
Abstract
Chronic stable angina is the most common manifestation of ischaemic heart disease in the developed world and is associated with impaired quality of life and increased mortality. The pathogenesis of stable angina is complex and often, albeit not always, involves flow-limiting epicardial coronary artery stenoses (atheromatous plaques) that reduce the ability of the coronary circulation to deliver appropriate blood supply to the myocardium. The coronary microcirculation can also play an important role. An imbalance between myocardial oxygen supply and metabolic oxygen demand causes the symptoms of angina pectoris and represents a major therapeutic target. Rational treatment requires a multi-faceted approach combining lifestyle changes, aggressive management of modifiable coronary artery disease risk factors, pharmacological therapy and myocardial revascularisation when appropriate. Despite modern therapies, many patients continue to suffer from angina. Several new anti-anginal drugs have been introduced that might allow more effective symptom control. These novel agents have specific mechanisms of action and fewer side effects compared to conventional drugs. The combined use of traditional and novel treatments is likely to increase the proportion of patients who are managed successfully with medical therapy alone. This article briefly reviews recent advances in the pharmacological management of chronic stable angina pectoris, highlighting how an understanding of the prevailing pathogenic mechanisms in the individual patient can aid appropriate selection of therapeutic strategies and improve clinical outcome.
Introduction
Current treatment strategies for chronic stable angina aim to control symptoms, reduce the ischaemic burden and improve prognosis by preventing the progression of atherosclerotic coronary artery disease (CAD) and its consequences. Ideally, the treatment of angina should be tailored to the individual patient's needs, taking into consideration the characteristics and severity of symptoms, the location, severity and functional significance of coronary artery stenoses, the presence of co-morbidities and patient preference. For each individual patient, the efficacy of the agent and their side effects, together with patient compliance, are important determinants for the success or the failure of a given treatment.
Overview of chronic stable angina
The term angina pectoris refers to William Heberden's classic description of the clinical symptoms of angina, as reported to the Royal College of Physicians in 1768.1 There is currently no systematically agreed definition for angina pectoris and the term is used to define both the typical chest pain associated with myocardial ischaemia and the syndrome characterised by chest pain, myocardial ischaemia and obstructive atherosclerotic coronary artery disease. In this article, we use the term ‘angina’ in relation to the occurrence of typical central chest pain associated with myocardial ischaemia, irrespective of the presence or absence of flow-limiting organic coronary artery stenosis.
Angina is considered to be ‘chronic’ and ‘stable’ when symptoms are present for at least two months, without changes in severity, character or triggering circumstances.2
Stable angina is the most common clinical manifestation of ischaemic heart disease, affecting 58% of patients with CAD.3 Its prevalence increases with age, rising from roughly 8% in men and 3% in women aged 55–64 years, to 14% in men and 8% in women aged 65–74 years, in England.4 The annual mortality rate resulting from coronary heart disease in patients with stable angina is 0.9–1.4% per year.5
Stable angina results from an imbalance between coronary blood supply and myocardial oxygen demand, which is often, but not always, associated with the presence of obstructive CAD. Transient myocardial ischaemia typically causes ‘constrictive’ chest discomfort, resulting from the activation of mechano- and chemo-sensitive myocardial receptors. Patients with stable angina might or might not present with typical symptoms, and ‘silent’ myocardial ischaemia can be present in patients with diabetes mellitus and in the elderly. The typical clinical characteristics of chronic stable angina are summarised in Box 1.
Pathophysiological and pathogenic mechanisms: determinants of clinical presentation
The pathogenesis of angina is often multi-factorial. The basic underlying mechanism that leads to angina is an imbalance of myocardial oxygen supply and demand. This often occurs as a direct result of flow-limiting CAD, but it can also be due to coronary artery spasm limiting blood supply, coronary microvascular dysfunction and/or several other contributing mechanisms. To a great extent, the underlying pathogenic mechanism determines the pattern of clinical presentation, leading to effort-induced angina, mixed angina or angina at rest.
