
Lesson
Case presentation
An 18-year-old Asian man presented to the emergency department with a three-day history of fever, lethargy, acute generalised abdominal pain and non-productive cough. He had experienced a flu-like illness three weeks prior to this presentation. Other than a history of acne, he was otherwise fit and well, with no new skin changes. He occasionally smoked flavoured tobacco via a water pipe but had no history of alcohol consumption or illicit drug use. Household contacts were well, and he had travelled to Pakistan a few years ago. He had received all childhood immunisations, including the Bacillus Calmette–Guérin (BCG) vaccine.
On initial assessment, the patient had a temperature of 40.1°C, a regular pulse of 122 beats per minute, blood pressure of 93/59 mmHg, respiratory rate of 24 breaths per minute and oxygen saturation of 94% on room air. On examination, he was alert and not in respiratory distress. He had no signs of jaundice, anaemia, clubbing or cyanosis, no peripheral signs of infective endocarditis, and no palpable lymph nodes. His pulse was tachycardic and his heart sounds revealed an ejection systolic murmur. His lungs were clear on auscultation, with good equal bilateral air entry and no added sounds. On abdominal examination, he had generalised abdominal tenderness but no palpable masses. Bowel sounds were normal, and hernia orifices were clear. Examination of his skin showed non-inflamed lesions, including open comedones and nodules on his face and back, which were in keeping with chronic acne.
Investigations and treatment
Laboratory tests revealed the following salient results: white cell count 14.6×109/l, neutrophil count 12.4×109/l, lymphocyte count 0.6×109/l, eosinophil count 0.2×109/l, platelet count 184×109/l, international normalised ratio 1.4 and C-reactive protein (CRP) 254 mg/l. Liver function tests and urea and