
Abstract
This systematic review aimed to estimate the prevalence of use of complementary and alternative medicine (CAM) in the UK. Five databases were searched for English language, peer-reviewed surveys published between 1 January 2000 and 7 October 2011. In addition, relevant book chapters and files from our own departmental records were searched by hand. Eighty-nine surveys were included, with a total of 97,222 participants. Most studies were of poor methodological quality. Across surveys on CAM in general, the average one-year prevalence of use of CAM was 41.1% and the average lifetime prevalence was 51.8%. In methodologically sound surveys, the equivalent rates were 26.3% and 44%, respectively. In surveys with response rates >70%, average one-year prevalence was nearly threefold lower than in surveys with response rates between 21% and 50%. Herbal medicine was the most popular CAM, followed by homeopathy, aromatherapy, massage and reflexology. Many patients and consumers in the UK use CAM; healthcare professionals should therefore responsibly advise their patients about the use of CAM.
Introduction
Complementary and alternative medicine (CAM) has been defined as ‘diagnosis, treatment and/or prevention which complements mainstream medicine by contributing to a common whole, satisfying a demand not met by orthodoxy, or diversifying the conceptual framework of medicine’.1 Annual out-of-pocket expenditure in the UK on CAM has been estimated at £1.6 billion.2 Despite many assertions to the contrary, CAM is not free of a potential to cause harm, particularly as it is frequently used for serious, treatable conditions.3,4 Vis a vis such data, it would seem crucial to provide reliable data on the prevalence of its use to help prioritise a research agenda, inform policy and define educational needs.
The aim of this systematic review was to summarise and critically evaluate surveys monitoring the prevalence of use of CAM by patients and consumers in the UK during the past decade.
Methods
Systematic literature searches were performed for all English language references using AMED, CINAHL, Cochrane, Embase and MEDLINE for surveys published between 1 January 2000 and 7 October 2011. Details of the search strategy are presented in supplementary Appendix S1 (published online only). In addition, relevant book chapters, review articles and our own departmental files were searched by hand for further relevant articles. Surveys that examined the prevalence of the use of CAM by patients and consumers in the UK and provided quantitative data on prevalence were included. Surveys that only reported qualitative data were excluded. Information from the included surveys was extracted according to predefined criteria and was assessed descriptively by two independent reviewers. Any disagreements were settled through discussion. Surveys were further classified according to the following criteria: sample size, response rate and random sampling. Finally, we created a category of ‘high-quality surveys’, which had to have a sample size of >1,000, have a response rate of >70% and employ a random-sampling technique.
The following methods were considered to be CAM: acupuncture/acupressure, Alexander technique, aromatherapy, autogenic training, Ayurveda, (Bach) flower remedies, biofeedback, chelation therapy, chiropractic, Feldenkrais, herbal medicine, homeopathy, hypnotherapy, imagery, kinesiology, massage of any form, meditation, naturopathy, neural therapy, osteopathy, Qigong, reflexology, relaxation therapy, shiatsu, spiritual healing, static magnets, tai chi and yoga. Non-herbal dietary supplements and vitamins, psychotherapy, physical exercises and some physio-therapeutic modalities such as electrotherapy and ultrasound were not considered to be CAM and were therefore excluded from analyses.
We ranked the top five methods of CAM (1 = most popular) from each survey and then averaged the rank numbers across the surveys to generate an overall ranking. We also provided the total number of surveys in which a particular method of CAM was the most prevalent/popular and then calculated the averages of those figures. Where available, we calculated the average of the percentage of responders who stated that they experienced benefit or were satisfied with CAM, as well as those who reported adverse effects after using CAM and the cost for purchasing CAM.