Effort-induced angina
Long-standing obstructive epicardial CAD causes angina by providing a fixed limitation of coronary blood flow, which prevents physiological matching of coronary blood supply to exercise-induced increases in myocardial metabolic demand. A stenosis of 50% or more in the left main coronary artery, or 70% or more in another major epicardial artery, is defined as ‘obstructive’.6 Symptoms of effort-induced stable angina resulting from flow-limiting coronary stenoses often occur at a predictable and reproducible threshold, triggered by physical activity and/or emotional stress. The Canadian Cardiovascular Society (CCS) grading of angina is a functional classification of exercise tolerance that can be related to metabolic equivalent units (METs) and it is used in the assessment of exercise stress testing.7,8
‘Mixed’ angina
The imbalance of myocardial oxygen supply and demand in angina can also result from combined mechanisms. Excessive coronary artery vasoconstriction at the site of organic stenoses manifests clinically as ‘mixed angina pectoris’, in which patients present with variable-threshold effort angina and occasionally angina at rest.5,9
Microvascular angina
Coronary microvascular resistance is the main determinant of coronary flow reserve (the ratio of maximal induced myocardial flow to resting coronary blood flow). Abnormal vasodilatory responses of the coronary microcirculation can cause effort-related angina (microvascular angina). It is important to note that as few as 38% of patients without previously known heart disease who undergo elective diagnostic coronary angiography are found to have obstructive CAD.6 In many of these patients with typical angina symptoms, exercise-induced myocardial ischaemia is caused by coronary microvascular dysfunction. Patients with cardiac syndrome X — defined as typical exertional angina, positive stress test responses and normal coronary angiograms — experience transient myocardial ischaemia resulting from impaired endothelial function, which leads to abnormal coronary microvascular vasodilatation, increased coronary vasoconstriction, or both.10–12
In the ACOVA (Abnormal Coronary VAsomotion in patients with stable angina and unobstructed coronary arteries) study, approximately two-thirds of patients without significant epicardial CAD had positive intra-coronary acetylcholine tests for distal epicardial or microvascular spasm.13 Clinicians should be encouraged to think about the possibility of microvascular dysfunction or coronary microvascular spasm in patients who present with typical angina despite having angiographically normal coronary arteries.
Other contributing mechanisms
Following transient myocardial ischaemia, impaired diastolic relaxation and increased wall tension caused by calcium overload, which results from intracellular acidosis, and activation of late inward sodium currents worsens the oxygen imbalance and prolongs the angina episode.2 Further metabolic derangement, including abnormalities of substrate supply and utilisation, enzymatic activities and mitochondrial function, can also contribute to the pathogenesis.8 Aortic stenosis, hypertrophic cardiomyopathy, severe anaemia and thyrotoxicosis (when present) are other potential contributory factors that can worsen myocardial ischaemia.2
Diagnosis and management
Importance of the clinical history for diagnosis and management of stable angina pectoris
The accurate diagnosis of chronic stable angina (and the recognition of possible underlying pathogenic mechanisms) relies largely on obtaining a detailed clinical history. The severity of chest pain does not necessarily correlate to the extent of underlying CAD, but the burden of symptoms experienced by an individual patient will guide the nature and extent of the anti-anginal treatments used.
The CCS classification of angina can provide clinically useful diagnostic and prognostic clues that are important for patient management. In CCS grade I patients, angina is only precipitated by strenuous or severe and prolonged exertion; whereas at the other end of the spectrum, CCS grade IV patients, develop angina with minor exertion or even at rest.7 It is important to remember that CCS grade does not necessarily reflect CAD severity.14 By contrast, the occurrence of chest pain with progressively increased frequency and/or severity (‘crescendo’ angina), compared to the usual chronic stable symptoms, can be an expression of acute coronary syndrome (unstable angina and myocardial infarction) and must be monitored carefully and investigated promptly.
