
Abstract
This overview of systematic reviews (SRs) aims to evaluate critically the evidence regarding the adverse effects of herbal medicines (HMs). Five electronic databases were searched to identify all relevant SRs, with 50 SRs of 50 different HMs meeting our inclusion criteria. Most had only minor weaknesses in methods. Serious adverse effects were noted only for four HMs: Herbae pulvis standardisatus, Larrea tridentate, Piper methysticum and Cassia senna. The most severe adverse effects were liver or kidney damage, colon perforation, carcinoma, coma and death. Moderately severe adverse effects were noted for 15 HMs: Pelargonium sidoides, Perna canaliculus, Aloe vera, Mentha piperita, Medicago sativa, Cimicifuga racemosa, Caulophyllum thalictroides, Serenoa repens, Taraxacum officinale, Camellia sinensis, Commifora mukul, Hoodia gordonii, Viscum album, Trifolium pratense and Stevia rebaudiana. Minor adverse effects were noted for 31 HMs: Thymus vulgaris, Lavandula angustifolia Miller, Boswellia serrata, Calendula officinalis, Harpagophytum procumbens, Panax ginseng, Vitex agnus-castus, Crataegus spp., Cinnamomum spp., Petasites hybridus, Agave americana, Hypericum perforatum, Echinacea spp., Silybum marianum, Capsicum spp., Genus phyllanthus, Ginkgo biloba, Valeriana officinalis, Hippocastanaceae, Melissa officinalis, Trigonella foenum-graecum, Lagerstroemia speciosa, Cnicus benedictus, Salvia hispanica, Vaccinium myrtillus, Mentha spicata, Rosmarinus officinalis, Crocus sativus, Gymnema sylvestre, Morinda citrifolia and Curcuma longa. Most of the HMs evaluated in SRs were associated with only moderately severe or minor adverse effects.
Introduction
Herbal medicines (HMs) are popular in many countries, including the UK.1,2 The reasons for this widespread use are complex – see, for example, Ernst and Furnham (2000)3 and Ernst (2008)4 – but the assumption that ‘natural’ can be equated with ‘safe’ is certainly an important factor.5 However, this notion is dangerously misleading: HMs contain pharmacologically active ingredients, some of which have been associated with adverse effects (AEs).6–9
The aim of this article is to provide an overview and critical evaluation of evidence from systematic reviews (SRs) of AEs associated with the use of HM products. It is important to remember that it does not attempt to identify or define all AEs of HM products: in many cases, probable AEs have been implicated but were not documented in an SR.
Methods
Electronic literature searches were conducted in January 2012 to identify SRs of AEs of HMs used in any type of clinical condition. The following electronic databases were used: Medline and Embase (via Ovid), the Allied and Complementary Medicine Database (AMED), CINHAL (via EBSCO) and the Cochrane database. Search terms were constructed using ‘herbal medicine’ and ‘adverse events’ terms and their derivatives, medical subject heading (MeSH) terms and ‘review’ in the title of the article (details of the search strategy are presented in the supplementary Appendix S1). In addition, our own extensive department files were searched by hand.
No restrictions on language or time of publication were imposed. Abstracts of reviews thus located were inspected and those that seemed to meet the inclusion criteria were retrieved for further evaluation by both authors. Systematic reviews were defined as articles that included an explicit and repeatable method. To be included, SRs had to pertain to AEs of HMs in human patients or volunteers. If multiple SRs were found for one specific HM, the most up-to-date, methodologically sound and independent review was chosen. Mixtures of more than one HM were excluded. Non-systematic reviews and reviews pertaining to the effectiveness of HMs were also excluded.
The quality of the methods underlying all SRs was assessed independently by the two reviewers using the modified Oxman score.10,11 This is a validated instrument that consists of the following domains for assessing the quality of the methods of review articles: reporting of search methods and their comprehensiveness, repeatable eligibility criteria, avoidance of selection bias and supportiveness of conclusions. We scored each of the above criteria as 1 (fulfilled), 0 (partially fulfilled) or −1 (not fulfilled). A final result of 0 or lower means the review has major flaws, of 1–2 means minor flaws and 3–5 means minimal or no flaws.
