
Introduction
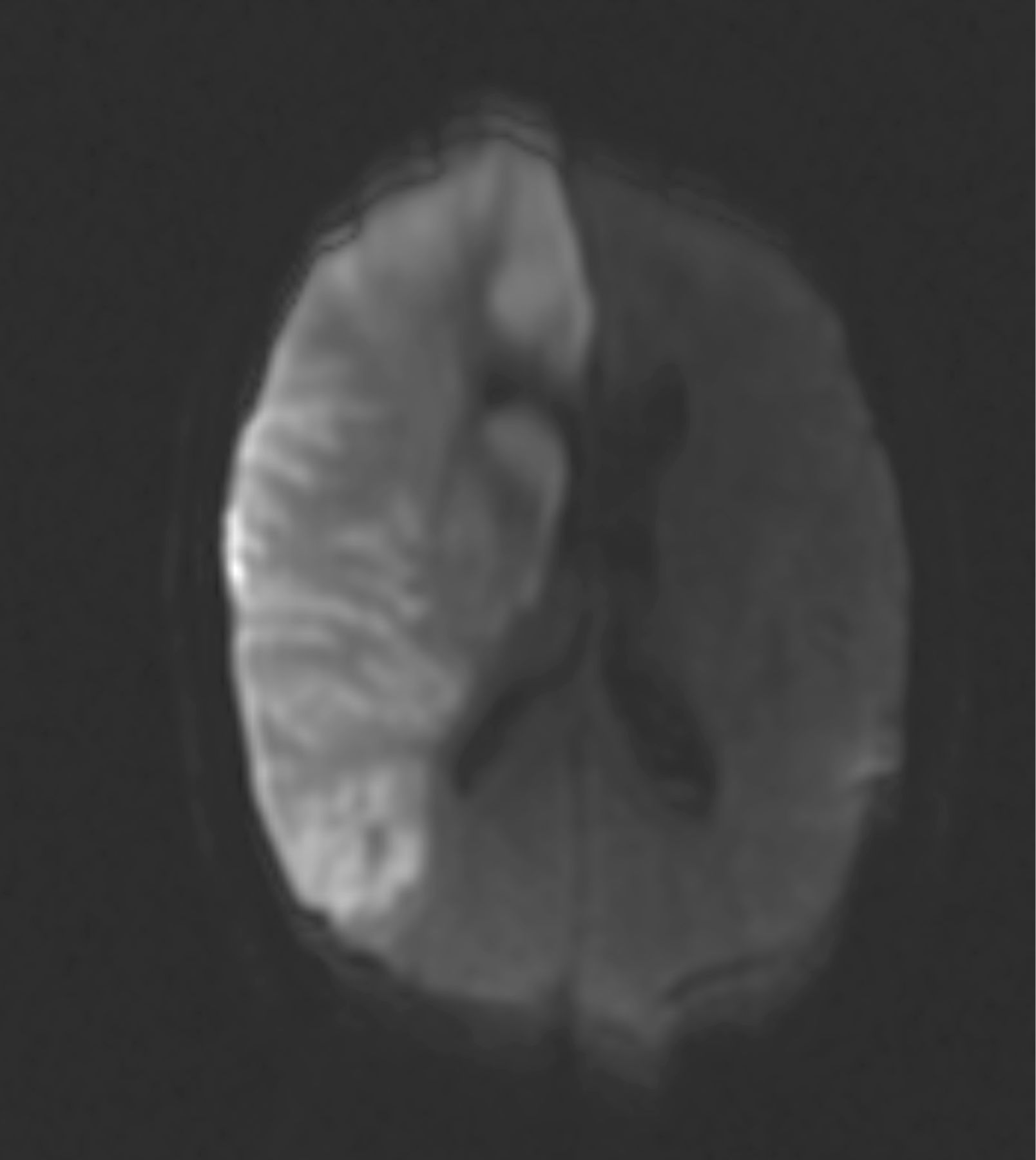
A 53-year-old woman, who had previously been fit and well, presented to the emergency department (ED) with headache, loss of consciousness and left hemiplegia of sudden onset. Her past medical history included neurosurgery for a left temporo-occipital cavernoma four years previously and a separate incidence of ‘labyrinthitis’. Cardiovascular examination did not reveal any abnormalities. The patient underwent routine investigations, including an electrocardiogram (ECG), blood tests, a computerised tomographic (CT) scan of head and a magnetic resonance (MR) scan of head (Fig 1). The latter showed a large cerebral infarct. The patient was found to be in sinus rhythm; 24-hour Holter monitoring and carotid duplex scan were also normal. On further questioning, there was a history of weight loss and night sweats.
