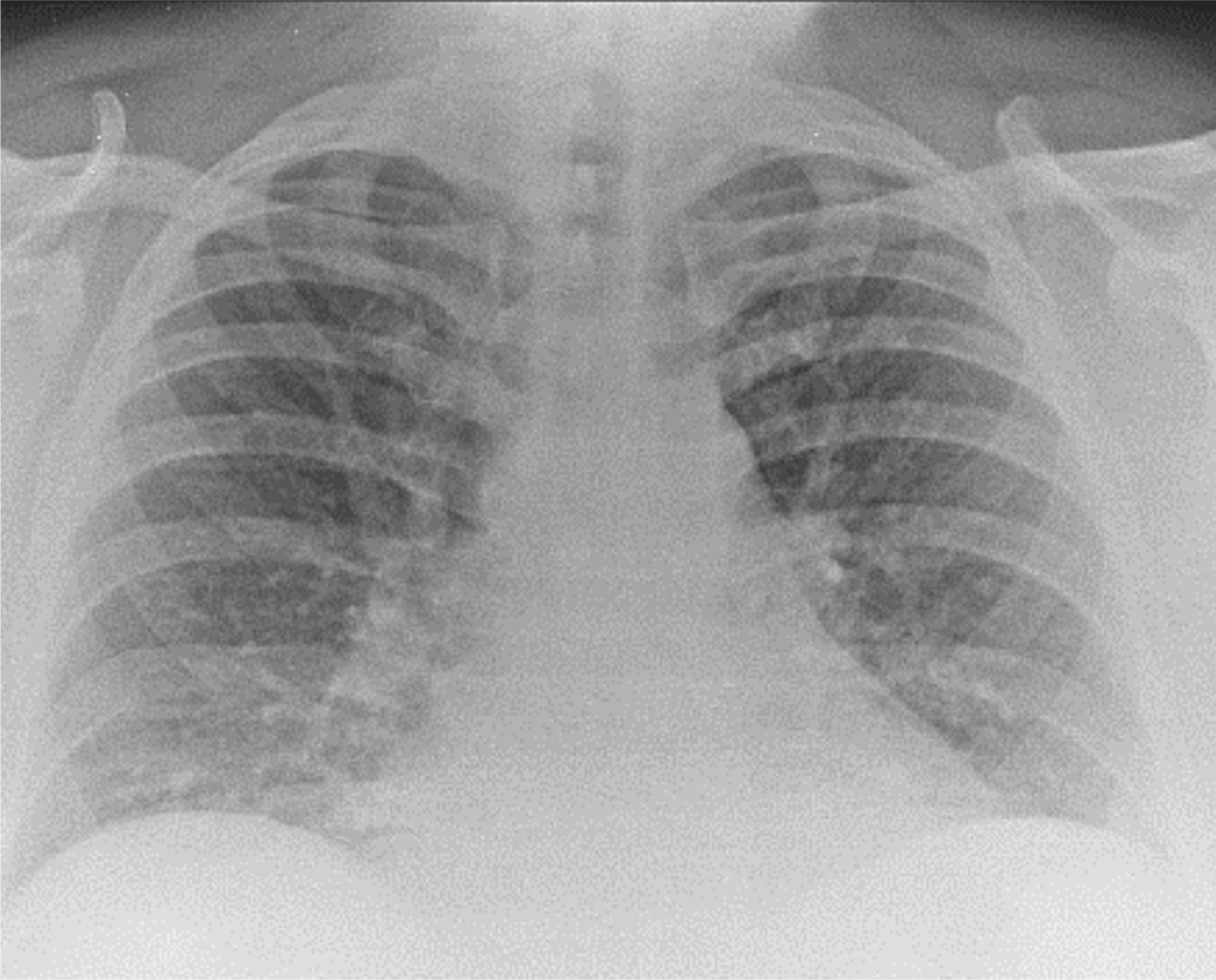
Investigations revealed marked neutrophilia (15.6), marked eosinophilia (7.7×109/l), mild hyponatraemia, transaminitis and erthryocyte sedimentation rate (ESR) of 32 mm/hr. Renal function remained stable throughout. His chest X-ray showed widespread shadowing of the right middle and lower lobe (Fig 3). Arterial blood gas (ABG) measurement (8.9 kPa) confirmed type 1 respiratory failure, with oxygen partial pressure (pO2) of 8.9 on 60% oxygen. An urgent echocardiogram showed good left ventricular function, no evidence of a massive pulmonary embolism and no pericardial effusion. At this time, the patient's rash worsened and he showed signs of respiratory distress. Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, triggered by the shop-bought flu medication, was ventured as a possible diagnosis at this time in view of the accompanying eosinophilia.