Diagnostic investigation
Further investigation is guided by a risk stratification that is based on pre-test probability, derived from age, sex, character of symptoms and cardiovascular risk factors, as outlined by the NICE (National Institute for Health and Clinical Excellence) guideline on chest pain.15 For low-risk CAD patients (10–29%) with stable symptoms, NICE recommends CT coronary calcium scoring as the first-line investigation.15 While the reasons behind this recommendation are sound, the practical implementation of this strategy is not always feasible or straightforward, and cardiologists often resort to alternative diagnostic testing with stress echocardiography or even exercise stress testing. Functional imaging with stress echocardiography, nuclear myocardial perfusion scanning or first-pass cardiac magnetic resonance scanning is advised for patients with moderate cardiovascular risk (30–60%).15 For high-risk patients (61–90%), NICE recommends proceeding directly to invasive coronary angiography.15 The use of ECG exercise tolerance testing to diagnose CAD is not recommended,15 albeit this relatively inexpensive test can often give useful functional information and, in practice, is still a useful diagnostic tool.
Pharmacological management of angina pectoris
Although the general principles of treatment (ie lifestyle modification and risk-factor management) are applicable to all patients with angina, treatment should be individualised where possible. It should aim to reverse or reduce the underlying pathophysiological mechanisms in order to relieve symptoms and improve cardiovascular risk profile. Key interventions include lifestyle changes (eg smoking cessation, dietary modification and increased physical exercise), management of hypertension, diabetes and obesity, and other secondary cardiovascular disease prevention measures, such as the use of anti-platelet and lipid-lowering agents, pharmacological anti-anginal therapies and percutaneous and/or surgical revascularisation when appropriate.4,5
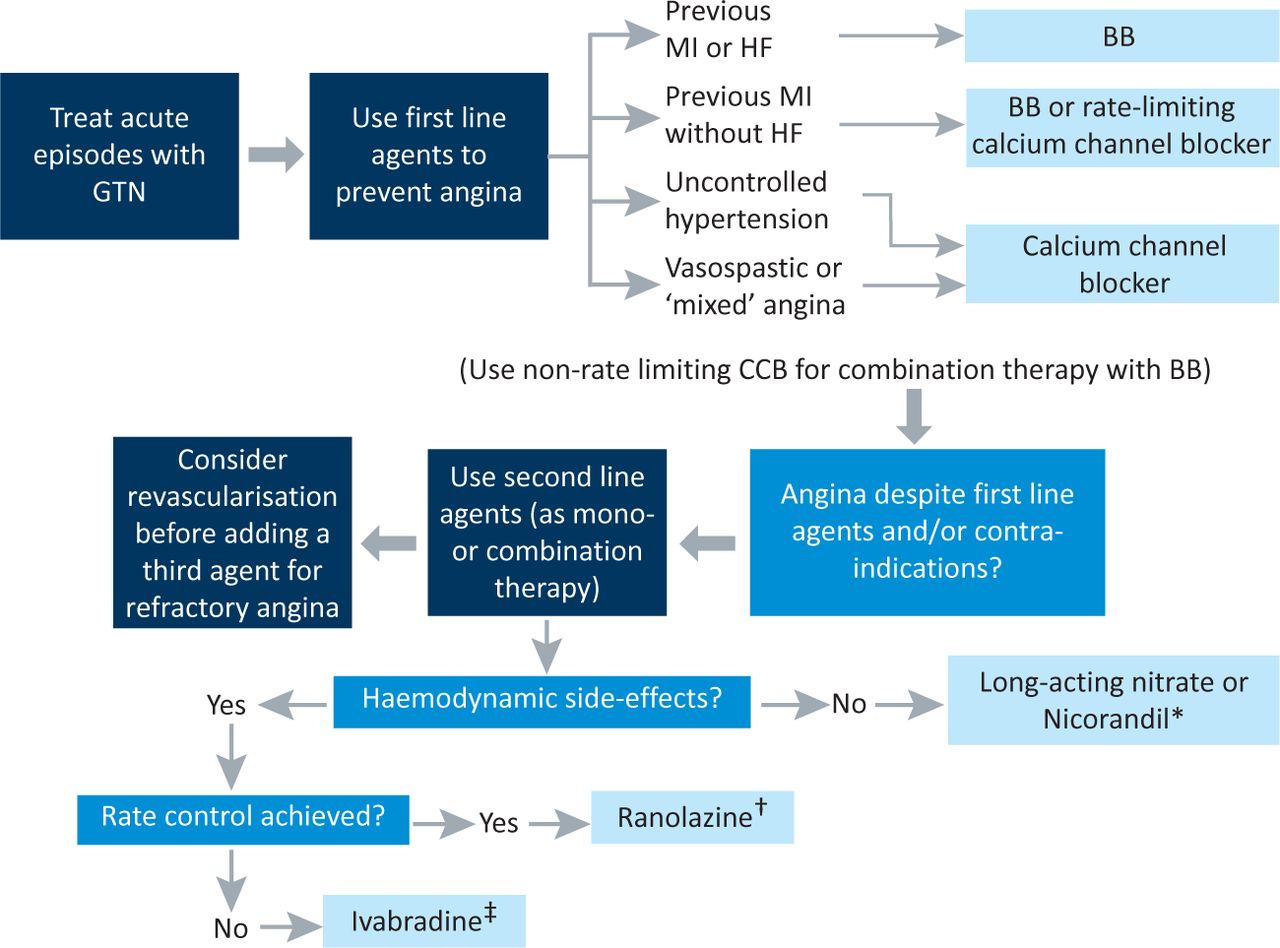