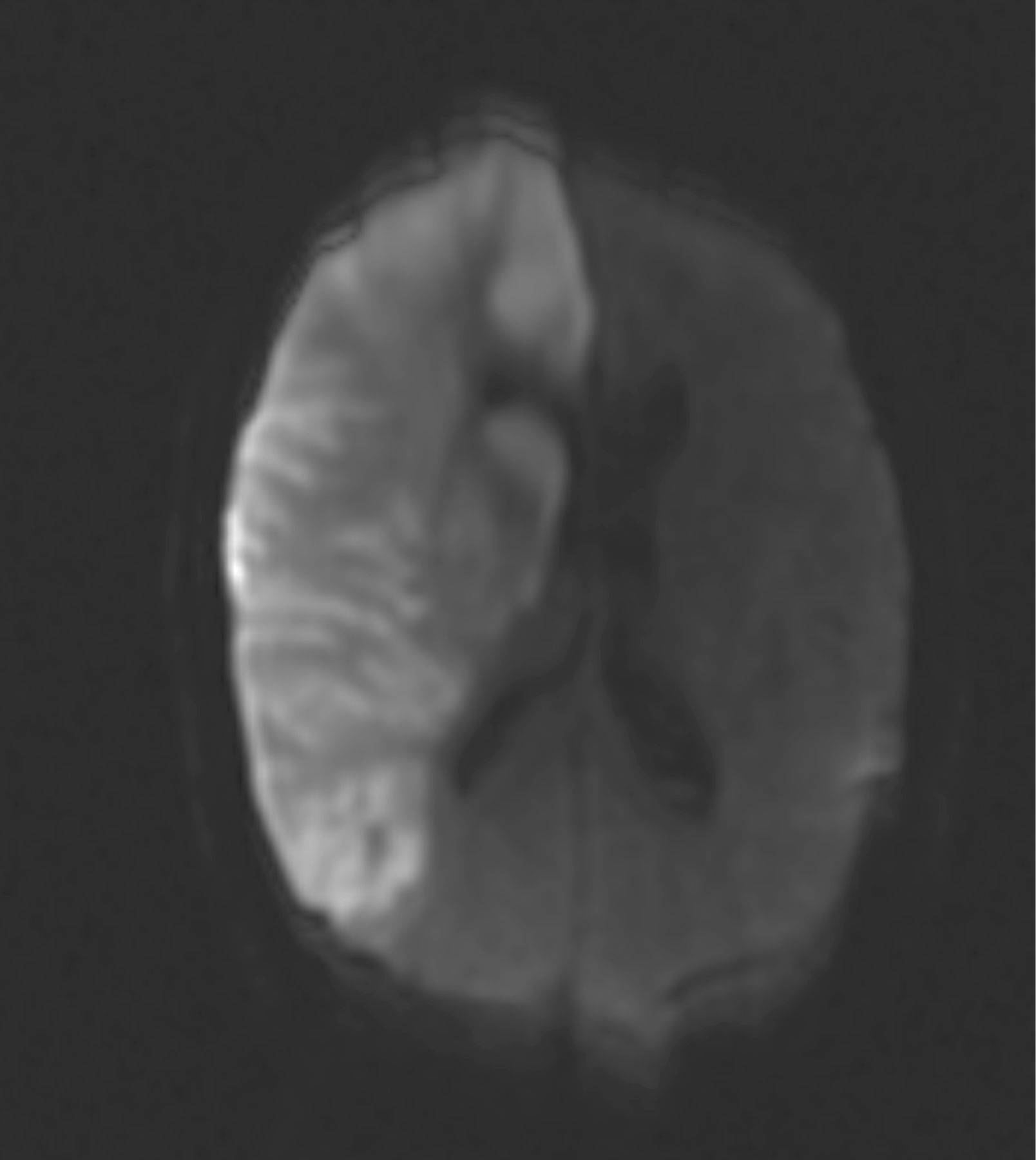
Magnetic resonance axial diffusion-weighted scan of head.