electrolytes were normal. Arterial blood gas results on room air showed: pH 7.59, oxygen partial pressure 10.4 kPa, carbon dioxide partial pressure 3.82 kPa, partial pressure of bicarbonate 19.8 kPa and base excess −3.2 mEq/l. The capillary blood glucose level was 9.0 mmol/l and urine dipstick test was positive only for blood.
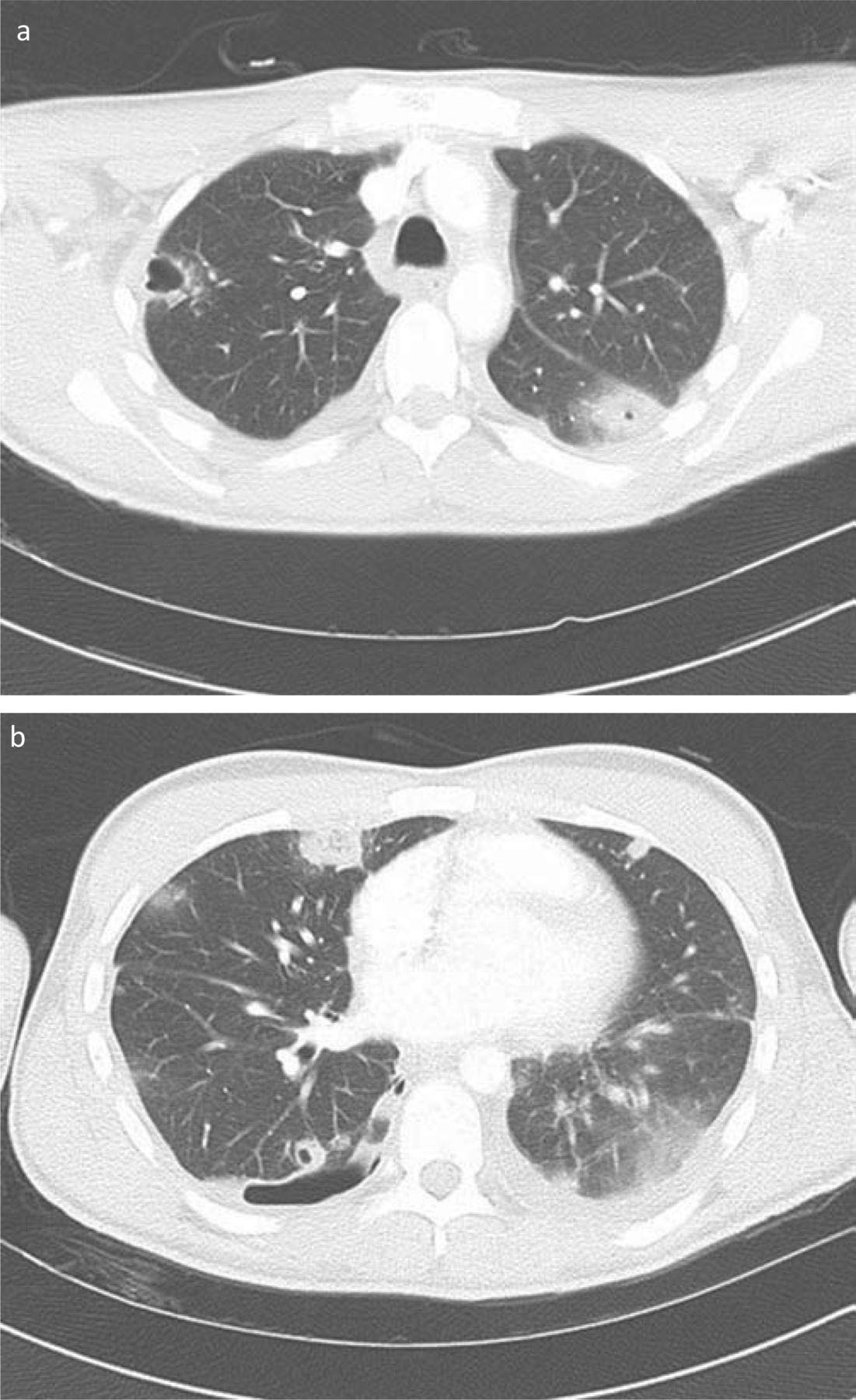
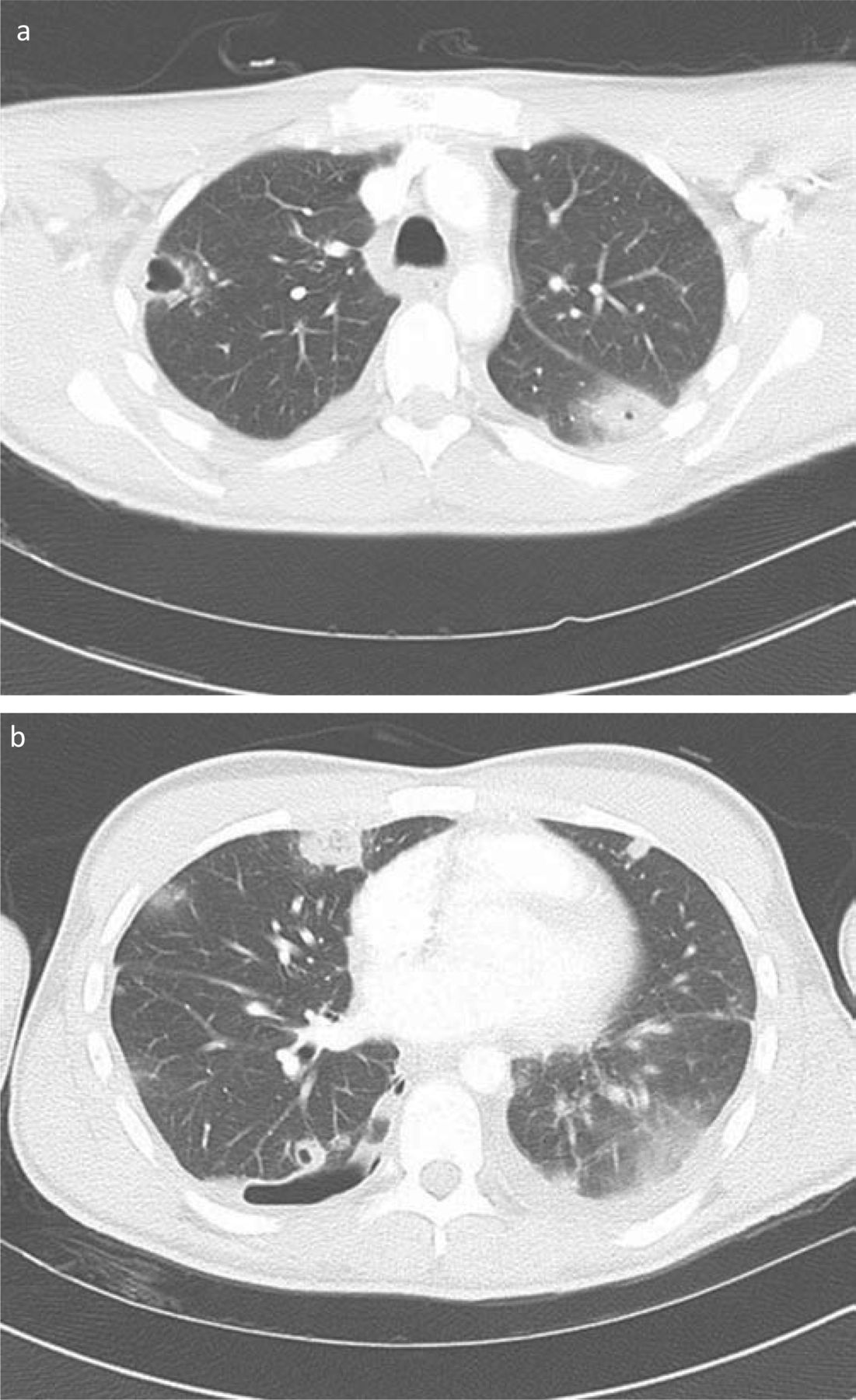
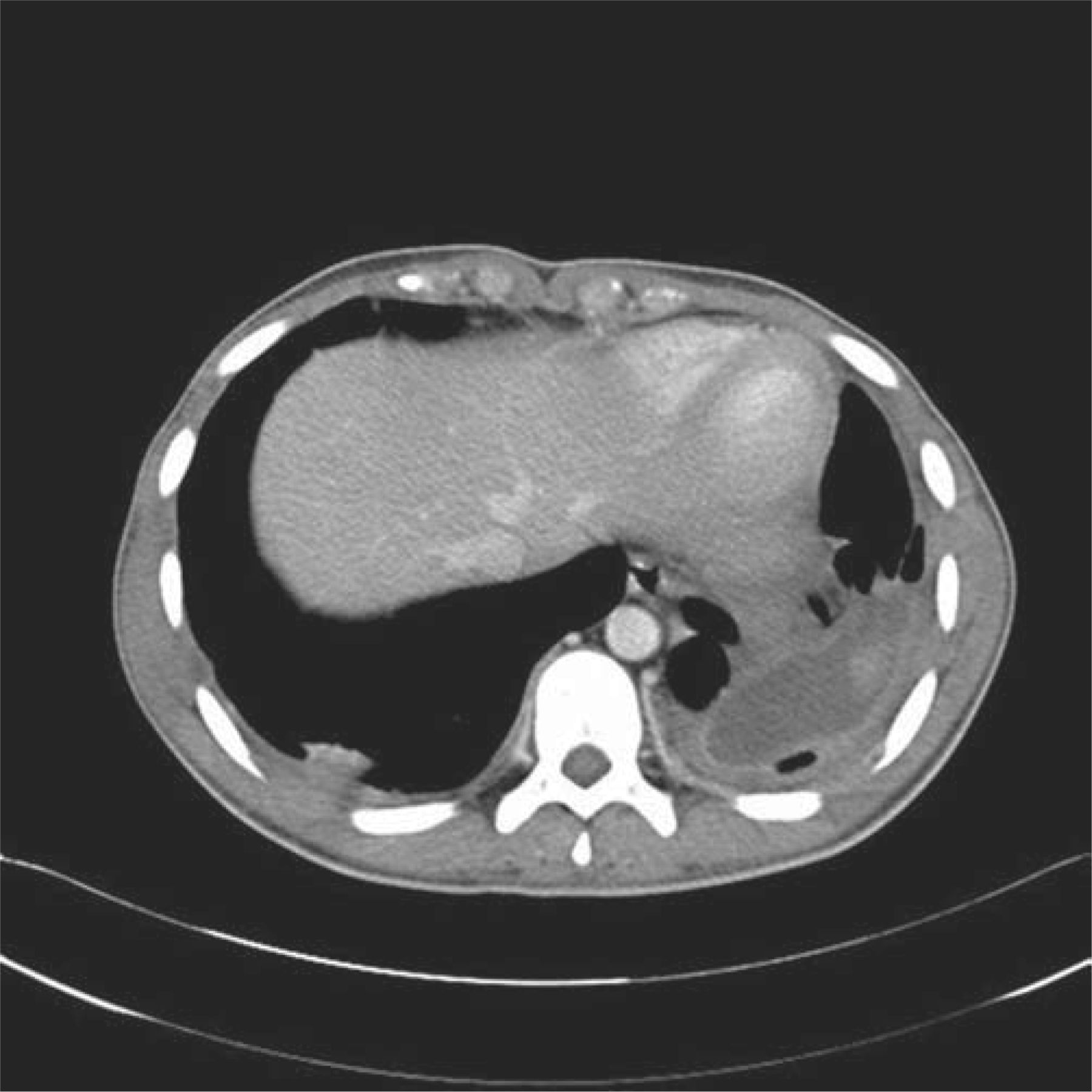
Initial chest X-ray was normal (Fig 1), but a surgical referral was sought to rule out a duodenal perforation given his severe acute abdominal pain. As the results of the chest X-ray were normal, computed tomography (CT) scan of the abdomen and pelvis was requested. This did not show any intra-abdominal pathology, but it demonstrated multiple pulmonary nodules, along with bilateral lower lobe inflammatory changes (Fig 2). An echocardiogram of his heart showed no vegetations and normal valves.