Fig 1 provides a proposed practical therapeutic algorithm that is based on recently updated NICE guidelines, and Table 1 summarises important clinical information for each of the currently used anti-anginal agents included in this treatment algorithm.4
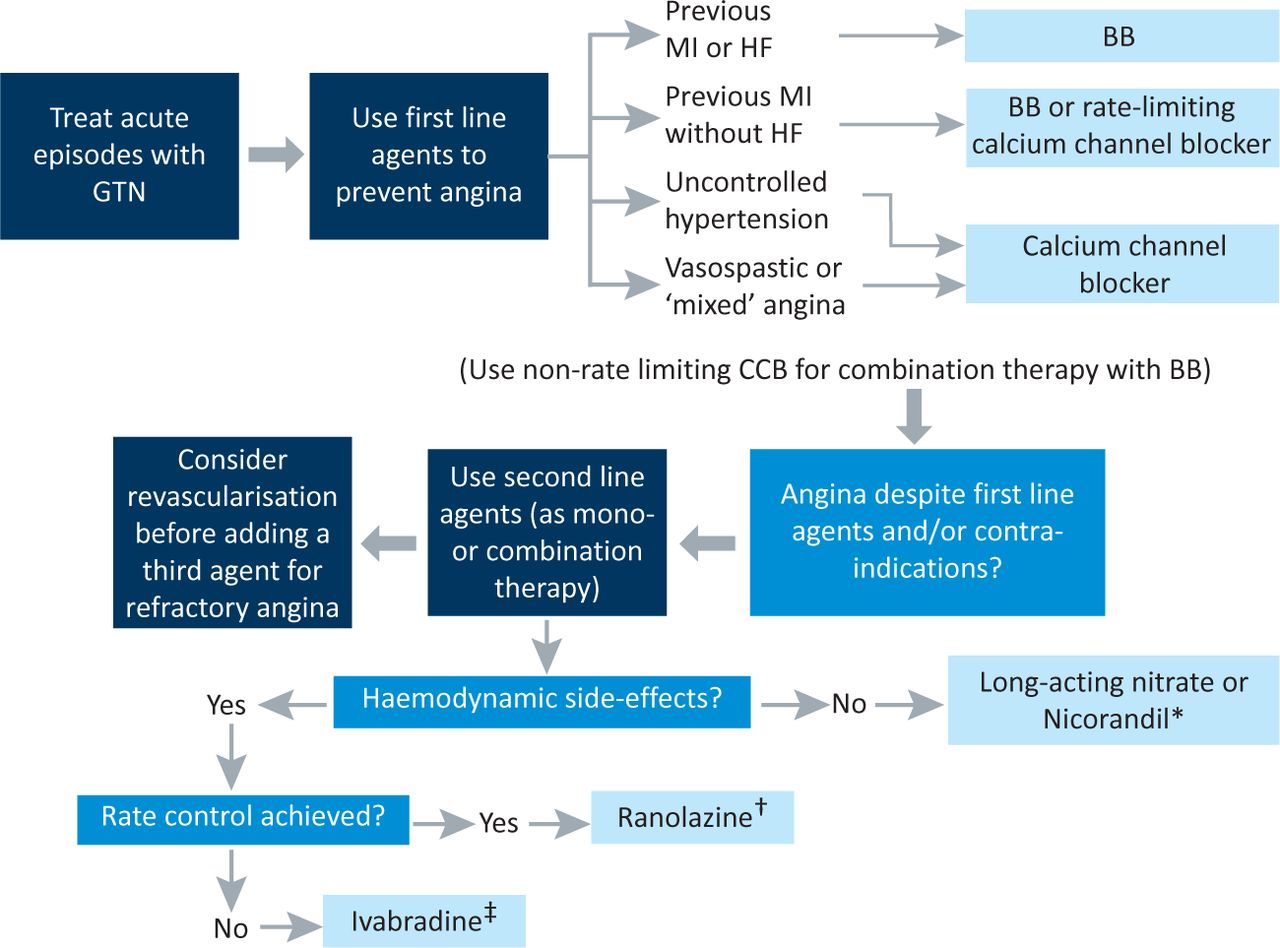
Proposed practical algorithm for pharmacological treatment of chronic stable angina based on NICE guidance.4 BB = beta-blocker; CCB = calcium channel blocker; DM = diabetes mellitus; GTN = glyceryltrinitrate; HF = heart failure; MI = myocardial infarction. *added cardio-protective properties; †improves HbA1c in DM; ‡prognostic benefit in HF.
Summary of anti-anginal drugs supported by NICE guidance.4
Treatment of chest pain episodes
Episodes of angina are best treated with sublingual glyceryltrinitrate (GTN). GTN acts as a nitric oxide donor, causing systemic and coronary vasodilatation. GTN is rapidly absorbed in the sublingual mucosae and its effects usually occur within 2–10 minutes. Common side effects of sublingual nitrate administration are headaches, dizziness, hot flushing and nausea. Contraindications for the use of GTN include aortic stenosis, hypertrophic cardiomyopathy, systemic hypotension and co-administration with phosphodiesterase-5 inhibitors (eg sildenafil). GTN is recommended for all patients with stable angina, unless contraindicated. When prescribing GTN, patients should be given advice regarding how and when to use GTN and potential side effects that they may experience. They should be advised to inform their doctor if the symptoms are not controlled. GTN can also be useful in preventing episodes of exertional angina when used prior to undertaking physical exertion.
First-line anti-anginal drugs
β-adrenergic receptor blockers (beta-blockers) and calcium-channel blockers are considered to be first-line anti-anginal drugs and have been shown in many studies to prevent angina and myocardial ischaemia. The TIBET (Total Ischaemic Burden European Trial) study showed that atenolol produced similar anti-anginal benefits when compared to