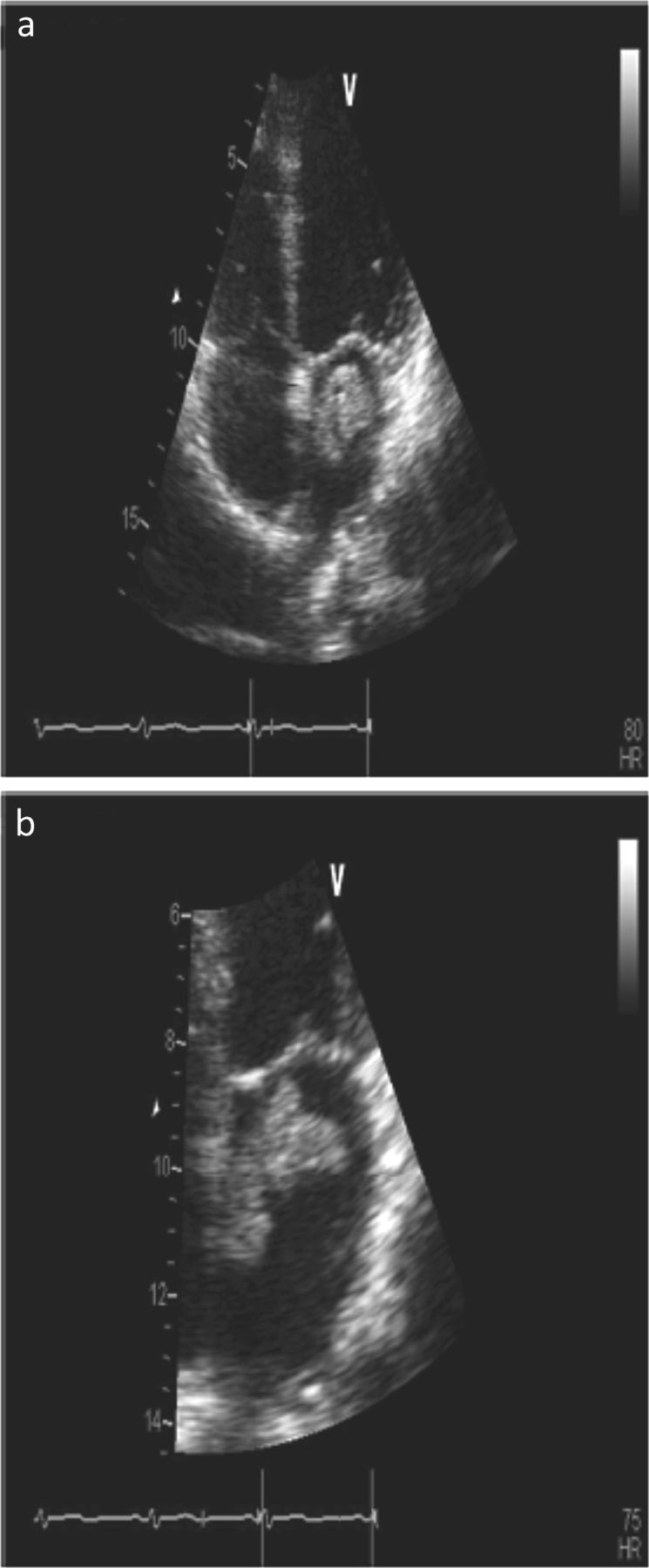
A cardioembolic cause for the cerebral infarct was suspected and consequently confirmed by a transthoracic echocardiogram (TTE). The TTE demonstrated a large, mobile echodense mass within the left atrium (LA) (Fig 2). The irregular and frond-like mass, resembling a cluster of grapes, appeared to be attached to the fossa ovalis. Its appearance was considered to be consistent with a LA myxoma. Thrombolysis was not attempted and the patient was unfit for cardiac surgery. Despite cranial decompression on day two, the patient died 35 days after presentation.