Results
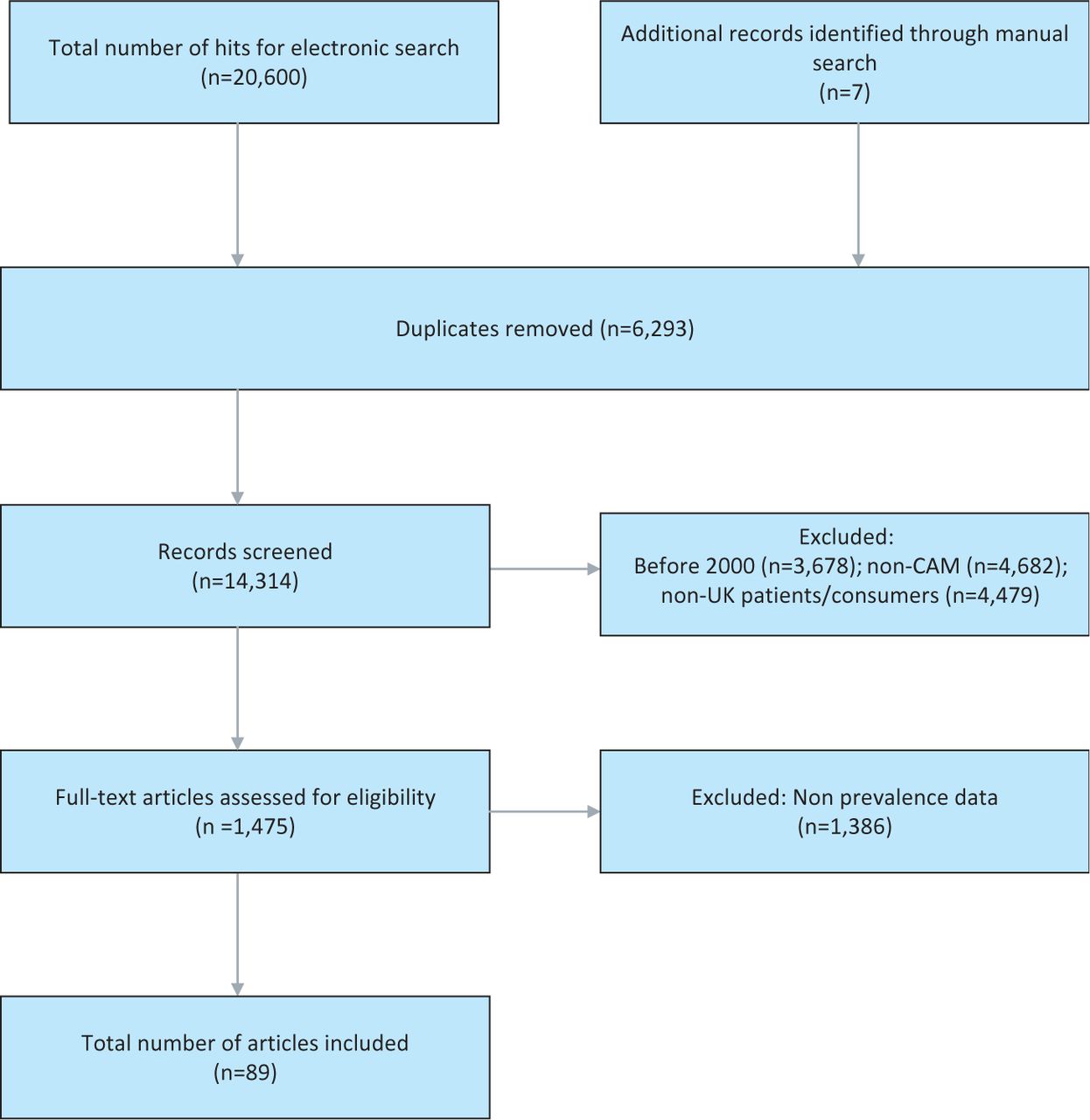
The searches generated 20,607 articles, of which 20,518 were excluded (see Fig 1). Eighty-nine surveys met our eligibility criteria.2,5–92 Detailed characteristics of the included studies are presented in Supplementary Table S1, while Supplementary Table S2 represents the surveys included on specific CAM modalities (both tables are published online only). Fifty-three surveys originated from England, 11 from Scotland, six from Wales and one from Northern Ireland. The remaining 19 surveys pertained either to the whole of the UK or their geographical location was not clearly specified.

Flow diagram showing screening process. CAM = complementary and alternative medicine.
The total number of patients included in the 89 surveys was 97,222. Seventy-four surveys were on CAM in general, while the other 15 were on specific CAM modalities: 10 on herbal medicine,7,27,28,31,38,43,66,70,83,90 two on acupuncture,13,50 two on homeopathy21,22 and one on chiropractic.85 The participants included patients with asthma,26 cancer, 8,9,15,18,19,31,32,39,42,51–56,59,60,63,66,70,71,73,79 dermatological conditions,6,38,47,57 epilepsy,12 HIV,14 hypertension,77 infertility,10,13 multiple sclerosis,30,72,85 pain,16,41,49,69,84 Parkinson's disease, 75 paediatric illneses,11,23,47,51,61,64,76,87,91 surgical procedures27,62 and various other clinical conditions.2,21,50,74,82 Thirteen surveys referred to the use of CAM in healthy consumers.7,20,22,23,34,36,44,45,58,65,67,68,78
The use of a random-sampling method was mentioned in 13 (14.6%) surveys.2,7,16,20,24,26,31,34,44,55,58,64,65 The response rates ranged from 13.8% to 100% (average 69.7%). Across surveys on CAM in general, the average one-year prevalence was 41.1% (range 9.2–100%) and the average lifetime prevalence was 51.8% (range 29–71%). Across surveys on specific methods of CAM, the average one-year prevalence of use of herbal medicines was 64.2% (range 36–92.4%) and the lifetime prevalence of use of homeopathy was 70% (range 70–70%).