Plain chest radiograph showing bilateral interstitial opacification and right-sided hilar lymphadenopathy.
A computed tomography scan of the chest showed evidence of pneumonitis (Fig 4), which, together with the peripheral eosinophilia and rash, raised the possibility of systemic vasculitis. This led to initiation of immunosuppressive therapy involving intravenous methylprenisolone by the on-call respiratory consultant.
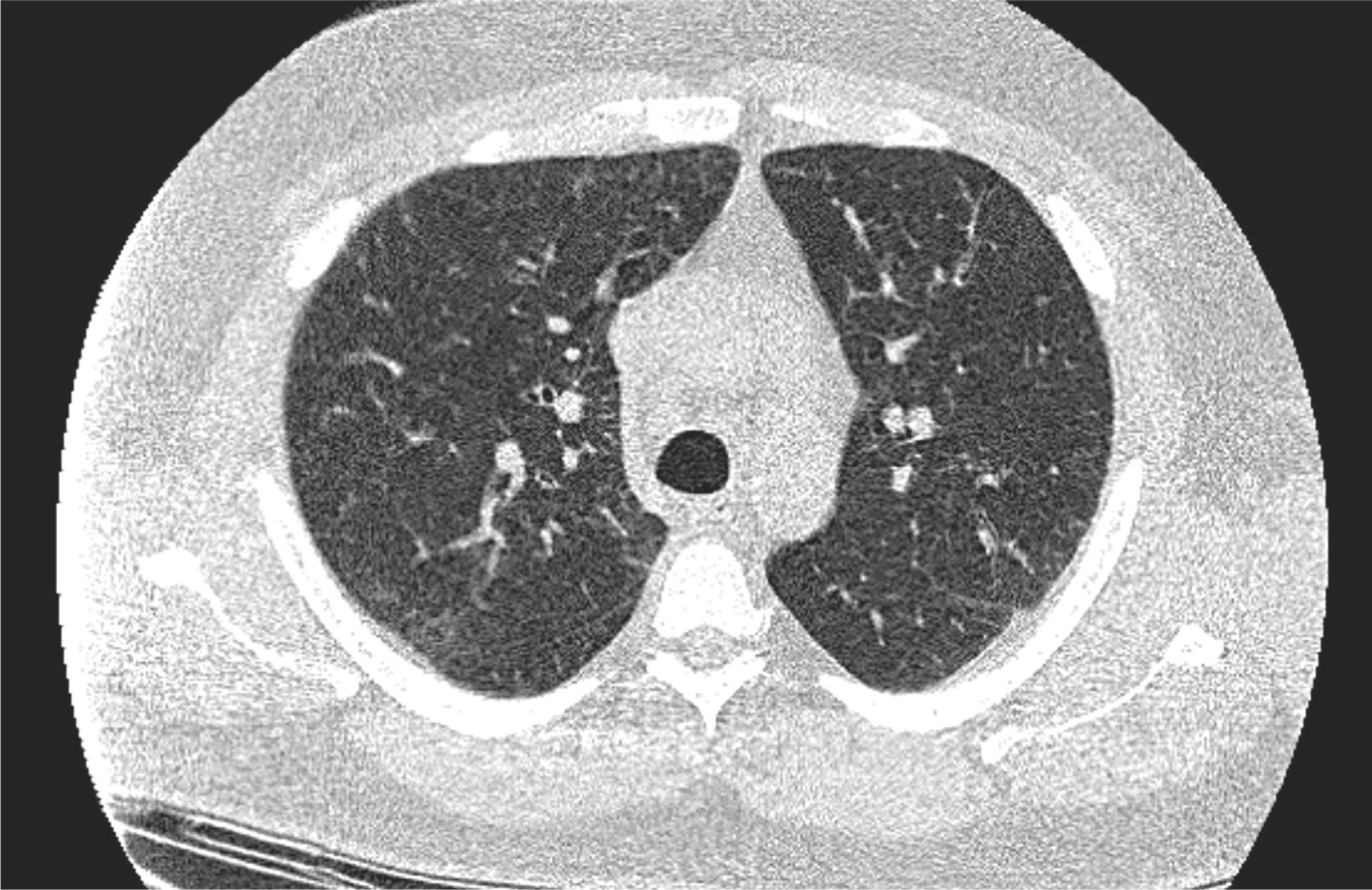
Computed tomography scan of chest showing glass-ground shadowing and increased interstitial opacification consistent with pneumonitis.