Transthoracic echocardiogram. (a) Apical four-chamber view; (b) left atrial-focused view.
The MR image in Fig 1 demonstrates right frontoparietal lobe intensity, indicating acute infarction of territory of the right middle and right anterior cerebral arteries.
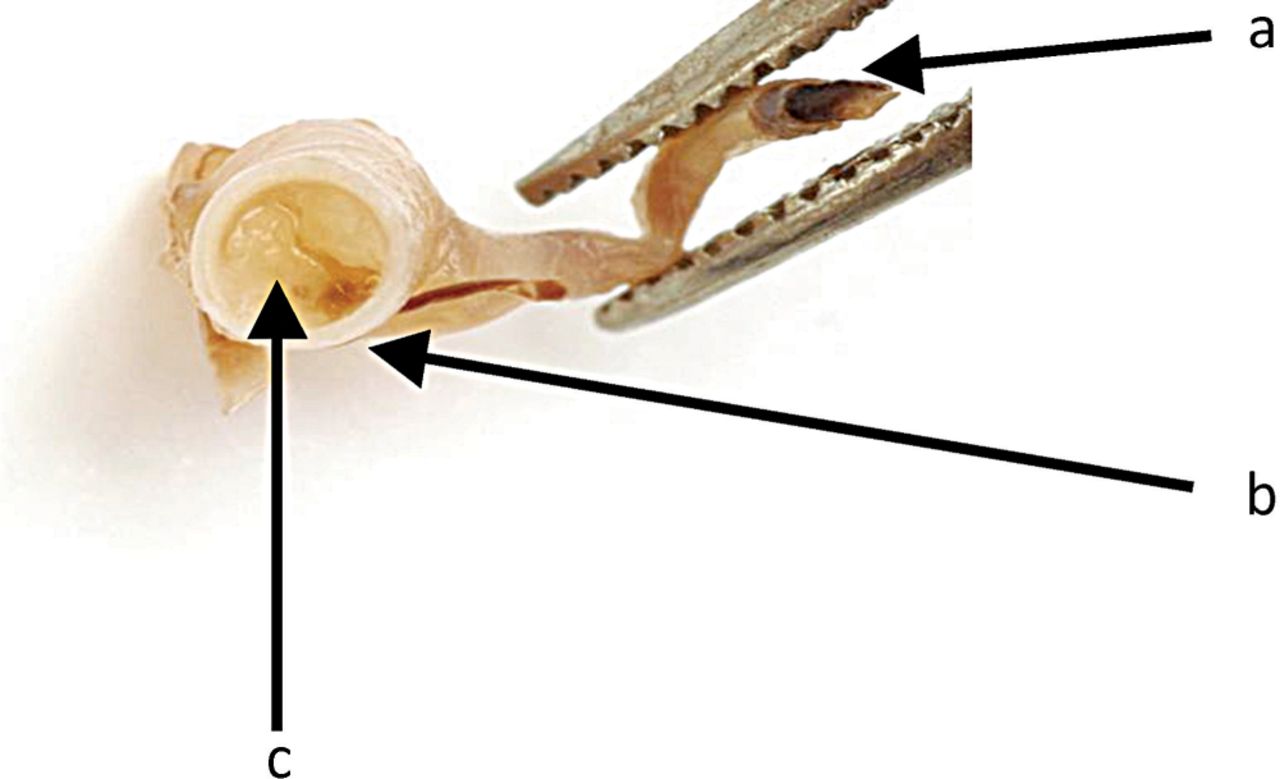
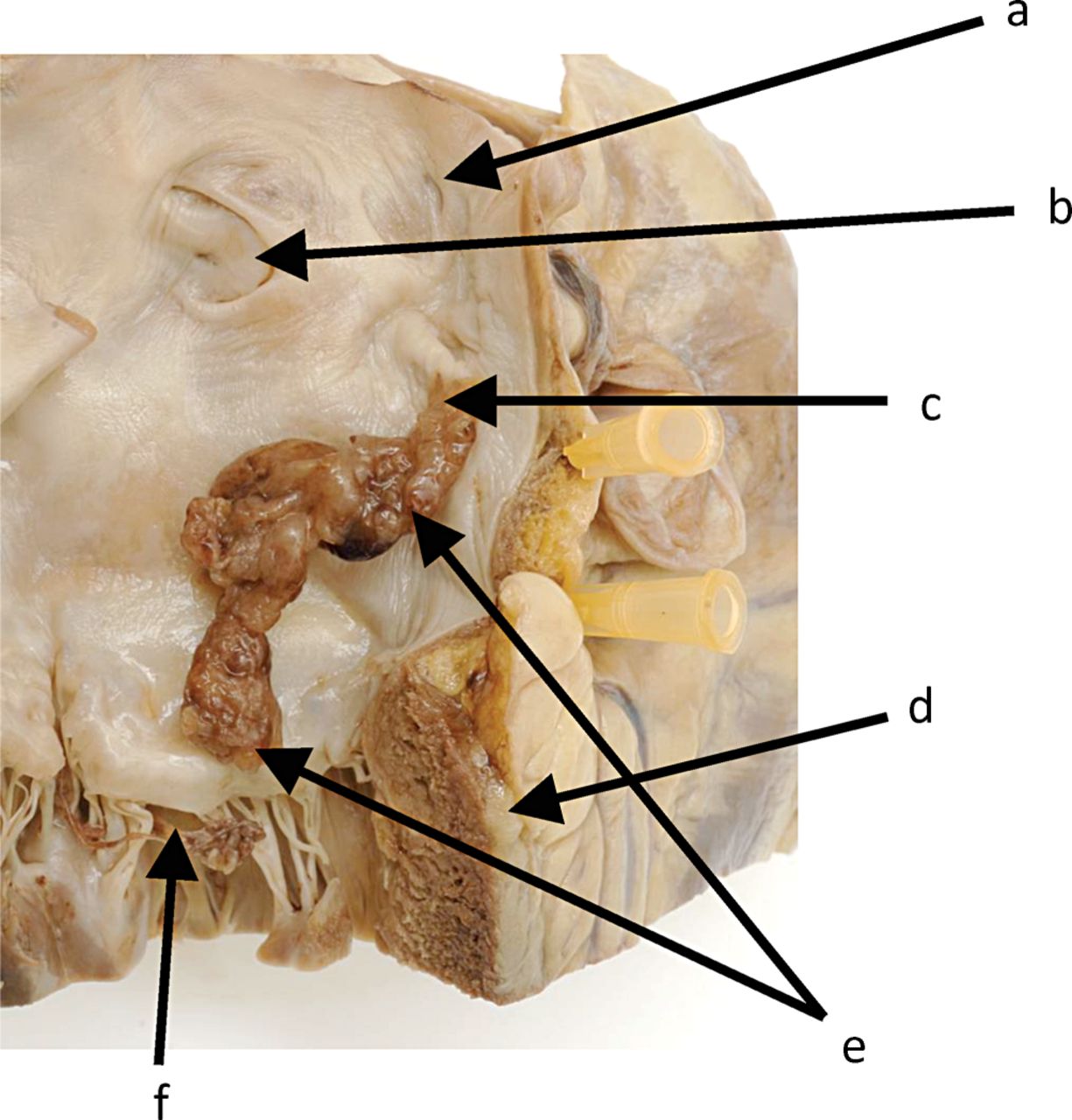
A consented hospital post-mortem was performed and showed that the immediate cause of death was bronchopneumonia following a massive right anterior cerebral artery territory infarct. The distal right internal carotid artery and its branches were all occluded by a tumour embolus typical of an embolic myxoma (Fig 3). Acute infarcts were seen in kidneys, spleen and liver, and an old infarct was seen in the myocardium. An old right cystic cerebellar infarct was also confirmed. The LA contained a tan-coloured, elongated, lobulated mass 25-mm long and 8 mm in maximum diameter (Figs 4 and 5). It was firmly attached to the interatrial septum just posterior to the closed fossa ovalis and extended to the orifice of the mitral valve. Histology of both the cardiac mass and the tumour embolus in the right internal carotid artery was identical. Immunohistochemistry for calretinin was positive in both cardiac and arterial samples confirming that this was an atrial myxoma. Myxoid sarcomas (myxoid imitators) and organised thrombus were excluded. Although thrombus was present in both cardiac and cerebral artery lesions, it was not significant in amount.