CXR performed on admission.
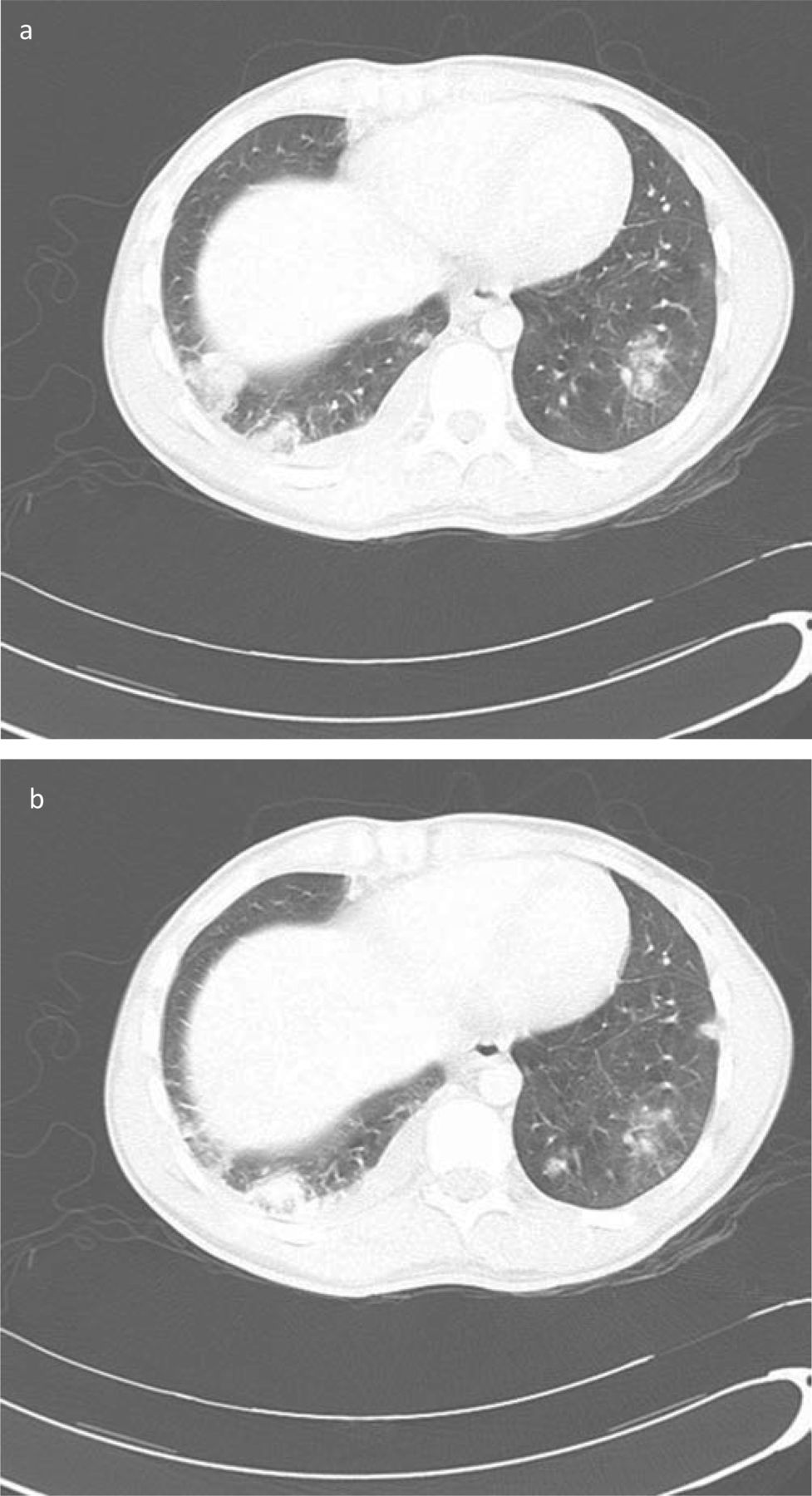
CT scan of abdomen, pelvis, and thorax performed within 48 hours showing bases of lung.