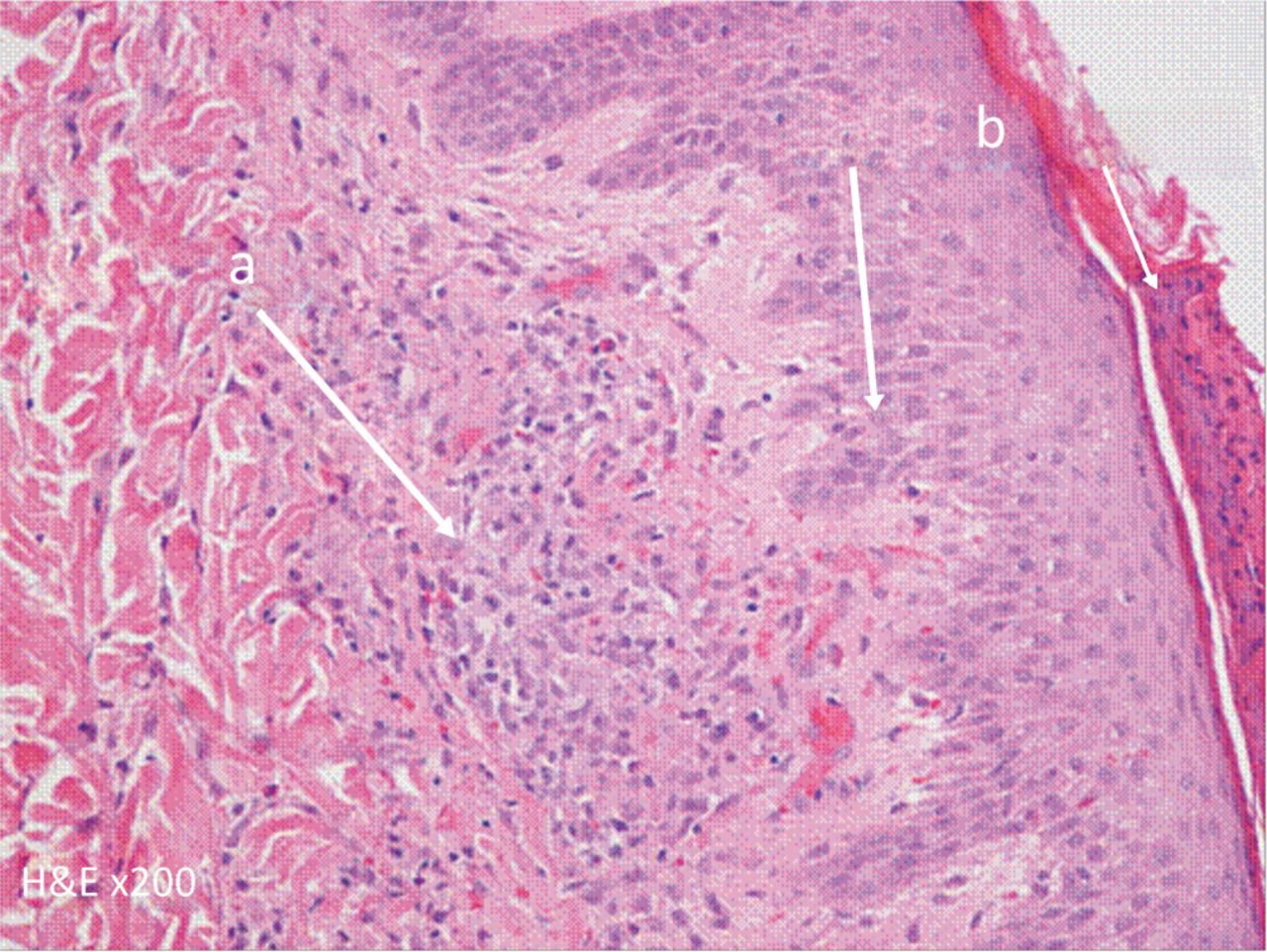
After the patient was transferred to the critical care environment, his incisional biopsy result, which showed evidence of a vasculitic process (Fig 5), became available. Histologically, the skin lesions showed a range of changes from focal areas of collagen degeneration with an associated mixed inflammatory cell infiltrate to more-established lesions with granulomatous inflammation and an accompanying eosinophilic infiltrate. These features were in keeping with both Wegener's granulomatosis and Churg-Strauss syndrome. At this stage, cyclophosphamide was added to the intravenous methylprednisolone regimen. However, the patient's autoimmune screen was, in fact, negative. The diagnosis of Churg-Strauss syndrome was made by the rheumatologists on the basis of eosinophilia, asthma, histological confirmation of vasculitis and the presence of pulmonary infiltrates on imaging. The patient was discharged on a reducing regimen of prednisolone.
