
New treatments and strict specifications about how care should be organised have dramatically advanced stroke medicine over the past 5 years. This progress is built upon an evidence-based national audit organised by the Royal College of Physicians and has led to the emergence of stroke medicine as a distinct medical specialty. Here, I report on the conference marking the halfway point in the Government’s 10-year stroke strategy.
Damien Jenkinson, the national clinical lead for the NHS Stroke Improvement Programme, started by outlining the importance of targets. The ‘vital signs’ used for stroke, such as the amount of time spent on a stroke unit and the 24-hour target for specialist assessment of transient ischaemic attacks (TIAs), have been pivotal in concentrating the minds of all those trying to improve services. Since the start of the National Stroke Strategy, there has been a 30% fall in mortality nationwide. In London, where there has been wholesale service redesign, survival has improved at a greater rate than in the rest of the country. Even though the London stroke model needed significant investment, evaluation has demonstrated that the improved service is cost-effective by 90 days post stroke. Dr Jenkinson reported, however, that the Care Quality Commission was still finding significant problems with post-hospital care in many areas and that a new consensus statement on community stroke care was due to be published shortly.
Political environment
Dr Matt Fay, a Bradford general practitioner (GP) who is national clinical lead for atrial fibrillation, outlined the new commissioning structure. He explained that the Clinical Commissioning Groups (CCGs) would be judged on the achievement of NICE quality standards. In questions, it became apparent that very few members of the audience were yet involved with CCGs and that there was uncertainty as to which CCGs would take responsibility for stroke and therefore problems knowing who to talk to. Dr Fay had serious qualms about the transition to the new system, which had not been well planned, causing de-skilling of Primary Care Trusts (PCTs), loss of support from stroke networks and the possibility of stroke moving lower down the commissioning agenda. Physician advocacy will be crucial in maintaining momentum because those who shout loudest will probably be heard. We were urged to: ‘learn how to use the acronyms and befriend a GP’.
Fourth edition National Clinical Guidelines for Stroke launched
Prof Tony Rudd, chair of the Intercollegiate Stroke Working Party, introduced the fourth edition of the National Clinical Guidelines for Stroke, which were to be launched that day, as mandatory reading for every stroke physician. Unlike previous editions, the new guidelines include recommendations on rehabilitation as the NICE guidelines on this have been delayed. They set challenging targets that will mean a change of practice even in high-achieving units. The most pertinent for me were:
patients with TIA or minor stroke and atrial fibrillation should be anticoagulated with an agent that has rapid onset in the clinic
patients with confirmed TIAs should receive immediate treatment with an antiplatelet drug and statin
carotid surgery should be performed within 7 days (reduced from 14 days previously)
brain imaging after stroke should be undertaken within a maximum of 12 hours (down from 24 hours previously)
indications for thrombolysis should be revised as discussed below following the publication of the Third International Stroke Trial.1
There was, however, some reassurance to prevent clinical practice running ahead of research evidence:
intra-arterial thrombolysis and perfusion scanning should take place only within clinical trials
screening or surgery for asymptomatic carotid stenosis should not be performed routinely.
Avril Drummond, professor of healthcare research at the University of Nottingham, focused on rehabilitation. She emphasised that rehabilitation should be like the cream in a black forest gateau: integrated into the structure. It should not be seen as the job of one particular profession but should pervade the culture of the whole team. Prof Drummond outlined some of the problems in getting clinical trials on rehabilitation published, especially those with negative results, but emphasised how important it is to increase the evidence base. She also discussed the controversial target that every patient should have 45 minutes rehabilitation provided by each relevant specialty daily, explaining that the philosophy was to give patients much more treatment than at present. She commented that it is unacceptable that many stroke patients still spend much of the day doing nothing. Compared with Italy, France, Switzerland and Germany even this 45 minute target is conservative. To increase therapy to patients, Prof Drummond commented that we need to reduce excessive paperwork and maximise the amount of time patients spend doing meaningful activity. The recent ACTNoW trial2 showed that intelligent non-professionals can provide treatment that is as good as that provided by professionals in certain circumstances. We should find ways to introduce this practice more widely.