slow-release nifedipine; no significant additional benefits were seen when the two agents were combined.16 In the APSIS (Angina Prognosis Study in Stockholm) study, patients with stable angina treated with either metoprolol or verapamil had similar rates of cardiovascular events and mortality.17 The choice between these two drug classes is generally guided by contraindications, the presence of co-morbidities and patient preference. If one of these agents is not well tolerated, the other can be tried instead. If combination therapy is required, the use of a non-heart-rate limiting dihydropiridine calcium channel blocker (eg amlodipine or slow-release nifedipine) is recommended. The anti-anginal actions of beta-blockers result from a reduction in heart rate, contractility and blood pressure, which result in a reduced myocardial oxygen requirements. Also, by lowering the heart rate, the diastolic component of the cardiac cycle is prolonged, which improves myocardial flow. For maximal efficacy, long-acting, cardioselective beta-blockers that have no intrinsic sympathomimetic activity are preferred. The dose should be titrated to achieve a target resting heart rate of 50–60 beats per minute. The prognostic benefit of beta-blockers in angina has been extrapolated from studies of post myocardial infarction but has not yet been documented in stable angina.16
The potential benefits of beta-blocker therapy are often limited by side effects and contraindications. Among the most common side effects of beta-blockers are fatigue, dizziness, syncope, bronchospam, hyperglycaemia, depression and erectile dysfunction. These agents are contraindicated in patients with reactive airway diseases, severe bradycardia, 2nd or 3rd degree heart block, sick sinus syndrome, hypotension, acute heart failure and peripheral vascular disease. Beta-blockers are not generally used in patients with vasospastic angina because of the possibility that unopposed α-adrenergic receptors might have unwanted effects. Abrupt withdrawal of beta-blockers can cause rebound myocardial ischaemia.
