
Abstract
Syncope is a major healthcare problem with significant morbidity, mortality and healthcare cost. It is a common symptom with a complex pathophysiology and, therefore, several aetiologies. Tilt-table testing (TTT) is an important, yet perhaps not widely-used, test that forms part of the management of syncope. We sought to assess the utilisation of this test in our institution for the investigation of patients with syncope, to study the referral patterns and the outcomes and usefulness of the TTT in a real-life setting. We undertook a retrospective study of all the TTT that were performed in our institution between January 2009 and October 2009. Of the 69 patients in which TTT was performed, 14 (20%) presented with presyncope, 24 (35%) with a single episode of syncope and 24 (44%) with multiple episodes. The average age was 57.2 years and 64% were female. Of the total patients, 35 (51%) had an abnormal TTT. Of the patients with normal TTT, four had internal loop recorders and six were referred to other medical specialities. The remaining patients (49%) had no formal diagnosis and were referred back to their general practitioner. TTT remains a common test modality and has great value when undertaken in the correct clinical context. This underlines the importance of a detailed clinical history. The European Society of Cardiology guidelines ensure a methodical and rational approach to syncopal patients and aide in choosing the right patient for the right test.
Introduction
Syncope and transient loss of consciousness (T-LOC) are a common presenting complaint in the acute medical ward and in other medical and cardiology clinics. The European Society of Cardiology (ESC) 2009 guidelines on the management of syncope1 encompass syncope within a larger framework of T-LOC (Box 1). Therefore, T-LOC is a term that applies to all causes of loss of conscious that are self-limiting, irrespective of cause. T-LOC syndromes are characterised by rapid onset and short duration with a spontaneous and complete recovery. However, syncope has an additional feature of transient global cerebral hypoperfusion (Box 2). There are several causes of syncope (Box 3).

Investigations of syncope and T-LOC are varied, depending on the symptoms. There are several investigations that can be undertaken to exclude common causes of syncope. If these tests fail to determine a diagnosis, the patient is often referred for further specialist tests, such as tilt-table testing (TTT).
TTT was first introduced into clinical practice by Kenny et al in 19862 and remains a pivotal modality for the investigation of syncope in appropriate patients. The ESC guidelines suggest various indications for this test (Box 4), where its diagnostic yield can be high. TTT are generally performed in patients where all the baseline tests have been reported as negative and the history is suggestive of a vasomotor origin. However, despite these guidelines, one often finds that TTT are requested as part of a routine test for patients with syncope, therefore subjecting patients to an unnecessary, and potentially unpleasant, test. TTT in these inappropriate patients would, not surprisingly, be negative.
Our aim was to audit the use of TTT in our institution, to study the referral pattern and the outcomes of this test.
Methods
To audit the use of TTT in our institution, we undertook a retrospective study of all the tests that were performed in our institution between January 2009 and October 2009. We set out to study the referral patterns, outcomes and usefulness of TTT for the diagnosis of syncope.
The protocol used for TTT in our institution is based on the 2004 protocol by Brignole et al.3 The test is performed in a quiet room that is equipped with a resuscitation trolley. The patient lies supine on a Tilt couch (Akron Streamline, Arjo Huntleigh Ltd, Gloucester, UK). The test begins with a pre-tilt supine position with the patient laying still for 5–20 min and then at a tilt of 60° for approximately 20 min. If there has not been any change, a carotid sinus massage (CSM) is performed at this time. The patient is then brought back to the supine position and is maintained for another 20 min, following which another CSM is performed. During the test, the patient is monitored with the Task force 3040i Monitor (CN systems, Graz, Austria). The endpoints are either induction of syncope or completion of planned test.
We obtained the data from clinical and electronic notes, the referral letter and, where appropriate, the general practitioner. This audit was registered and approved by the audit department of our institution.