The patient was admitted to a respiratory ward and started on empirical treatment for atypical community-acquired pneumonia, with tuberculosis and small-vessel vasculitis as possible differential diagnoses. However, the patient continued to deteriorate despite treatment, with haemoptysis, a swinging temperature, intermittent tachycardia and increasing shortness of breath requiring increases in the fraction of inspired oxygen up to 40%. Blood tests showed worsening lymphopenia, with increasing levels of CRP. A repeat chest X-ray showed a right basal effusion, which was drained, guided by ultrasound scan. A total of 1.2 l of haemorrhagic fluid was drained, which was classified as a complicated para-pneumonic effusion with no pus; no organism was grown on culture. His chest X-ray 48 hours after admission was dramatically different to that on admission (Fig 3).

CXR performed 48 hours after admission.
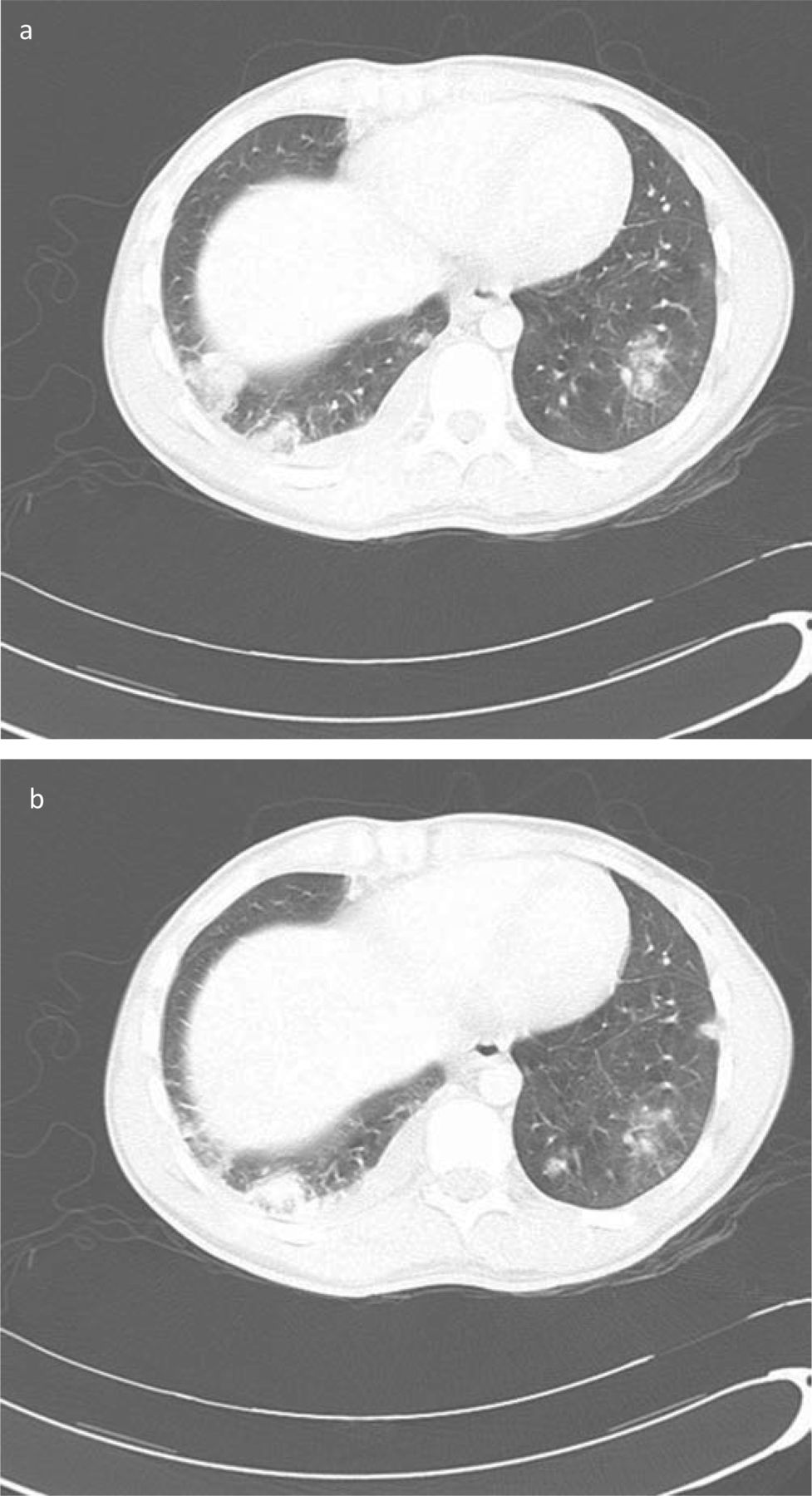
Forty-eight hours after he was admitted, the admission blood cultures grew a methicillin-sensitive Staphylococcus aureus (MSSA); antimicrobial sensitivity also included flucloxacillin, clarithromycin and rifampicin. Intravenous flucloxacillin was started at a dose of 1 g every six hours to treat this community-acquired pneumonia. Repeat CT of the thorax showed increasing pulmonary soft tissue nodules, some of which were developing into cavitations and worsening bilateral pleural effusions (Fig 4).