Perceived effectiveness of CAM was mentioned in 41 (50.5%) surveys.2,5,6,10,11,15,19,21,23,25,26,31,33,34,37,42,45,47–49,51–57,60–63,68,72–74,76,79–82,84,86,88,89,92 The average perceived effectiveness across all surveys on CAM in general was 49.7% (range 10–100%). The incidence of AEs was reported in 11 (12.3%) surveys11,28,31,52,53,55,56,69,82,83,89 and the incidence across surveys on CAM in general amounted to 5% (range 2.1–11.8%). The costs of CAM were provided in 23 (25.8%) surveys.2,11,12,18–20,23,26,30,42,46,49,52–56,59,60,64,68,73,81 Based on four surveys, the average cost of using CAM per patient per month was £15.99 (range £8.80–28.00).2,30,42,46
Table 1 summarises the prevalences according to sample size, response rate and survey design. In surveys with response rates of >70%, the average one-year prevalence was 30.8% (range 9.2–47.5%) and the average lifetime prevalence was 58.8% (range 37–71%). In surveys with a sample size of >1,000, the average one-year prevalence was 34.9% (range 10–100%) and the average lifetime prevalence was 58.7% (range 44–71%). In surveys with a random-sampling method, the average one-year prevalence was 21.15% (range 10–28.3%) and the average lifetime prevalence was 45.3% (range 44–46.6%). One survey met all of the above criteria for methodological acceptability44 and reported one-year prevalence of 26.3% and lifetime prevalence of 44%.
Average prevalence of use of complementary and alternative medicine as a function of sample size, response rate, survey design and study population.
Herbal medicine was ranked as the most popular type of CAM in 24 surveys (second in four, third in four, fourth in none and fifth in one), homeopathy in eight surveys (second in seven, third in two, fourth in two and fifth in none), aromatherapy in six surveys (second in seven, third in five, fourth in three and fifth in two), massage in six surveys (second in seven, third in two, fourth in one and fifth in none) and reflexology in four surveys (second in two, third in four, fourth in one and fifth in one) (based on surveys of use of CAM in general). Using our ranking method, herbal medicine was the most popular form of CAM (32.4% of surveys), followed by homeopathy (10.8%), aromatherapy (8.1%), massage (8.1%) and reflexology (5.4%). The average percentage values of the five most popular methods of CAM were 29.5% for herbal medicine, 37.7% for homeopathy, 24.5% for aromatherapy, 15.2% for massage and 25.4% for reflexology. Prayer and relaxation were both ranked first in 2.7% of all surveys. Acupuncture, chiropractic, osteopathy, reiki and yoga were all ranked first in 1.3% of surveys.
Discussion
Our aim was to investigate the prevalence of use of CAM in the UK by conducting a systematic review of all recent relevant surveys. Our findings are noteworthy in several respects. Firstly, the amount of surveys published in the last decade is larger than many of us would have expected. It has been noted before that ‘the number of [CAM] surveys published each year considerably and consistently exceed[s] the number of clinical trials.93 Secondly, the methodological quality of almost all of these surveys was limited.
The abundance of flawed surveys combined with the paucity of sound survey data have the potential to mislead. Depending on what article we select, we could choose almost any prevalence rate we wish. This huge variability of data on the prevalence of use of CAM has been noted repeatedly.93,94 Proponents of CAM tend to use the allegedly high prevalence of its use to argue that CAM should be made more widely available: most patients in the UK pay for CAM out of their own pocket and the argument of enthusiasts for CAM, in the name of equality and fairness, is that CAM should not just be available to those who can afford it but it should be paid for by the NHS.
A particular concern is the often low response rate in the included surveys. It seems reasonable to assume that those volunteers who fail to respond have less interest in CAM than those who do; low response rates thus might generate falsely high prevalence rates. It would be relatively easy to take this factor into account – for example, by assuming a range of prevalence rates in non-responders, which would provide a range of prevalence rates depending on such assumptions. None of the included surveys has adopted this method.
Further problems with surveys of CAM relate to the fact that no universally accepted definition of CAM exists. This means that different surveys monitor the use of different methods, which inevitably creates confusion. 93 Furthermore, none of the questionnaires used in the included surveys has been formally validated. This means that there is no certainty that they quantify what they aim to measure.
Given the abundance of problems with CAM surveys, it is difficult to trust their findings. This applies not just to the reported prevalence rates but also to all other information that such surveys might generate. For instance, we noted that the average perceived effectiveness of CAM was substantial. Assuming that proponents of CAM predominantly answer such surveys, this information is unsurprising but less than reliable. Similarly, one cannot fail to notice that the methods of CAM that are deemed to be among the most popular vary to a disconcerting extent. Considering that other evidence contradicts our list of the most popular treatments based on the included surveys, and in view of the fact that this list could be prone to frequent and rapid fluctuations, we advise caution when interpreting these data.
These and other problems seriously limit the conclusions we are able to draw despite the plethora of data. Even though many articles on CAM start with the notion that the use of CAM has been increasing, we have no sound data to confirm that this is the case in the UK. Despite the common assumption that use of CAM in the UK is high, we have little solid evidence that this is true.
In conclusion, many surveys are monitoring the prevalence of use of CAM in the UK. Due to numerous flaws and problems, the information they provide is less than reliable.
Funding
PP has a fellowship from the Royal College of Physicians (RCP), London.
Competing interest
The RCP had no role in the study design or in the data collection or interpretation.
Tables S1 and S2, and Appendix S1 can be found online at www.clinmed.rcpjournal.org.
- © 2013 Royal College of Physicians








{kind=link}