Results
Over the 10-month period, 69 patients underwent TTT in our institution. The age range was 18–86 years of age (average 57.2, median 67) (Fig 1). More than half (64%) of the patients were female. Most patients (72 %) were referred by cardiologists, with 28% patients being referred by other hospital-based medical specialties, mainly the care-of-the-elderly team.
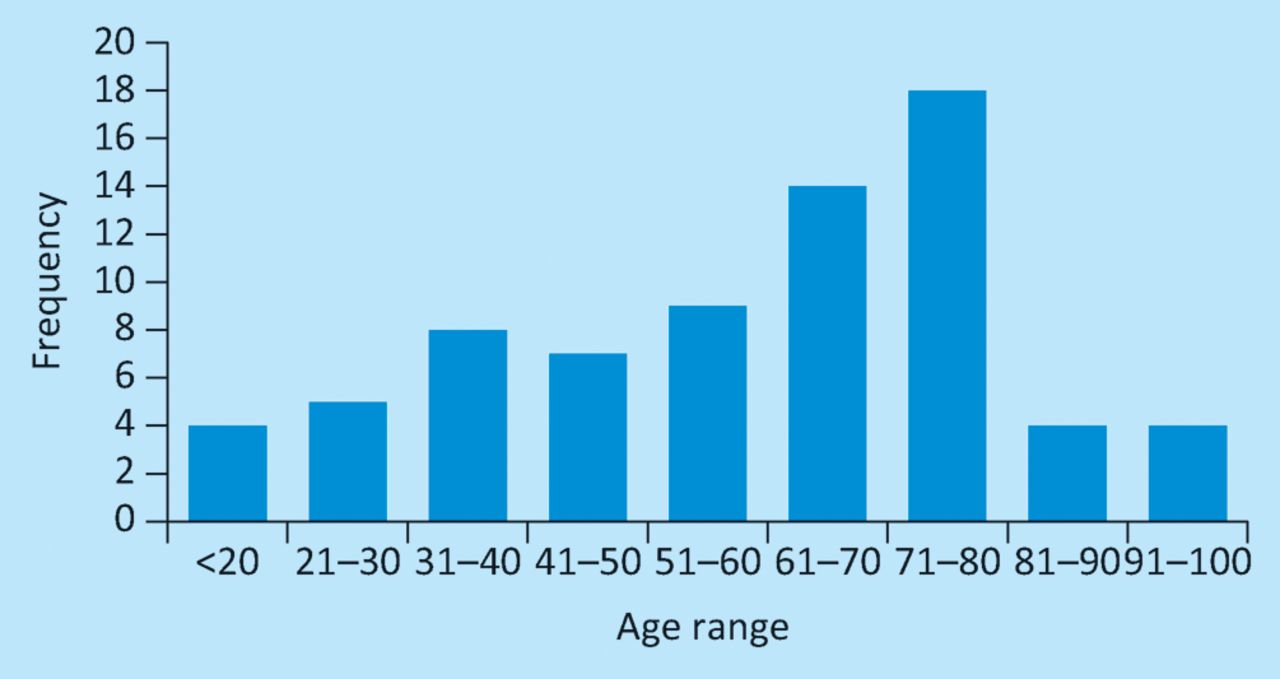
Frequency of age range of patients.