CT scan of thorax performed on day three.
Other organisms were also excluded; three sputum smears were negative for acid-fast bacilli and influenza A (H1N1), with no growth of microbes in the pleural effusion. A urine test was negative for legionella and pneumococcal antigens. Serology was negative for HIV, cytomegalovirus, Epstein-Barr virus and hepatitis. The patient was also negative for anti-neutrophil cytoplasmic antibodies and an autoimmune screen including anti-glomerular basement membrane antibody was also negative.
On the eighth day after admission, the Health Protection Agency notified the hospital that this patient's strain of S. aureus was positive for the Panton-Valentine leukocidin (PVL) toxin. Following microbiological advice, the patient was started on intravenous clindamycin, linezolid, rifampicin and immunoglobulins. He was treated in a side room, and staff and visitors had to wear personal protective equipment. A five-day course of octenidine-containing hypoallergenic antimicrobial hair and body wash (Octenisan) and mupirocin was also started for the patient and his household contacts.
Outcome and follow up
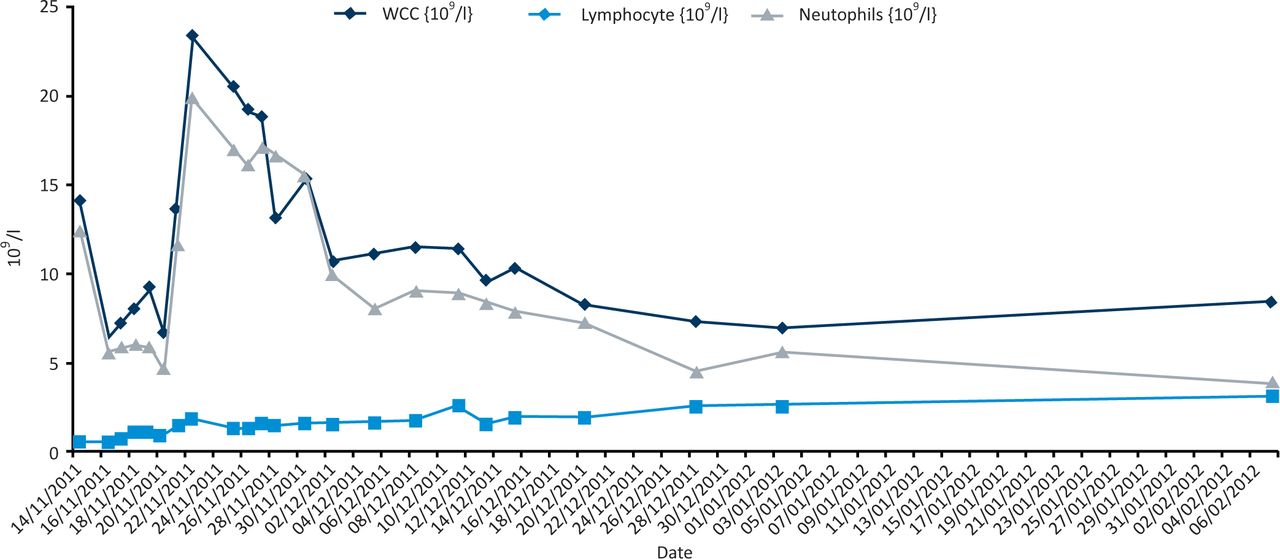
Once antitoxin treatment had been initiated, the patient's clinical condition significantly improved, as evidenced by a dramatic reduction in haemoptysis and stabilisation of his temperature and haemodynamic observations. His lymphocyte and total white cell counts also increased slowly, which suggests that the antibiotics were able to block the further breakdown of white cells (Fig 5). Fortunately he did not require extracorporeal membrane oxygenation (ECMO) or mechanical ventilation and was discharged six weeks later.