In answering a number of specific questions, Prof Rudd pointed out that it was important that guidelines should be interpreted by skilled expert professionals. Although they apply to 80% of patients 80% of the time, the role of professionals’ individual decisions in stroke care was still paramount.
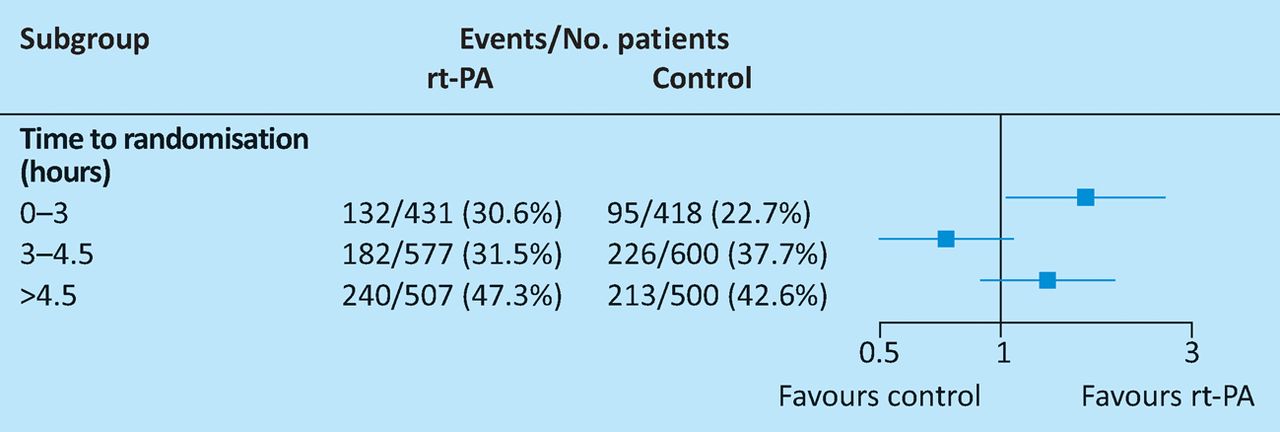
Graham Venables, national coordinator for the Third International Stroke Trial (IST3), reviewed the history and evidence base for thrombolysis in stroke. Analysis of the most recent data from IST3 confirmed that the most important variable for success is onset-to-treatment time (Fig 1).1 Our efforts should be aimed at reducing this however we can, including raising public awareness and reducing door-to-needle time in hospital. The data show that it is safe to thrombolyse people over 80 years of age, but that those with severe strokes remain at high risk. Many older people would, however, rather have the chance of disability-free survival even if that meant an increased risk of early death. It is therefore important that consent should be geared to the individual and that changes to local thrombolysis protocols should go through an appropriate clinical governance framework. The audience raised the usual controversial topics, including weighing patients and treating wake-up strokes, people with diabetes or those with posterior circulation strokes. Prof Venables stressed that none of the relative contraindications are more important than treating all appropriate patients rapidly.