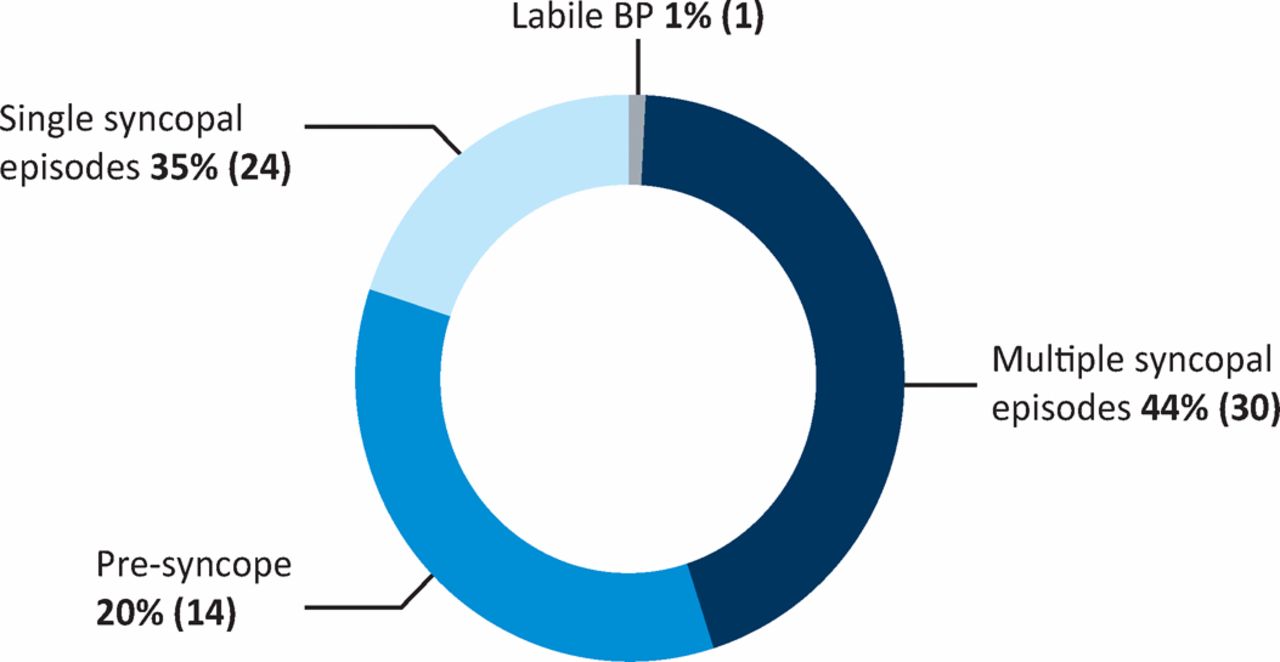
Of the 69 patients, 30 (40%) had had multiple episodes of syncope, 24 (30%) had had a single syncopal episode and the remaining 14 (20%) had presyncope or dizzy spells without loss of consciousness (Fig 2). Most of the patients had several other tests performed in addition to TTT. These included 24-h Holter monitoring, computerised tomography (CT) scan, magnetic resonance imaging (MRI) scan, transthoracic echocardiogram (ECG), short Synacthen° test, electroencephalogram (EEG) and implantation of an internal loop recording device. By contrast, 12 patients had a TTT only.
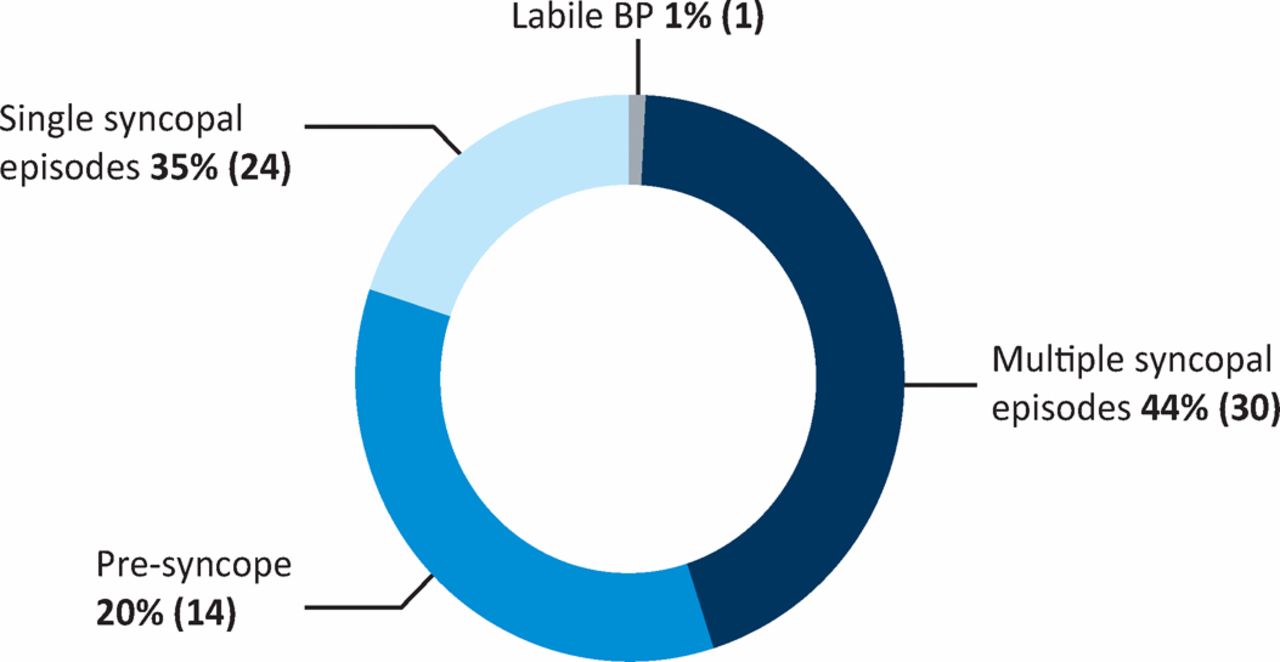
Patient presentation. BP = blood pressure.