Results
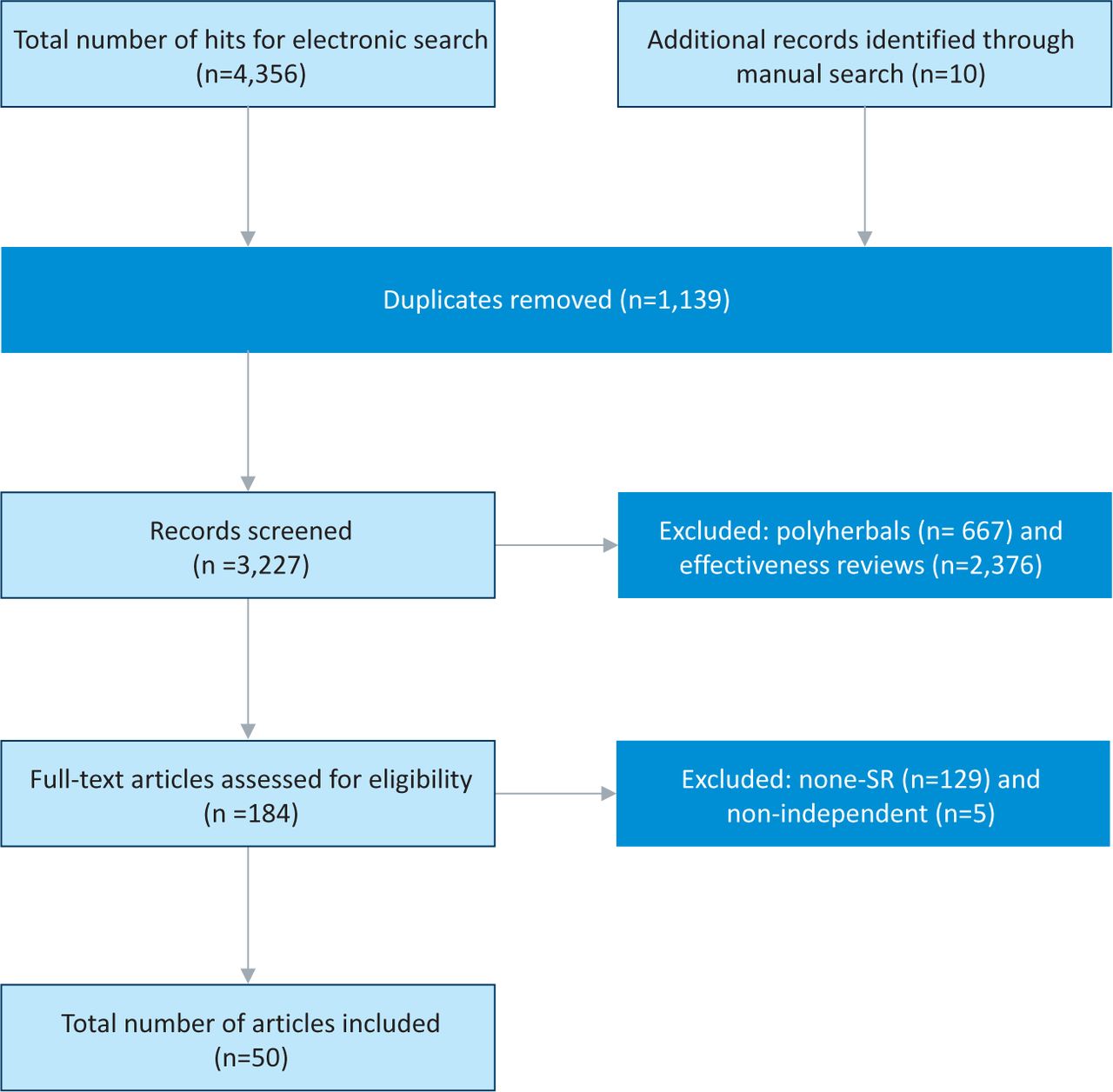
The searches generated 4,366 potentially relevant titles and abstracts, of which 4,316 were excluded (Fig 1). Fifty SRs met our inclusion criteria;12–61 these originated from Canada,21,22 Denmark,26 Germany,17,46 Italy,19,20,62 South Africa,41 the UK12,18,24,29 and the USA.13–16,23,25,27,28,30–40,42–45,47,50–61 In these SRs, adverse effects of the following HMs were evaluated: Agave americana,50 Aloe vera,52 Boswellia serrata,15 Calendula officinalis,16 Camellia sinensis,28 Capsaicin spp.,44 Cassia senna,61 Caulophyllum thalictroides,22 Cimicifuga racemosa,48 Cinnamomum spp.,21 Cnicus benedictus,53 Commifora mukul,36 Crataegus spp.,20 Crocus sativus,59 Curcuma longa,43 Echinacea spp.,24 genus Phyllanthus,26 Ginkgo biloba,29 Gymnema sylvestre,60 Harpagophytum procumbens,17 Herbae pulvis standardisatus,34 Hippocastanaceae,32 Hoodia gordonii,41 Hypericum perforatum,45 Lagerstroemia speciosa,38 Larrea tridentate,33 Lavandula angustifolia Miller,14 Melissa officinalis,35 Mentha piperita,51 Mentha spicata,57 Morinda citrifolia,42 Panax ginseng,18 Pelargonium sidoides,56 Perna canaliculus,54 Petasites hybridus,23 Piper methysticum,37 Rosmarinus officinalis,58 Salvia hispanica,39 Serenoa repens,12 Silybum marianum,25 Stevia rebaudiana,40 Taraxacum officinale,30 Thymus vulgaris,13 Trifolium pretense,27 Trigonella foenum-graecum,47 Vaccinium myrtillus,55 Valeriana officinalis,31 Viscum album46 and Vitex agnus-castus.19 A variety of safety concerns were raised, ranging from clinical AEs12,19,20,22,24,25,31,41,44,46,48 through effects on blood coagulation29 to a combination of drug interactions.13–17,21,23,27,32–40,45,47,50–61 The number of primary studies included in the SRs ranged from 138 to 216.28 The types of primary reports varied from case studies to epidemiological investigations. Some SRs also included secondary analyses such as review articles.15,23,45,47,51,52,59,61 One SR employed a meta-analytical approach.26
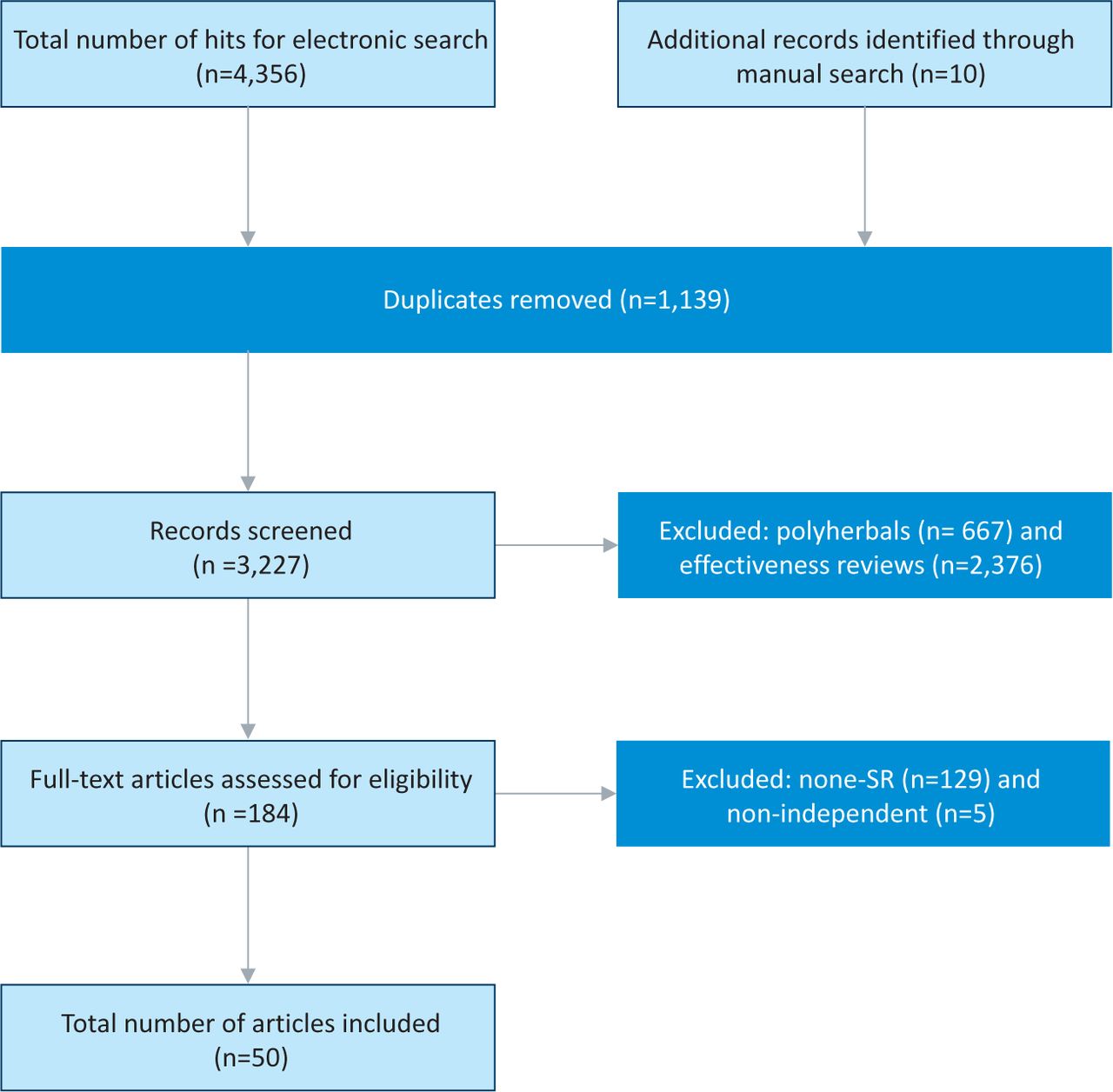
Flow diagram.
