
Abstract
First reported in 1898, post-dural puncture headache (PDPH) remains a significant clinical issue. Here, we present a brief case history and a summary of the current evidence for methods to reduce PDPH rates, along with the experience in our department of implementing these methods in clinical practice. The key points to note are that needle design, gauge and orientation, as well as stylet reinsertion, are factors known to affect the incidence of PDPH, and that there is no evidence to support the use of hydration and bed rest to reduce headache following dural puncture.
Introduction
A 30-year old woman presented to the emergency department with a three-hour history of severe frontal headache of sudden onset, radiating to the occiput. Her past medical history was unremarkable, with the exception of previous migraine as a teenager. Neurological examination and a computerised tomography (CT) scan of head revealed no significant focal abnormality. Therefore, the patient was admitted under the medical team for exclusion of subarachnoid haemorrhage (SAH).
With an improvement in the patient's symptoms noted, a diagnostic lumbar puncture was successfully carried out the following day. The patient was advised to maintain oral hydration and remain supine for two hours following the procedure. Cerebro-spinal fluid (CSF) analysis showed no xanthochromia, thus excluding SAH, and the patient was deemed fit for discharge.
However, within a few hours of the procedure, the patient developed further severe headache (worse on standing) with associated vomiting. She was reviewed the following day and it was felt these symptoms were in keeping with post-dural puncture headache (PDPH). After discussion with the patient, the decision was taken to proceed to epidural blood patch (EBP) the following day, should the headache remain severe.
The patient's symptoms improved spontaneously over the course of the subsequent two days, without the need for EBP. She was discharged with mild residual headache following a five-day admission, some four days after having initially been deemed fit. The patient felt that the procedure had resulted in worsening of her headache, significantly prolonging her hospital stay, and later submitted a formal written complaint.
Discussion
Since first described by Bier in 1898,1 post-procedure headache has been a frequent complication of both diagnostic and therapeutic dural puncture. This phenomenon has been attributed to continued CSF leakage from the puncture site.2 The incidence of PDPH can prove difficult to measure in clinical practice, with rates of up to 70% reported. We estimate to have approximately 50 cases per year in our department. Here, we examine the current evidence for methods of reducing PDPH and assess the practical implications of introducing these to our department.
Several factors have been postulated to affect the incidence of PDPH. These can be broadly divided into the following: patient, procedural and other factors. PDPH is known to occur more frequently in the young, those with a low body mass index, women (particularly in pregnancy) and those with either pre-existing headache or previous PDPH.3–5 It is also likely that the patient's psychological status affects the development of PDPH.6
Procedural factors that alter the incidence of PDPH include the needle design, gauge and orientation,7,8 as well as stylet reinsertion.6 It has also been suggested that other factors, including operator experience, caffeine administration and bed rest, influence the development of PDPH.
Needle gauge
The gauge of the needle used for dural puncture has been widely reported to affect the development of PDPH. Indeed, this has been proposed as the single most important factor,9 with needle gauge directly related to the incidence of PDPH4,5 (Table 1).
Rates of PDPH according to needle gauge. Adapted with permission from Bezov et al (2000).9
However, the use of smaller needles may be associated with technical difficulties and higher rates of procedure failure, particularly with needles <29 G.5,9 The use of 22G needles for diagnostic lumbar puncture has been advocated by the American Academy of Neurology,10 as use of smaller needles renders CSF collection and measurement of opening pressures difficult.12
Needle design
Needles can be either cutting (‘traumatic’) or pencil-point (‘atraumatic’) (Fig 1). There is a large body of evidence to support the use of pencil-point needles in reducing the incidence of PDPH. The mechanism for this effect has largely been attributed to the needle design, whereby the needle tip separates, rather than cuts, dural fibres.7,9,12 However, at electron microscopy, it has been observed that such needles cause more dural trauma compared with cutting needles.13 This has been postulated to generate a greater inflammatory response that, in turn, promotes more effective dural repair, thereby reducing CSF leakage.