Of the 69 patients, 35 (51%) had an abnormal result. Of these, five (14%) had prolonged asystole on CSM, two (6%) had an abnormal response to CSM without asystole, 10 (28%) had a mixed vasodepressor response, seven (20%) had a haemodynamic profile consistent with autonomic dysfunction (AD), three (9%) had features of postural orthostatic tachycardia syndrome (POTS), four (11%) had a significant cardioinhibitory response, three (9%) had symptoms with low blood pressure and one (3%) had psychogenic collapse. The remaining 34 patients (49%) had negative tests and no formal diagnosis (Fig 3 and 4).
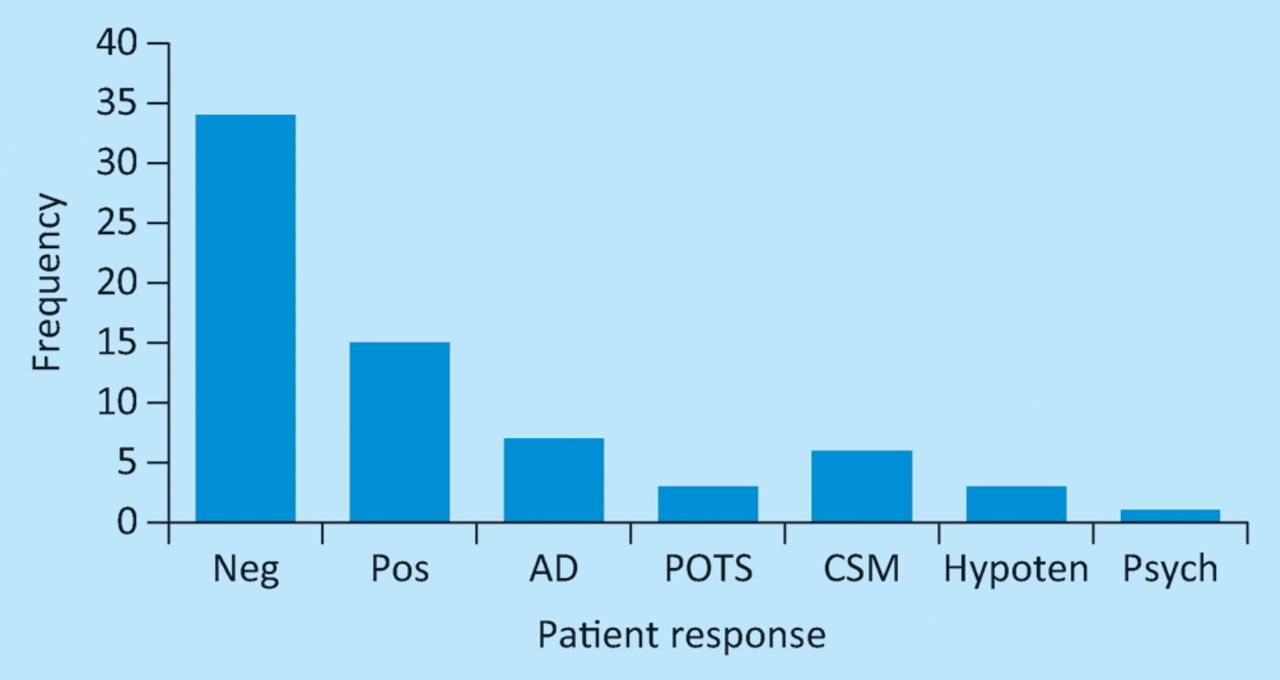
Patient response on tilt-table test. AD = autonomic dysfunction; CSM = carotid sinus massage; Hypoten = hypotension; Neg = negative test; Pos = positive test; POTS = postural orthostatic tachycardia syndrome; Psych = psychogenic.