Calcium channel blockers act on L-type Ca2+ receptors and lead to systemic and coronary vasodilatation, reducing afterload and improving myocardial blood flow. Like beta-blockers, non-dihydropyridines (eg verapamil and diltiazem) have additional anti-anginal affects through reductions in heart rate and contractility. Long-acting preparations are preferred. Common side effects of blockers include dizziness, headache, fatigue, flushing, abdominal pain, nausea and peripheral oedema. Like beta-blockers, non-diydropyridine calcium channel blockers are contraindicated by severe bradycardia, 2nd or 3rd degree heart block, sick sinus syndrome, hypotension and acute heart failure.
Second-line anti-angina therapies
For patients whose symptoms are not well controlled by beta-blockers and calcium-channel blockers, or if contraindications exist for these agents, several options supported by NICE guidelines4 are available. These include: vasodilators such as long-acting nitrates and nicorandil, a drug that selectively slows the heart rate; ivabradine, and ranolazine, an agent that acts on the fast sodium current to improve cardiac metabolism. When and in which order these second-line agents are used in clinical practice is based on several variables, including pathogenic mechanisms, patient characteristics and co-morbidities, drug interactions and patient preference.
Long-acting nitrates
Although there is no evidence that nitrates improve patient prognosis, long-acting nitrates (eg isosorbide mononitrate or isosorbide dinitrate) have been shown to reduce the frequency and severity of angina attacks in patients with stable angina when given alone or in combination with first-line anti-anginal agents. The mechanisms of action, side effects and contraindications for these drugs are similar to those described under sublingual nitrates above. The development of nitrate tolerance and the adverse effects of long-acting nitrates reported recently require consideration before these drugs are prescribed for a given patient.18,19
Nicorandil
Nicorandil acts as both a nitric oxide donor and a sarcolemmal K+-adenosine triphosphate (K-ATP)-dependant channel opener, causing K+ efflux and subsequent hyperpolarisation and inhibition of L-type Ca2+ channels, leading to systemic and coronary vasodilatation. The beneficial effects of nicorandil monotherapy are similar to those of metoprolol, amlodipine, diltiazem and nitrates.20–23 In the IONA (Impact Of Nicorandil in Angina) study, a reduced rate of fatal and non-fatal myocardial infarction and reduced admission for cardiac chest pain were seen in patients taking nicorandil in addition to other standard anti-anginal therapies.24 The cardio-protective properties of nicorandil might be due to ischaemic preconditioning mediated by activation of mitochondrial K-ATP channels.24 Common side effects of nicorandil are headaches, dizziness, nausea, vomiting and flushing. Metformin might antagonise the effects of nicorandil by closing K-ATP channels.25 The use of phosphodiesterase-5 inhibitors and nitrates should be avoided by those taking nicorandil because of the risk of profound systemic hypotension.