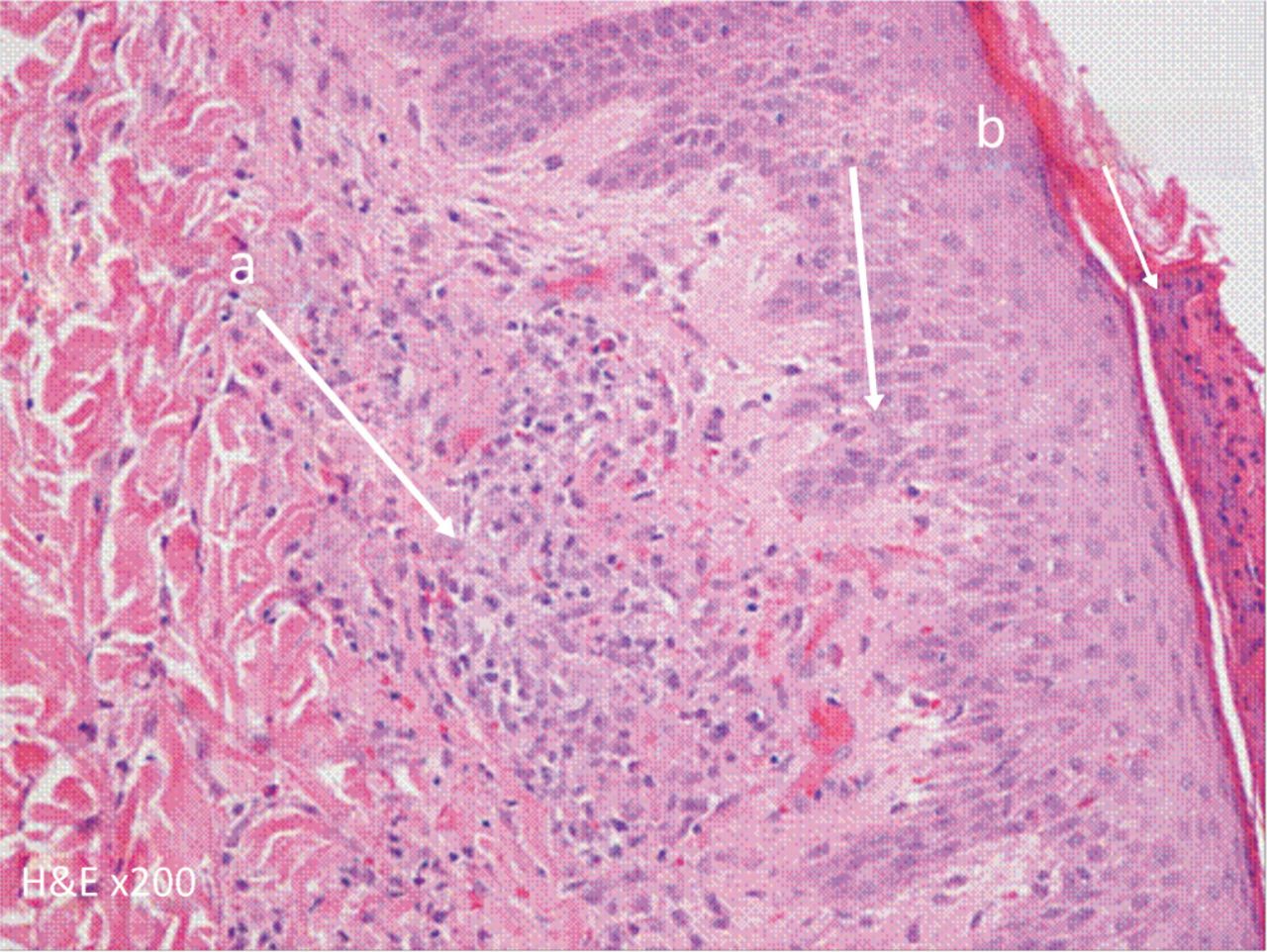
Histological appearance of cutaneous vasculitis from skin biopsy. a = granulomatous inflammatory infiltrate; b = epidermis showing some sporidiosis with parakeratosis.