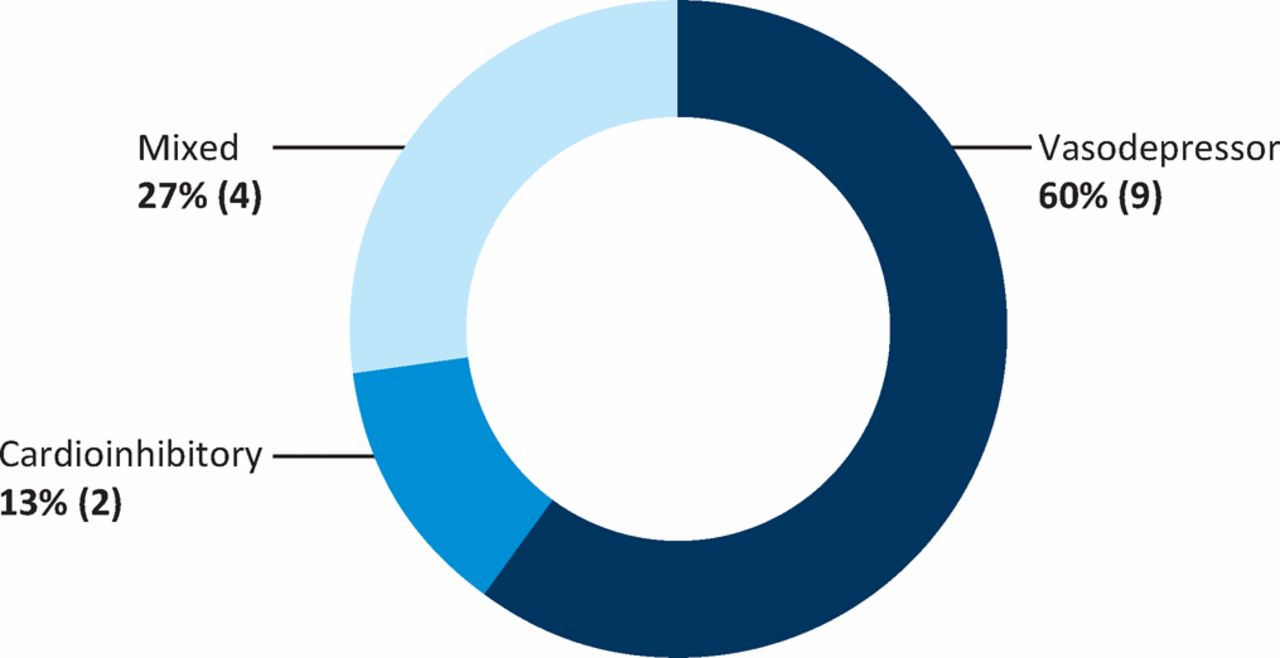
Type of positive response
Nine patients went on to have permanent pacemakers fitted. These were the four patients with cardioinhibitory response on TTT and five patients who had had significant asystole on CSM. The remaining 26 patients who had a diagnosis were either treated symptomatically or were referred to physiotherapists or occupational therapists. Of the 34 patients without a formal diagnosis, four had internal loop recorders fitted and six were referred to other medical specialities (including care of the elderly, physiotherapists, and neurologists) for further investigation. The remainder were referred back to their general practitioner with no abnormalities noted.