Thirty-one SRs concluded that the HM in question was safe.13–21,23–26,29,31,32,35,38,39,42–45,47,50,53,55,57–60 Fifteen SRs reported moderately severe AEs,12,22,27,28,30,36,40,41,46,48,49,51,52,54,56 and four SRs concluded that the HM in question was not safe (see Supplemental Tables S1 and S2).33,34,37,61 Thirteen SRs mentioned the duration of AEs,18,20,22,24,26,28,33,42,44–46,48,50 which ranged from 48 hours to 11 months. Forty-two SRs failed to mention conflict of interest of the authors.13–18,22,23,25–27,30–45,47–61 Thirty-two SRs made no mention of any source of funding.13–17,22,23,27,30,34–41,44,47,48,50–61
The quality of the methods of the included SRs was mixed (Table 1). Fifteen SRs had only minimal or no flaws (3–5 points on the modified Oxman scale),12,19–21,24–26,28,29,31,37,45,46,48 20 SRs had minor weaknesses (1–2 points)18,22,27,32,33,36,38,47,50–61 and 15 SRs had major flaws in their methods (≤0 points).13–17,23,30,34,35,39–44
Quality ratings for included systematic reviews of herbal medicines.
The HMs were used for a wide variety of clinical conditions, including allergic rhinitis;23 anxiety;14,37 asthma, Crohn's disease and ulcerative colitis;15 bronchitis or cough;13 cardiovascular diseases;20,32,39,40 common colds;56 constipation;61 diabetes;21,38,47,60 depression;45 dyspepsia;53 hyperlipidaemia;36 inflammatory skin conditions;16 insomnia;31 irritable bowel syndrome;34 liver disease;25 lower urinary tract infections or benign prostatic hyperplasia;12 menopausal symptoms;27,48 obesity;41 pain;44,30 pregnancy;22 prevention28 or treatment14,33,42,46 of cancer; rheumatic conditions;15,17,43,54 various clinical conditions18,19,24,29,51,52,55,57–59 and viral infections.26,35 Three SRs also included studies of healthy individuals.18,24,42
Discussion
This overview aimed to critically evaluate the data from SRs of AEs of HMs. Most SRs indicated that the HMs in question were reasonably safe.13–21,23–26,29,31,32,35,38,39,42–45,47,50,53,55,57–60 Only four SRs arrived at clearly negative conclusions about the safety of the reviewed HM.33,34,37,61