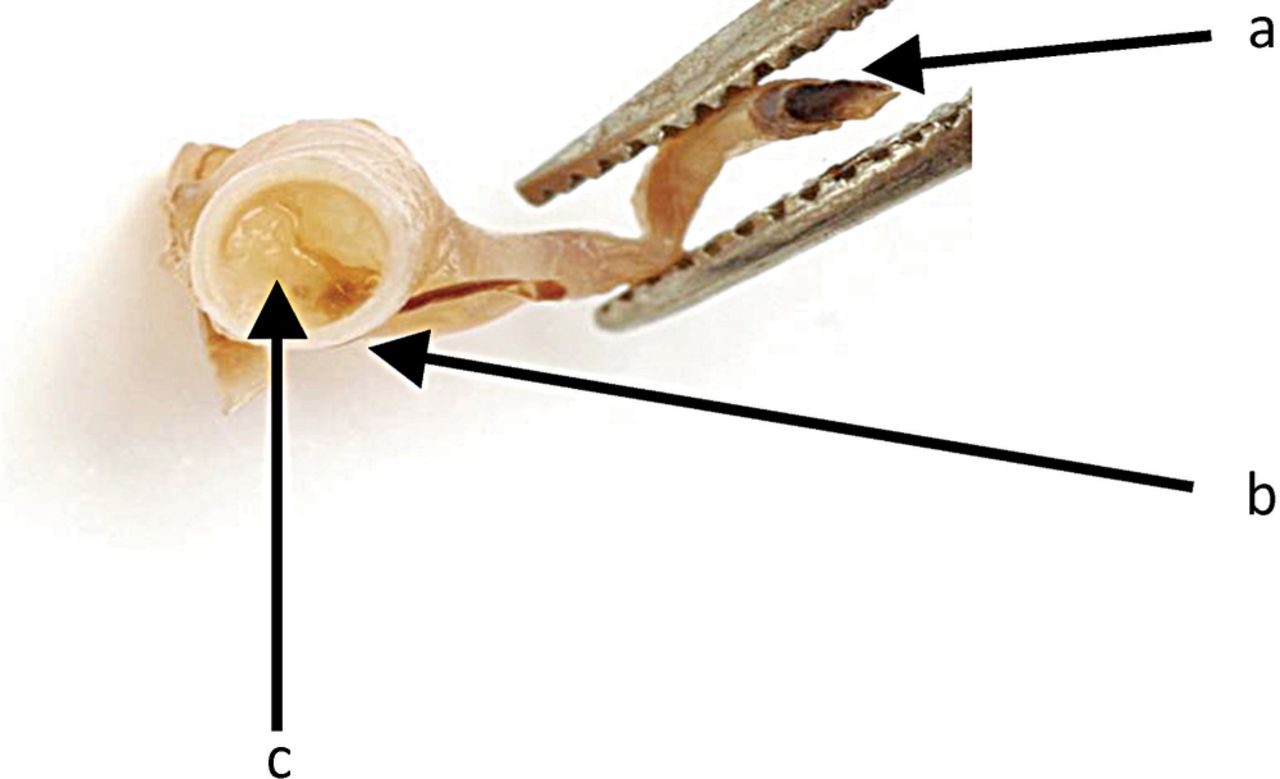
Right internal carotid artery occluded by embolic myxoma from left atrium. a = right anterior cerebral artery; b = right internal carotid artery; c = embolic myxoma.