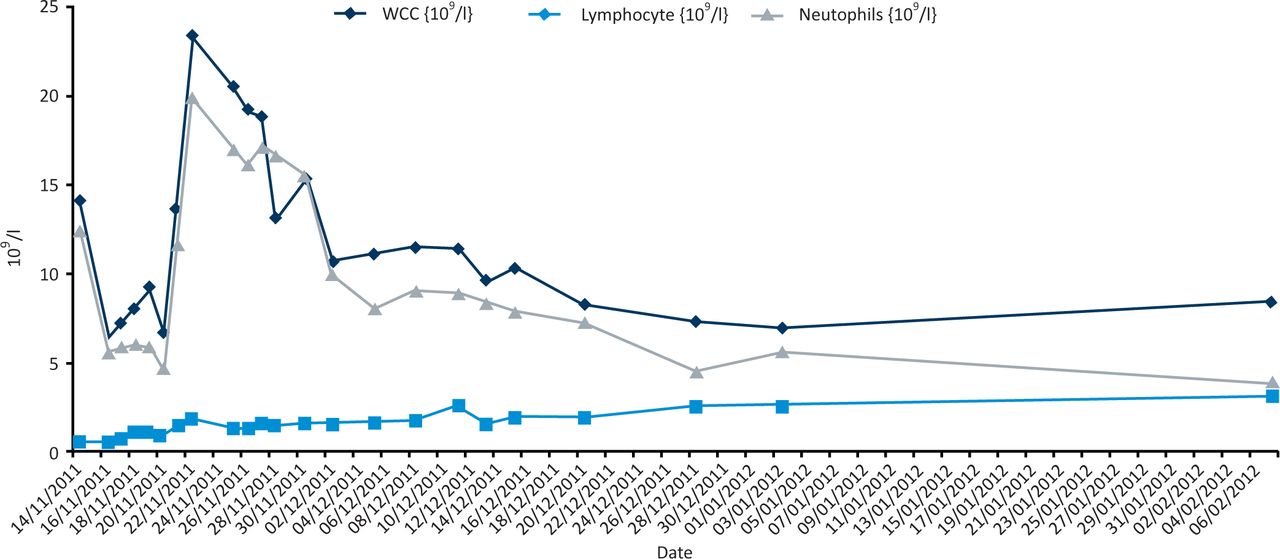
Trends in total white cell count, lympocyte count and neutrophil count in a patient diagnosed with necrotising haemorrhagic pneumonia.
Outpatient CT of the thorax seven weeks after discharge showed a reduction in the size of the effusions seen on the first CT scan of his thorax. Two small residual effusions with some pleural thickening were noted (Fig 6). The cardiothoracic surgeons reviewed the patient for potential lung decortication, but this was not required as he was clinically much improved.

CT scan of thorax performed seven weeks after discharge.
Four weeks later, a 42-year-old, female teacher from the same school presented with fever, rigors, cough, skin abscesses and myalgia. A chest X-ray showed subtle inflammatory changes in the left lower lobe and a very small effusion on a thoracic ultrasound scan. With a high index of suspicion, she was started on empirical treatment, and blood cultures were subsequently positive for PVL-producing S. aureus. She responded very well to clindamycin, linezolid and rifampicin, recovered much more quickly than the first patient and required no further intervention. As she was not in toxic shock, she did not require intravenous immunoglobulins. The local health protection unit was informed and performed a risk assessment at the school to screen for any further cases. The Stapylococcal Reference Unit at Colindale was able to perform DNA fingerprinting of the PVL-producing MSSA, which showed that two different strains were involved in the two patients. As of May 2012, no further cases have been reported from the school.
Discussion
Panton-Valentine leukocidin-producing S. aureus causes rapidly progressive, necrotising pneumonia, with mortality of up to 70%.1 Despite awareness that PVL-producing S. aureus causes mainly recurrent skin infections since 1932, a first case of necrotising pneumonia in the UK was described in 2003.2 Unlike S. aureus pneumonia seen in elderly patients with a number of pre-existing comorbidities, this PVL-producing strain of S. aureus tends to affect immunocompetent children and young adults. Although both of our cases involved MSSA, 47% of isolates have been found to be S. aureus resistant to methicillin (MRSA),3 so empirical treatment must cover for this possibility.