The AEs ranged from mild to severe. Mild AEs included pain,15,57,61 allergic reactions,13,17,19,20,21,24,36,37,53,58,59 burning sensation,44,51,55,57 constipation,23,34 dermatitis,50,57–59 diarrhoea,17,21,23,31,35,47,52,56,61 ‘difficulties’,16 dizziness,13,20,31,32,40 drowsiness,31 dry mouth,34 fatigue,12,45 gastrointestinal upset,15,19–21,23–26,30,32,36,37,39,43,45,48,53–56 headache18–20,25,31,32,34,35,36,45 loss of appetite,30 menstrual disorders,19 mouth burning,21 muscle spasm,32 muscle weaknesses,40 nausea,12,14,15,19,20,26,31,32,35,40,55,61 rash,24,48,56 sleep disorders18,35 and vomiting.14,21,23,30,53,61 Moderately severe AEs included anorexia, reversible neutropenia,14 coagulation abnormalities,29 confusion, slurred speech, blurred vision, sedation, hyper-reflexia,34 dysphagia, severe nausea,23 electroencephalogram (EEG) changes,35 increased fibrinolysis, inhibition of platelet aggregation,36 loss of consciousness,21 platelet aggregation,30 pruritis32 or vertigo, photophobia and mydriasis.34 Severe AEs included acute psychosis,34 cerebral haemorrhage, death,12,37,52 coma, respiratory arrest, tachycardia,37,51,56 hallucinations, convulsions, rhabdomyolysis and renal failure,36,51 acute lung injury,51,54 haemorrhage, circulation failure,20,56 hepatitis,41,48,52,54,61 hyperkalaemia,42,46 liver damage,28,30,42,46,61 nephrotoxicity,32 cirrhosis, liver failure,37,54 perinatal stroke, acute myocardial infarction, congestive heart failure,54 severe multiorgan hypoxic injury,22 carcinoma,33,61 perforation of the gastrointestinal tract,61 seizures and epilepsy.58
The large number of included SRs means that it is not easy to provide practical guidance through this labyrinth of HMs and multitude of AEs. Readers with an interest in one specific HM or one particular AE might look up the relevant SRs and refer to the primary reports. Readers with a more general interest in the safety of HMs would probably prefer to study those SRs that report serious AEs.33,34,37,61
The quality of the methods of some of the included SRs was frequently not optimal. This could be due to the fact that several of the articles were not designed as typical SRs. Many of the papers that scored poorly on quality were monograph-type publications, which are relatively frequent in the literature on HM. As these articles do nevertheless contribute relevant information, we decided to include them in our overview. Despite the fact that many SRs failed to achieve high-quality scores, we believe that virtually all of them contribute to our knowledge of AEs associated with HMs. In our view, none of the defects noted in Table 1 completely invalidates the SR in question. Even an SR that scored poorly on the formal quality rating can serve an important purpose when it alerts us to the risks associated with the HM in question.