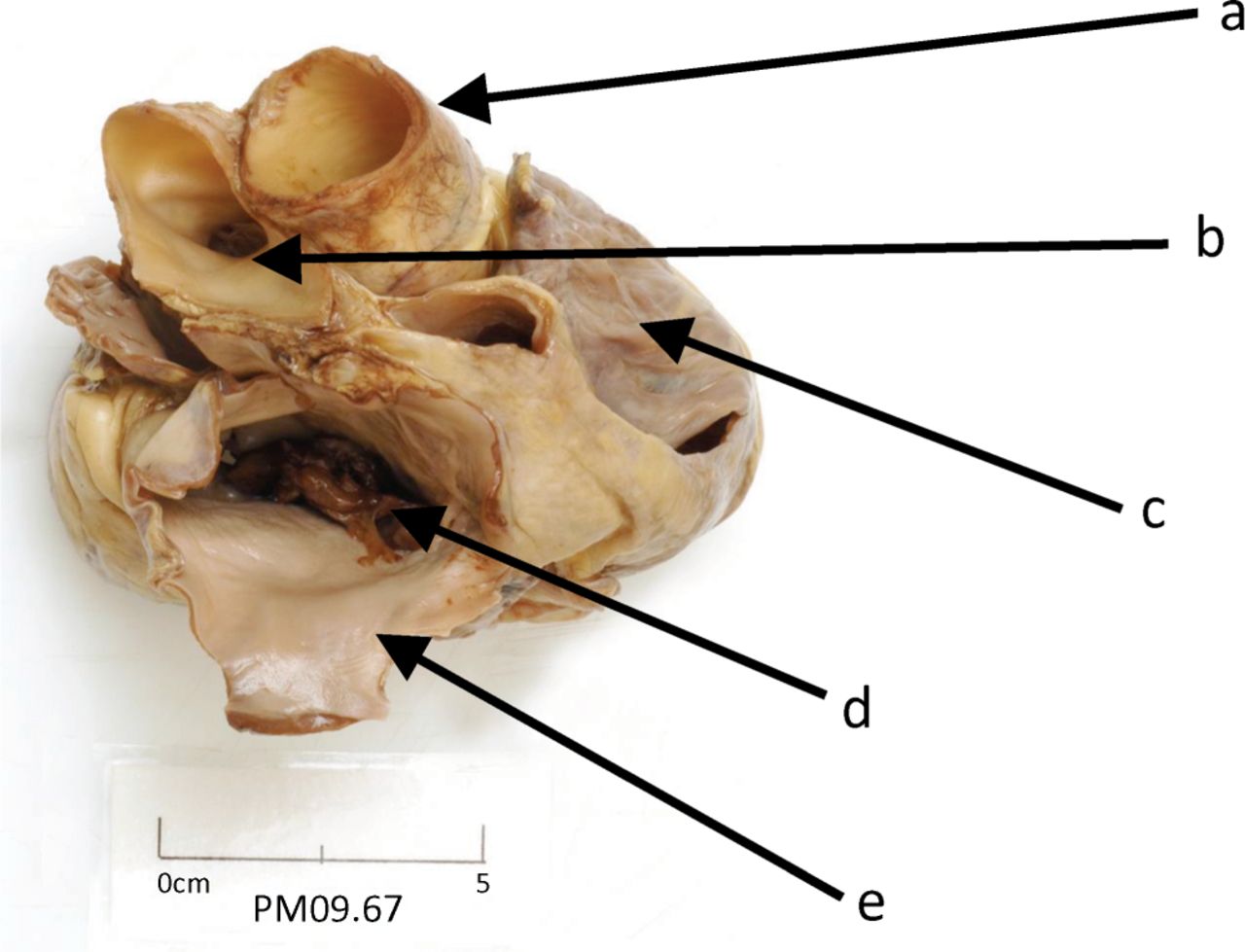
Superior view of heart. a = aortic root; b = pulmonary trunk; c = right atrium; d = tumour and post-mortem clot; e = left atrium.

Left atrium and upper left ventricle. a = left atrial wall; b = fossa ovalis; c = point of attachment of myoxma to the posterior interatrial wall posterior to fossa ovalis; d = upper posterior left ventricle wall; e = myxoma polypoid free-floating tumour; f = mitral valve posterior cusp.