Discussion
Syncope is a common presenting complaint across Europe, accounting for 1% of all emergency department referrals, of which 40% are admitted with a median length of stay of 5.5 days.4–9 In the UK, the average cost per patient per admission is £611, with 74% of the cost attributed to hospital stay.10 In the USA, the mean cost of syncope and syncope-related admissions derived from the Medicare database is US$5,400 per hospitalisation.11
Besides the economic issues, syncope also has a significant impact psychosocially and on the patients’ quality of life. Patients with recurrent syncope scored a 33% adverse effect on the disease-specific Syncope Functional Status scale, with a reduction in mobility and self-care, and an increase in depression and pain.12 The further reduction in quality of life was worse in patients with more comorbidities, female sex, increasing age and a greater number of presyncopal and syncopal episodes.12
Different tests are available to investigate the possible causes of syncope. These tests include ECG, 24-h Holter monitoring and prolonged cardiac monitoring, with devices such as the cardiac memo and the implantable loop recorder. Owing to the number of possible causes of syncope, several tests are available that can be used to aid diagnosis. There is currently no gold standard test that could yield a diagnosis. However, blanket testing for each cause of syncope could theoretically lead to increased cost and inappropriate use of medical resources. This highlights the need to follow a standard pathway to ensure that only the appropriate diagnostic test is performed, not only to decrease costs, but, more importantly, to also obtain an accurate or reliable diagnosis.13 Detailed patient history is essential to guide the physician towards the appropriate system for investigation. If the features are typical of neural- and/or reflex-mediated syncope, often no tests are required, unless there are significant high-risk implications, such as for HGV drivers or airline pilots.1
TTT was first introduced into clinical practice by Kenny et al in 1986 for the evaluation of syncope of unknown origin.2 It is usually carried out to confirm the diagnosis of neurally medicated syncope.14–16 TTT has been suggested to be a useful tool in discriminating syncope from epilepsy,17 syncope from falls in older patients18 and even in patients where a psychological element is suspected.19 TTT can also be useful in discriminating pure neural-mediated syncope from atypical forms of delayed orthostatic hypotension.20 However, it is important to appreciate that a negative TTT does not exclude the diagnosis of neurally mediated syncope.