Several challenges in methods and concepts were faced when undertaking this overview. We analysed data from SRs of AEs of specific HMs and omitted SRs of polyherbal preparations and effectiveness reviews (see Supplemental Table S3).63–81 It was frequently impossible to differentiate between herb–drug interactions and AEs, as these questions were addressed simultaneously. Herb–drug interactions, adulteration and contamination obviously can also cause AEs.1,82–84 Our plan is to address these issues in specific analyses to be published as separate overviews.
This overview has further limitations that must be kept in mind when interpreting the evidence. Although a comprehensive search strategy was employed, there is no guarantee that all relevant SRs have been located. All SRs are prone to publication bias, and so any such bias may have been transferred to our overview. As we only included SRs, our overview cannot provide information on HMs for which no SR is available. A comprehensive review of all information available to date regarding AEs of HM would be a monumental task that by far exceeds the possibility of a single journal article.85
The nature of the evidence reviewed here also requires a brief comment. Rigorous and comprehensive SRs of AEs should consider anecdotal data such as case reports. Such evidence is clearly relevant for assessing safety issues, but it does not lend itself to establishing cause and effect. We therefore ought to be cautious when interpreting such data and should critically question causality on a case-by-case basis.
In conclusion, numerous SRs of HMs have recently become available. Most of these SRs reveal mild adverse effects associated with HMs; however, some HMs might pose more severe health threats.
Funding
Paul Posadzki was supported by a fellowship from the Royal College of Physicians, London.
- © 2013 Royal College of Physicians








{kind=link}