Cardiac source of embolism
The causes of stroke can be classified into two major categories, with approximately 85% being ischaemic and the remaining 15% being haemorrhagic.1 Of those ischaemic strokes, embolism from a cardiac source accounts for approximately 20% and is shown to carry a poorer outcome compared with other causes of stroke. Echocardiography is indicated in the setting of a suspected cardiac mechanism for stroke or related symptoms of syncope and transient ischaemic attack (TIA). In this regard, echocardiography has a pivotal role in determining cardiac sources. Causes of cardiac sources of embolism are summarised in Table 1, and are categorised according to embolic risk; high, low and/or undetermined.
Causes of cardiac source of embolism.
Cardiac masses seen on echocardiography can be broadly classified into one of three categories: tumour, thrombus or vegetation. Cardiac tumours can be primary or secondary, benign or malignant and arise from the heart (primary) or be deposited in the heart from a remote primary (metastasis). They can present with embolic events and stroke, which might be the first indication of their presence, as illustrated by our case. The most common tumours associated with embolic stroke are cardiac myxomas and papillary fibroelastomas of the cardiac valves.
Myxomas
Although sporadic cardiac myxomas present more often in middle-aged (30–70 years) females (male:female ratio is 1:3), 7% are familial and associated with Carney complex. Cardiac myxomas are benign intrinsic neoplasms possibly arising from intracardiac sensory nerve ganglia, which are also calretinin positive.2 Such myxomas are the most common primary neoplasm of the heart, representing approximately 30–50% of all primary cardiac neoplasms, although metastatic (secondary) malignant neoplasms are more frequent. Most (90%) are found in the LA and are pedunculated, arising from the fossa ovalis. Other sites include the right atrium (approximately 18%), left ventricle (approximately 4%) and right ventricle (approximately 4%), although myxomas can occur at multiple sites simultaneously.3 Cardiac myxomas cause constitutional symptoms (paraneoplastic reactions), including malaise, arthralgia, pyrexia of unknown origin, night sweats, anorexia and cachexia, and can lead to haemolytic anaemia, dysglobulinaemia and thrombocytopenia. Cardiac presentations include cardiac failure and syncope. If the tumour mass causes significant mitral valve obstruction, then clinical signs of mitral stenosis might be present, including a typical early low-pitched diastolic murmur known as a ‘tumour plop’ on auscultation.3 Occasionally, they might also be incidental findings.
The primary objective in the treatment of a cardiac myxoma is to remove it surgically. This is performed by surgical shaving of the tumour from the septum4 or excision with a small amount of atrial septal tissue to prevent recurrence and the septum repaired, if necessary, with pericardial tissue.5
Echocardiographic assessment
TTE is a non-invasive method for assessing cardiac tumours and is useful for establishing their location, extent, attachment and haemodynamic consequences, as well as for excluding multiple-site involvement (see Box 1 for an echo checklist). Myxomas are gelatinous, lobulated and often pedunculated neoplasms that resemble a cluster of grapes, having an irregular surface and usually being attached to the endocardium via a stalk (ie pedunculated). A myxoma is generally heterogeneous in appearance, containing bright echodense regions if there is calcification. Superimposed onto this mass might be thrombus, although this is usually difficult to differentiate from the tumour mass on TTE. If there is suspicion of tumour infiltration, which cannot be confidently assessed, then transoesophageal echocardiography (TOE) might be needed. If all the salient information cannot be acquired with echocardiography, then a further evaluation with a CT or MR scan might be required.
Echocardiography checklist protocol for suspected atrial myxoma.

Acknowledgements
The authors wish to thank Caroline Pryke, Cardiology, Addenbrooke's Hospital, Cambridge, for her contributions to this article. The authors also thank Dr S Nagaraju, Neuropathology, Queen Elizabeth Hospital, Birmingham; Dr J Cross, Neuroradiology, Addenbrooke's Hospital,; Dr E O'Brien, Medicine, Addenbrooke's Hospital; Dr B Seymour, Neurology, Addenbrooke's Hospital; and the Departments of Neuropathology, Cardiology and Medical Photography, Addenbrooke's Hospital.
- © 2013 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.