Discussion
Churg-Strauss syndrome, otherwise known as allergic granulomatous angiitis, is a vasculitis involving small- and medium-sized vessels. Churg and Strauss described the condition in 1951 after identifying 13 patients with asthma, eosinophilia, necrotising vasculitis and glomerulonephritis.1 It is the least common of the three main presenting anti-neutrophil cytoplasmic antibody (ANCA)-positive vasculitides, presents equally in both sexes and is rare after the age of 65 years.2 This multisystem disorder is characterised by chronic rhinosinusitis, asthma and marked eosinophilia. Pulmonary involvement is most common, but it can also affect the renal system, upper airways and skin.3–4
Churg-Strauss syndrome seems to have three stages: prodromal, eosinophilic and vasculitic.5 The prodromal phase tends to feature atopic disease in the second decade, while the eosinophilic phase presents as asthma and marked eosinophilia in the third decade. Indeed, asthma is the cardinal feature, occurring in 95% of patients and on average 8–10 years ahead of the vasculitic phase.5 The final vasculitic phase tends to be associated with extrapulmonary signs in middle age, with fever, weight loss and lethargy.5 The official diagnosis is based on satisfying four of the American College of Rheumatology's criteria (Box 1).6
American College of Rheumatology 1990 criteria for the classification of Churg-Strauss syndrome.7
Autoimmunity is the key driver in Churg-Strauss syndrome, which is demonstrated by increased levels of eosinophils, ANCA and immunoglobulin E, but the exact pathophysiology remains unknown.7 The most common treatment is glucocorticoid therapy, with the addition of cyclophosphamide in patients with major, life-threatening, multiorgan involvement. These drugs can later be converted to steroid-sparing agents such as azathioprine, mycophenolate mofetil and methotrexate.8
Although Churg-Strauss syndrome is a rare diagnosis, with an incidence of 2.5 in 100,000 in the UK, the consequences of missing a diagnosis can be fatal, as survival without treatment after five years is 25%.7 This case acts as reminder of the importance of tissue biopsy in confirming the diagnosis of syndrome, the need for a multidisciplinary team approach in achieving diagnosis, the polymorphic nature of the associated rash and the subsequent broad range of differentials.
Achieving diagnosis in this case was not straightforward: it is the least common form of systemic vasculitides, and cutaneous vasculitis can take a number of forms, so the changes seen in the skin biopsies histologically could only be suggestive of rather than diagnostic for the syndrome. Erythema multiforme and rashes related to drug hypersensitivity are far more common and share a number of features with the vasculitic rashes, in addition to associations with internal manifestations. In the acute vasculitic phase, the destruction of leucocytes results in petechiae and purpura, with necrosis in severe cases. Subacute vasculitis results in erythematous macules and papules, at times resembling urticaria, which are located symmetrically on the extremities and scalp. Chronic vasculitis tends to be a macular erythematous patchy exanthem.
The main manifestations of DRESS syndrome are fever, a morbilliform rash, lymphadenopathy and internal organ involvement, with marked eosinophilia. The most frequently involved organ is the liver, followed by the kidney and lungs. The morbilliform drug eruption usually appears first on the trunk and then spreads to the limbs and neck. The exanthem consists of widespread pink macules and papules in annular or urticarial formations. The spots may cluster and merge to form sheets over several days, sometimes involving the entire skin surface. A drug hypersensitivity syndrome can occur up to eight weeks after first exposure to the drug responsible.
Erythema multiforme is a hypersensitivity reaction usually triggered by infections or drugs. The eruption is polymorphous, developing as sharply demarcated erythematous macules that become papular and then coalesce to form plaques up to several centimetres in diameter. Lesions usually evolve over 72 hours, with target formation followed by blistering. The mucous membrane may be involved. Erythema multiforme is acute and self-limiting, usually resolving without complications.
The key message from this particular case was the importance of early diagnosis when a rash is combined with marked peripheral eosinophilia and respiratory distress. Other learning points include the polymorphic nature of the rash, which highlights the importance of tissue diagnosis, the misconception that ANCA must be positive for diagnosis of systemic vasculitis (in fact, data show that only 38% of cases of Churg-Strauss syndrome are positive ANCA)9 and recognition that the entity is dependent on a good clinical history, as the changes seen in skin biopsies are not diagnostic. Careful clinicopathological and serological correlation are therefore essential to come to the correct diagnosis, which necessitates a multidisciplinary team approach.
- © 2013 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.