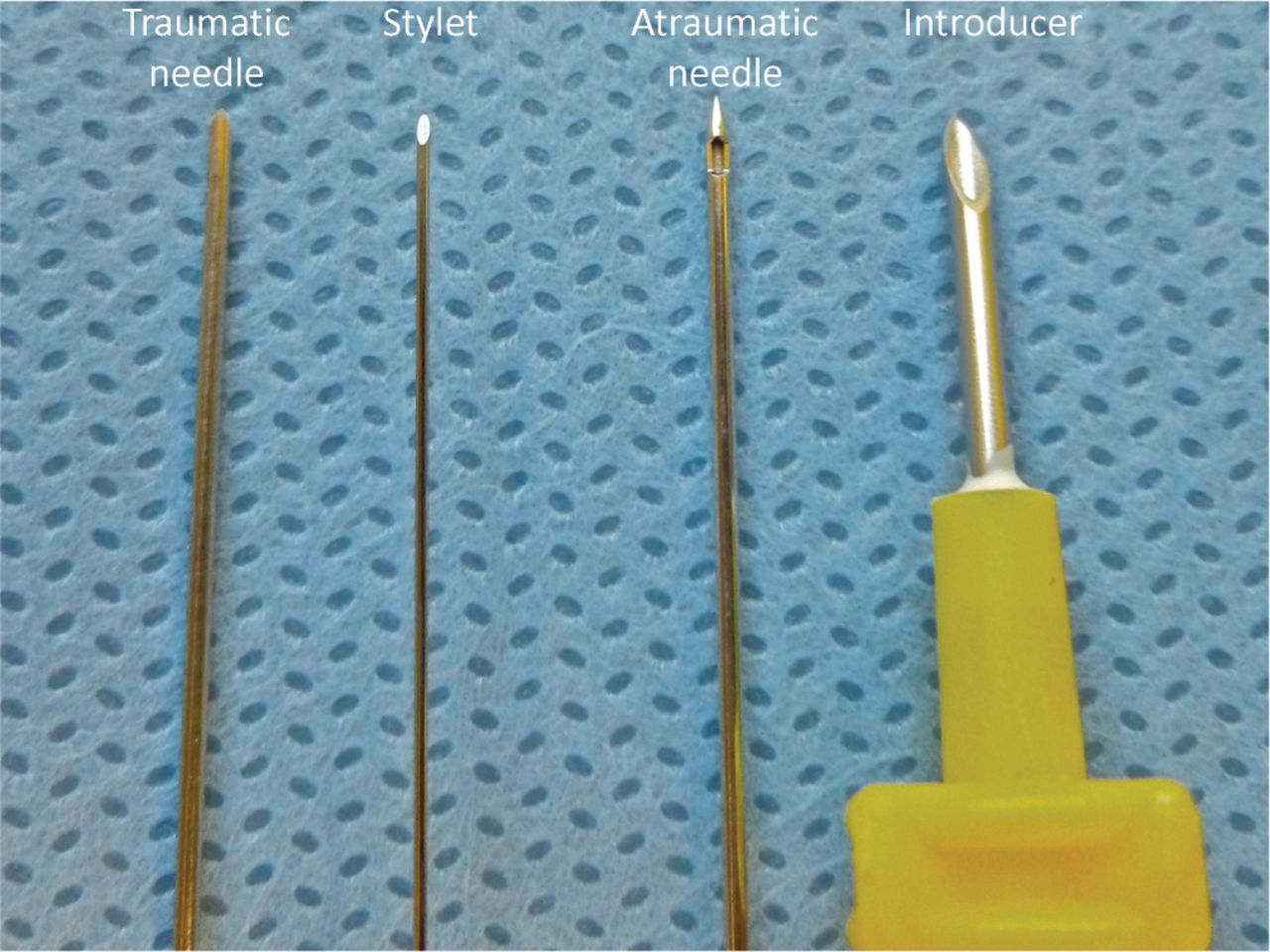
Illustration of dural puncture equipment.
However, such needles have been associated with certain negative features. Van den Berg and colleagues observed that such needles were more likely to induce an iatrogenic pain response.14 This phenomenon has been attributed to aspects of the needle design. The authors postulated that dural separation and stretch constitute a painful stimulus; other groups have implicated the positioning of the needle orifice. Given that the opening is situated on the barrel, rather than at the tip of, the needle, deeper insertion into the subarachnoid space is required before CSF is obtained. This would increase the likelihood of contact with the cauda equina and, therefore, paraesthesia.11
Additionally, it has been observed that because certain pencil-point needles are thinner walled, they can bend more easily,9 and so could be associated with increased operator difficulty and procedure failure. This issue remains controversial, but could theoretically be circumvented by the use of an introducer.
Needle orientation
Based on a meta-analysis, Richman et al15 concluded that insertion of traumatic needles with the bevel parallel to the long axis of the spine, rather than in a perpendicular direction, reduced the incidence of PDPH (although rates remain significantly higher than for pencil-point needles)8. This is likely to be attributable to reduced fibre injury, but may be of less consequence when considering the use of pencil-point needles.
Stylet reinsertion
The effect of stylet reinsertion on the development of PDPH has been examined by a single randomised trial.6 Strupp et al found that reinserting the stylet when using pencil-point needles significantly reduced the incidence of PDPH. It is uncertain whether this finding can be extrapolated to the use of traumatic needles as, to date, no randomised control trials have been conducted in this area.
Other factors
There is no evidence from the current body of data to suggest that the incidence of PDPH is significantly affected by bed rest,9,16 hydration,2,3 volume of CSF removed or the number of attempts at dural puncture.9 It is possible that administration of intravenous (rather than oral or intramuscular) caffeine has a protective role,9 although there is no clear consensus on this issue at present. There is conflicting evidence regarding the effect of operator experience, with reports of both a significant relationship17 and no correlation.2,8
Conclusions
In our department, dural puncture is carried out for diagnostic purposes only. This requires measurement of opening pressure and collection of CSF over a relatively brief period, and it is likely that the use of needles smaller than 22 G will be impractical. Therefore, it may be necessary to restrict needle use to 22 G only.
Insertion of cutting needles parallel to the long axis of the spine is an effective method of reducing the incidence of PDPH and is easily effected in clinical practice. The role of stylet reinsertion when using cutting needles has yet to be fully elucidated. Stylet insertion does not increase the technical difficulty of dural puncture, although care must be taken to ensure the sterility of the stylet between removal and reinsertion. Taking these points into consideration, we recommend stylus reinsertion in our department.
Although it is widely accepted that use of pencil-point needles significantly reduces the rates of PDPH, implementing their use in our department has proved challenging. From our experience, their flexibility renders skin penetration and needle advancement difficult. It may be possible to overcome this issue through the use of an introducer. Our departmental lumbar puncture protocol, based on the evidence in this review, is detailed in Box 1.
Protocol for lumbar puncture on the emergency assessment unit

- © 2013 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.