The end response is usually classified as either vasodepressor with hypotension, cardioinhibitory with asystole or a mixed response21 (Table 1). However, this does not necessarily translate into a patient only having either of these as the cause of their symptoms. For example, a patient with a vasodepressor, mixed or even a negative TTT could still have asystole during a syncopal episode.22,23
Positive responses on tilt-table testing using the VASIS classifications.21
If we consider normal physiology, gravity pools blood from the thoracic cavity into the lower limbs when one stands up from a supine position. This phenomenon is offset by physiological mechanisms that compensate and enable continued cerebral blood flow, thereby preventing syncope. These compensatory mechanisms are neurohumoral, neurovascular and the so-called ‘muscle pump’. Collectively, these interact to maintain blood pressure and, therefore, cerebral blood flow. TTT takes advantage of this pathophysiological mechanism by reproducing a neurally mediated reflex in the cardiac physiology laboratory by pooling blood to the lower limbs, causing a decrease in venous return, which in turn causes hypotension that might be accompanied by bradycardia and impaired vasoconstriction. This is compounded by vagal overactivity and withdrawal of sympathetic tone in certain patients.22
The yield of the TTT can be enhanced with use of CSM, especially in those patients aged 80 years or above with no cardiovascular or neurological complications. Indeed, it has been suggested that TTT and CSM should be included in a comprehensive work up for patients with a history of syncope and/or falls if no diagnosis has been made.23
There are several TTT protocols, one that uses no provocating agents, and others that use isoprenaline, nitroglycerine (GTN), clomipramine or edrophonium as provocating agents. Use of provocating agents such as isoprenaline or GTN is thought to increase the yield of the test, with high specificity (92–94%) and positive rates (61–69%) being observed with provocating methods.24–26
One of the first TTT protocols from Westminster Hospital London used no provocation agents and was solely done with the use of a footboard set at 60°. This was named the Basal or Westminster protocol, with patients supported at an angle of 60° for 45 min, and was found to have a sensitivity and specificity of 75% and 93% respectively.27 The duration of the TTT was questioned by Stein et al who analysed results from 11 published TTT studies using the Westminster protocol and compared the results with 213 patients that then performed a TTT for 30–60 min. The authors found that diagnostic accuracy was not significantly increased with the duration of the TTT lasting more than 30 min.28
GTN is the most commonly used provocating agent, with a reported sensitivity and specificity of 62% and 92% respectively.29 Other agents that have been used include isoprenaline,30–33 clomipramine34,35 and edrophonium.36
Furukawa et al37 assessed whether different provocating agents would affect the TTT response. They found that use of a provocating agent was likely to make the test positive. They also found that a cardioinhibitory response seemed to be observed more frequently if clomipramine was used as a provocating agent and vasodepressor, and mixed responses seemed to predominant if GTN was used. However, they did not recommend using any agent over the other.
In our study, 49% of (34/69) of patients had no formal diagnosis at the end of their investigations. Kapoor et al38 recognised the difficulties in diagnosing the cause of syncope, with 45% of patients in this retrospective study having no diagnosis. Further studies showed similar results in intensive care units,39 within institutionalised older patients40 and for patients admitted with syncope,41 with only 47%, 31% and 39% of syncopal patients having a firm diagnosis, respectively. However, the diagnostic yield can be as high as 98% with 50% diagnosis during initial evaluation involving history, clinical examination and standard ECG.1 Acute admissions and inpatients stays were reduced as were the number of appropriate tests when adhering to ESC guidelines.5 The use of TTT and CSM diagnosed neural syncope in 24% of patients with previously unexplained syncope. This study in a teaching hospital of 200 patients aged 65 years or older with previous unexplained falls also reported that 26% of patients with syncope remained undiagnosed.42
Investigative patterns for syncope vary from institution to institution. This partly depends on local expertise. Brignole et al43 noted that 38% (17) of patients who presented with faints had no formal diagnosis. In their cohort, only 7% of patients had TTT, which is less than would be expected, yet a higher than expected number of patients had imaging and neurological referrals. Their cohort also had a few patients (3%) receiving an implantable loop recorder. In our cohort, 10% of patients were referred to a neurologist and 6% of patients received a loop recorder.
With the development of a faint algorithm, Daccarett et al44 performed a retrospective study of 254 patients presenting with faints. They were programmed into the algorithm and compared with what the actual outcomes were. The faint algorithm suggested that there would have been a 52% reduction in admission rates without a statistical difference in serious event within 7 days. This perhaps illustrates the need for a more standardised approach.