Ivabradine
Ivabradine is a novel selective heart-rate-lowering anti-anginal drug. Ivabradine inhibits If channels, thereby affecting the intrinsic pacemaker cells of the sino-atrial node. When activated by hyperpolarisation in diastolic range voltages and by adrenergically driven increases in cyclic adenosine monophosphate, the If channel, causes an inward Na+/K+ ionic current across the sarcolemma, leading to spontaneous depolarisation of myocytes in the sino-atrial node.26 Inhibition of the If current lwers the heart rate. Ivabradine is more effective in patients who have increased If channel activity.26 It does not affect blood pressure, atrio-ventricular node conduction or contractility. On average, ivabradine reduces resting heart rate by 10 beats per minute.25 Complete If blockade results in a maximum 30–40% reduction in heart rate due to compensation from other populations of pacemaker cells.27
The anti-anginal efficacy of ivabradine has been shown not to be inferior to atenolol and amlodipine in major trials.28,29 In the BEAUTIFUL (morBidity-mortality EvAlUaTion of the If inhibitor ivabradine in patients with coronary disease and left-ventricULar dysfunction) trial, lower rates of hospital admission for fatal and non-fatal myocardial infarction and coronary revascularisation were seen with ivabradine compared to placebo in patients with stable angina and heart rate ≥70 beats per minute.30
Ivabradine is indicated for patients with stable angina who are in sinus rhythm and cannot tolerate or have contraindications for conventional heart-rate-lowering agents (ie beta-blockers and non-dyhidropyridine calcium channel blockers), and for patients established on conventional monotherapy whose resting heart rate is sub-optimal. Common side effects include visual ‘flashing lights’ that are often mild and transient, headache, dizziness, blurred vision, 1st degree heart block and ventricular extra-systoles. Contraindications are bradycardia, sick-sinus syndrome, heart block, atrial fibrillation, acute myocardial infarction, acute heart failure, hypotension, and renal and hepatic failure. Ivabradine is metabolised by the CYP3A4 liver enzymes, and significant interactions might occur with drugs that interfere with these enzymes (eg azole anti-fungals, diltiazem, verapamil, macrolide antibiotics and grapefruit juice). Ivabradine can be used safely in patients with asthma and chronic obstructive pulmonary disease.31
Ranolazine
Ranolazine is a piperazine derivative that is thought to exert its anti-anginal effect by inhibiting ischaemic-induced late inward Na+ currents, preventing Ca2+ overload and reducing diastolic wall tension and extrinsic coronary artery compression.32 It might also improve endothelial-mediated coronary vasodilatation.33 It was originally thought to act as an anti-metabolic drug, but the concentration required to inhibit myocardial fatty-acid oxidation is much higher than the therapeutic levels used to treat angina.32 An advantage of ranolazine is that it does not cause significant haemodynamic changes, with on average less than 2 beats per minute reduction in heart rate and less than 3 mmHg decrease in systolic blood pressure.25 It is, however, associated with a dose-dependant increase in QT-interval.25
The clinical efficacy of ranolazine in chronic stable angina as monotherapy and in combination with other anti-anginal drugs has been shown in MARISA (Monotherapy Assessment of Ranolazine in Stable Angina),34 CARISA (Combination Assessment of Ranolazine In Stable Angina)34 and ERICA (Efficacy of Ranolazine in Chronic Angina) trials.36 No reduction in cardiovascular death, acute myocardial infarction or recurrent ischaemia was seen in the MERLIN-TIMI 36 (Metabolic Efficiency with Ranolazine for Less Ischemia in Non-ST-elevation acute coronary syndromes) trial when ranolazine was taken instead of placebo.37
Common side effects of ranolazine are dizziness, nausea, constipation, abdominal pain and headaches. Contraindications to ranolazine are prolonged QT-interval and co-administration with other QT-prolonging drugs, previous history of ventricular tachycardia, and moderate to severe renal impairment or severe hepatic failure. Ranolazine is metabolised by liver CYP3A4 and to a lesser extent by CYP2D6 enzymes, consequently there is a potential for drug interactions. Ranolazine is also a weak inhibitor of cytochrome p450 enzymes and therefore doses of P-glycoprotein substrates (eg simvasatin and digoxin) might need to be reduced for those taking ranolazine.25
Other anti-anginal drugs
A number of other anti-anginal drugs exist. These are not currently included in NICE guidance, but could in future become available for use in the UK. Trimetazedine, a thiolase that efficiently inhibits beta-oxidation of fatty acids in the myocardium, shifting cardiac metabolism towards more efficient pathways, is used in many European countries as a metabolic modulator.38 Angiotensin-converting-enzyme inhibitors are not strictly speaking anti-anginal agents but they have been shown to improve prognosis in patients with diabetes or heart failure and following a myocardial infarction. They are therefore indicated in those circumstances and studies are required to determine their true role in stable angina pectoris.