The true incidence of this isolate may not be clear. In 2002–03 in the UK, <2% of all S. aureus isolates were found to include the PVL strain, but it was found in 4.6% of S. aureus isolates from skin and soft tissue infections. In 2005, 224 cases in total were recorded, while this had nearly doubled to 496 in 2006. Whether this is a true increase or the result of better diagnosis and awareness is uncertain, but this strain is still not a notifiable disease. Furthermore, a post-mortem may not be performed in patients who die with severe community-acquired pneumonia, and lung specimens are not routinely cultured in those who do undergo post-mortem. However, the Department of Health is sponsoring two major projects to determine the prevalence of PVL-producing S. aureus in different settings.
Panton-Valentine leukocidin-producing S. aureus can arise from the transmission of blood-borne organisms from soft-tissue infections, but patients often have no skin changes.3 Instead, presentation is often preceded by a flu-like illness, as was seen in the first case. Clinically, patients tend to present with a triad of airway bleeding/haemoptysis, hypotension and non-specific findings such as a temperature of >39°C, myalgia, tachycardia, diarrhoea and vomiting.1 This triad was seen on our first patient's admission. Conditions such as vasculitis, pulmonary embolism and organisms such as Streptococcus pneumoniae and Mycobacterium tuberculosis may present with similar symptoms.
Routine blood tests will often reveal a very high level of CRP (>200 mg/l), which is rarely seen in viral infections. The white cell count may be within normal limits early in the illness, as toxins are only starting to be produced. However, marked leucopenia soon follows, as toxin production increases and the disease progresses due to an increase in local inflammatory mediators, which leads to destruction of lung tissue.4 Large areas of pulmonary infarction and haemorrhage occur, which appear on CT scans as cavitating lung lesions. Complications include septic shock and acute respiratory distress syndrome, which contribute to the high mortality.
The exact pathophysiology is not clearly understood, but it is suggested that the PVL toxin has an affinity for basement membrane of desquamated ciliated epithelium, which is able to pierce and destroy polymorphs, releasing proinflammatory cytokines. A preceding virus may impair the phagocytic activity of macrophages, allowing the unhindered replication of PVL-producing S. aureus.5
As this case demonstrates, routine antimicrobial treatment is not effective in treating necrotising pneumonia caused by community-acquired, PVL-producing MSSA. Indeed, the use of beta-lactam antimicrobials such as flucloxacillin as first-line therapy may increase toxin release,2 leading to further tissue necrosis and further clinical deterioration. Instead, first-line treatment should include antibiotics with an anti-toxin effect, such as linezolid or clindamycin plus rifampicin, with immunoglobulins if there is any suggestion of toxic shock. This regimen also provides cover for PVL-producing MRSA. Vancomycin is not recommended, as it does not produce a high enough concentration in the lung to kill the PVL-producing MRSA or to block the toxin.
Close contacts of patients with necrotising pneumonia also need to be screened and decolonised with antiseptic wash, as the disease is highly infectious. Infection control measures must be adhered to while the patient is nursed in a side room. Finally, once treatment is completed, all patients should be followed up and imaging repeated to assess improvement.
Conclusion
Necrotising cavitatory pneumonia secondary to PVL-producing S. aureus has very high mortality and morbidity, particularly in children and young adults. This diagnosis should be considered if a patient does not respond to first-line antibiotics and has clinical signs such as a temperature of >40°, heart rate >120 beats per minute, haemoptysis, lymphopenia and bilateral alveolar infiltrates/effusions. The patient should be monitored for skin manifestations, as PVL toxin is dermonecrotic. Airway bleeding, erythroderma and leucopenia are associated with fatal outcome. Clindamycin and linezolid switch off production of the PVL toxin, and linezolid is also active against MRSA isolates. Intravenous immunoglobulin (2 g/kg) may have a beneficial immunomodulatory action, especially in patients with toxic shock, neutralising superantigens and circulating toxins. Close contacts of patients with necrotising pneumonia must be screened and decolonised due to the high risk of transmission.
Acknowledgements
I thank Dr Marina Morgan, consultant microbiologist, Royal Devon and Exeter NHS Foundation Trust.
- © 2013 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.