Finally, although no deaths have been reported during TTT, which is a safe albeit uncomfortable test, the ESC guidelines recommend that resuscitation equipment should always be available during TTT.1 The main complications are of syncope, whether cardioinhibitory, vasodepressor or a mixed response. These are endpoints and suitable resuscitation equipment should be immediately available.
Treatment of syncope is dependent on cause. Lifestyle, physical counter-pressure manoeuvres (PCMs), pharmacological and pacing have all been tried in treatment of reflex syncope (REF). Lifestyle changes would include avoidance of situations that could precipitate a syncopal episode, advising the patient to stay well hydrated and to take caution with medication that might cause hypotension or bradycardia.45
Leg crossing or arm gripping have been shown to be effective in treating REF.46,47 These PCMs cause an increase in blood pressure that is able to either delay or avoid syncope. A multicentre prospective study assessed the effectiveness of PCMs on patients with recurrent REF and found a significant improvement in symptoms and a decrease in syncope burden.48 There were no adverse events reported in patients trained with PCMs.
Tilt training has also emerged as a possible treatment for recurrent vasovagal syncope that can be triggered by orthostatic stresses.49–52 A proposed tilt training regimen includes patients standing twice daily for up to 30 min, leaning back onto a vertical wall with their feet 15 cm from the wall. The guidelines also recommend a family member to be present.1 Alpha-adrenoceptor agonists have also been tried as pharmacological agents to prevent or reduce symptoms associated with vasovagal syncope. Etilefrine was not found to be superior to placebo in preventing these attacks.53,54 By contrast, midodrine has been shown to be effective in preventing vasovagal syncope and in reducing the symptoms associated with it.55–57 A recent meta-analysis of the use of alpha-adrenoceptor agonists for the treatment of vasovagal syncope also confirmed a role for these drugs, with midodrine being more superior compared with etilefrine.58
Finally, the use of pacemakers in REF has been studied in five multicentre randomised trials.59–63 The results were mixed. However, an earlier meta-analysis of all these studies suggested a nonsignificant reduction of symptoms.64 More recently, the International Study on Syncope of Uncertain Aetiology (ISSUE-3)65 demonstrated that dual chamber (DDD) pacing can significantly reduce syncope in patients over 40 years of age with severe asystolic neurally mediated syncope.
Our study is a retrospective audit of our practice. Given that much of the information came from the medical records, it has inherent limitations, because the quality of the data depends on the quality of the record keeping. However, we did contact the general practitioners for more information if we felt that any data was missing. Another drawback of the study is that we only investigated patients who were referred for TTT. We did not look at patients presenting with syncope to the institution to see how they were managed. Perhaps this would need investigating with another audit of our practice.
To keep up with the audit cycle, we have educated the physicians to the latest ESC guidelines on the management of syncope and we hope that future audits will show a better adherence to these guidelines. In this day and age of financial constraints, such specialised tests should be restricted to patients who fulfil the criteria for the tests.
Conclusions
Syncope is a common symptom with a complex pathophysiology and several possible aetiologies. TTT remains a valid cornerstone test modality for syncope and should be considered in patients that have had several unexplained falls, to test for the susceptibility of REF and to discriminate between orthostatic hypotension and REF. The test could also be considered in syncopal patients who are seen to have twitching, to discriminate from epilepsy. However, TTT should not be used for patients with a single syncopal episode unless there is a clinical need to demonstrate susceptibility of REF, differentiation of REF and orthostatic hypotension or, finally, to differentiate between jerking movements owing to syncope or to epilepsy. However, great emphasis must be placed on the interpretation of TTT relevant to the symptoms of the patient.
Treatment should be based on patient reassurance, education and lifestyle modifications. Pharmacological therapy has not proved to be of benefit and pacing should be considered in selected patients that have documented asystole.
Unfortunately, many patients are either overinvestigated with blanket tests or underinvestigated, resulting in a large percentage of patients labelled with unexplained syncope. This underlines the need for a detailed patient history and adherence to ESC guidelines.
- Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.