F 15845 (3-(R)-[3-(2-methoxyphenylthio-2-(S)-methylpropyl]amino-3,4-dihydro-2H-1,5-benzoxathiepine bromhydrate) is a newly described selective inhibitor of the persistent Na+ current, which has shown anti-ischaemic properties and an ability to prevent ischaemia-induced arrhythmias in animal models; it currently is being assessed in phase II clinical trials.39–41
Individual approach to anti-anginal drug selection
In many patients, multiple drugs with different mechanisms of action might be necessary for successful symptom control. Many patients, however, are unable to tolerate conventional angina therapies, mainly those eliciting haemodynamic side effects. The NICE guideline recommends adding a third drug only when two anti-anginal drugs do not satisfactorily control symptoms and the patient is awaiting revascularisation, or in patients for whom revascularisation is not appropriate.4
For patients with previous myocardial infarction or heart failure, beta-blockers are the preferred first-line agent because of their proven prognostic benefit.5 Rate-limiting calcium channel blockers can also improve prognosis in post-myocardial-infarction patients who do not have heart failure.5 Calcium channel blockers are preferred in patients with angina who require good hypertensive control.27 Long-acting nitrates are a logical choice for patients whose symptoms persist despite their taking beta-blockers or calcium channel blockers but who tolerate short-acting nitrates. As nitrates do not improve prognosis, however nicorandil might provide similar anti-anginal effects but with added cardio-protective benefit.
For patients who develop hypotension or other haemodynamic side effects with conventional anti-anginal therapies, ivabradine and ranolazine are suitable options as they do not exert vasoactive actions. Ivabradine controls heart rate efficiently without significantly causing haemodynamic effects and can be used safely by patients with obstructive airways disease. Ivabradine can also be used in combination with beta-blockers. In the ASSOCIATE (Antianginal efficacy and Safety of the aSsociation Of the If Current Inhibitor ivAbradine with a beTa-blockEr) trial, the combination of ivabradine and atenolol was effective and well tolerated in patients with stable angina, and it was not associated with untoward effects.42 Ivabradine has also been shown to reduce cardiovascular death and hospital admission in patients with systolic heart failure.43 In patients with diabetes, ranolazine has an added metabolic benefit in that it has been associated with a significant reduction in HbA1c concentrations.44,45
It is important to remember that angina results from the interplay of a number of complex vascular and metabolic mechanisms and does not result solely from the presence of obstructive epicardial CAD. Anti-anginal regimes should be, as much as possible, aimed at addressing the prevailing underlying pathophysiological mechanisms in the individual patient. This is particularly important for patients who have chest pain, objective documentation of myocardial ischaemia and angiographically ‘normal’ coronary arteries, in whom coronary microvascular dysfunction and distal epicardial vasoconstriction often play an import role. Calcium channel blockers and other vasodilator agents are useful to these individuals. In patients with true vasospastic angina, ie Prinzmetal's variant angina, calcium channel blockers (usually at high doses) are the best treatment option and are preferred over nitrates for long-term control of symptoms, albeit nitrates (particularly sublingual GTN) can also play an important role in management.5
Conclusions and future directions
Medical management of stable angina includes lifestyle modification and optimal medical therapy, which encompasses both aggressive pharmacological control of the cardiovascular and metabolic risk profiles, and individualised anti-anginal drug regimes, targeted at specific underlying pathogenic mechanisms. Medical treatment should be regarded as the most important initial intervention and as such should be implemented for all patients as it might reduce the need for invasive coronary intervention, particularly for patients with mild to moderate CAD in whom the prognostic benefit of revascularisation remains unproven.
Recent advances in the pharmacological management of chronic stable angina offer more precise and individualised solutions. Drug selection can be tailored to the individual on the basis of their underlying pathophysiological mechanisms, which often can be identified from the clinical history. The main aims of therapy remain to control symptoms, thereby improving quality of life, and ultimately to prevent progression of the underlying atherosclerotic coronary heart disease and its long-term complications. For the future, angiogenic gene therapy, using genes that encode vascular endothelial growth factors and fibroblast growth factors, and intramyocardial hematopoietic stem cell therapy are currently being developed. At present and in theory, these offer reasonable promise.27,46
- © 2013 Royal College of Physicians








{kind=link}