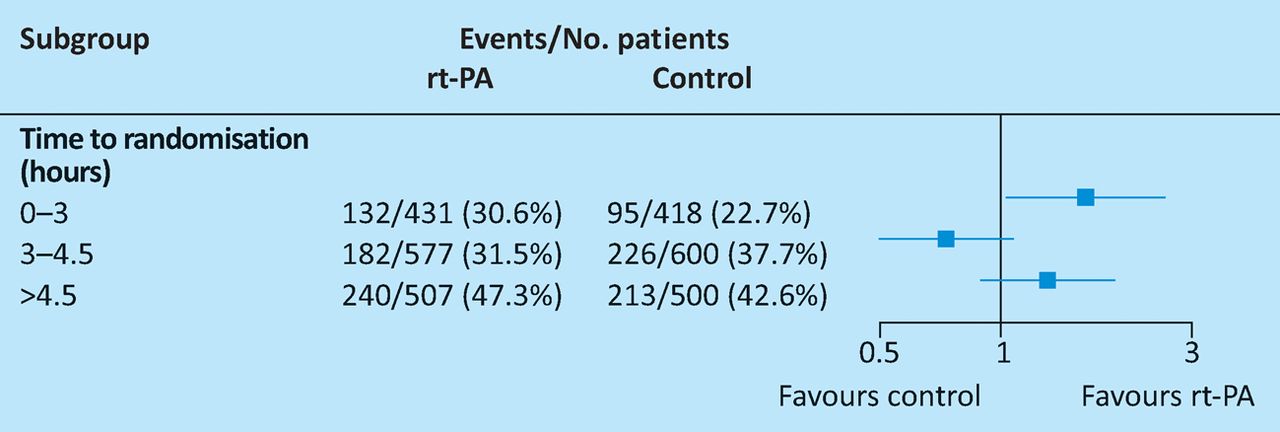
Effect of treatment with recombinant tissue plasminogen activator (rt-PA) on the primary outcome of Oxford Handicap Scale 0, 1 or 2 in patients by time to randomisation adjusted for age and baseline NIH Stroke Scale. Odds ratio (boxes) with 99% confidence intervals (horizontal lines). Reproduced with permission from Sandercock et al (2012).1
Imaging
Joanna Wardlaw, professor of applied neuroimaging at the University of Edinburgh, reminded us that imaging is there to answer clinical questions. The most obvious are: ‘Is this event vascular or non-vascular?’ and ‘Is this stroke ischaemic or haemorrhagic?’ A further emerging question is: ‘What sub-type of stroke is this?’ Magnetic resonance investigation of TIA or minor stroke should always include gradient echo sequences to look for evidence of past haemorrhage. Prof Wardlaw also pointed out that diffusion-weighted imaging can be positive in some stroke mimics and negative in some genuine strokes or TIAs. For carotid imaging, whichever modality gives the fastest answer locally should be used.
Early supported discharge (ESD)
Helen Rogers, professor of stroke care at Newcastle University, started by surveying the audience and found that 60% had an early supported discharge (ESD) service and that the majority would like one for themselves or their relatives. Community rehabilitation empowers patients and carers, leads to less isolation and emphasises psychological and social recovery. It does, however, increase carer stress and primary care workload and so it needs to be coordinated and started immediately after discharge. The intensity of therapy at home during ESD should be the same as it would have been had the patient remained in hospital. Although the Sentinel Audit showed that 60% of services claimed to have ESD, there was concern that some of these might be re-badged generic services, in the same way that many early stroke units were re-badged as geriatrics wards. Clinicians and patients should refuse to be fobbed off with these. Randomised controlled trials are being set up to look at extended rehabilitation services post-ESD and Prof Rogers encouraged the audience to consider taking part.
Patient and public involvement
Margaret Goose, member of the Patient and Carer network at the RCP, introduced herself and her long history of championing patient and public involvement (PPI) in stroke. She pointed out how difficult it was for patients to accept being ‘discharged’ and urged us all to use the phrase ‘transfer of care’, reminding us that professional input should not finish with hospital discharge. Dr Goose likened the doctor–patient relationship to a dance where only one partner (the doctor) knows the steps and can hear the music: we should make sure that our patients have been taught the steps and can also hear the music. She introduced Healthwatch (www.healthwatch.co.uk), which is the new statutory body that champions patients’ concerns. Her tips for successful PPI emphasised the need to ensure that we produce outcomes that are important for patients as well as ticking professional boxes (Table 1). Chris Clarke, of the Stroke Association, emphasised how important it is to avoid or explain professional jargon.
Tips for successful patient and public involvement.
Stroke units still crucial
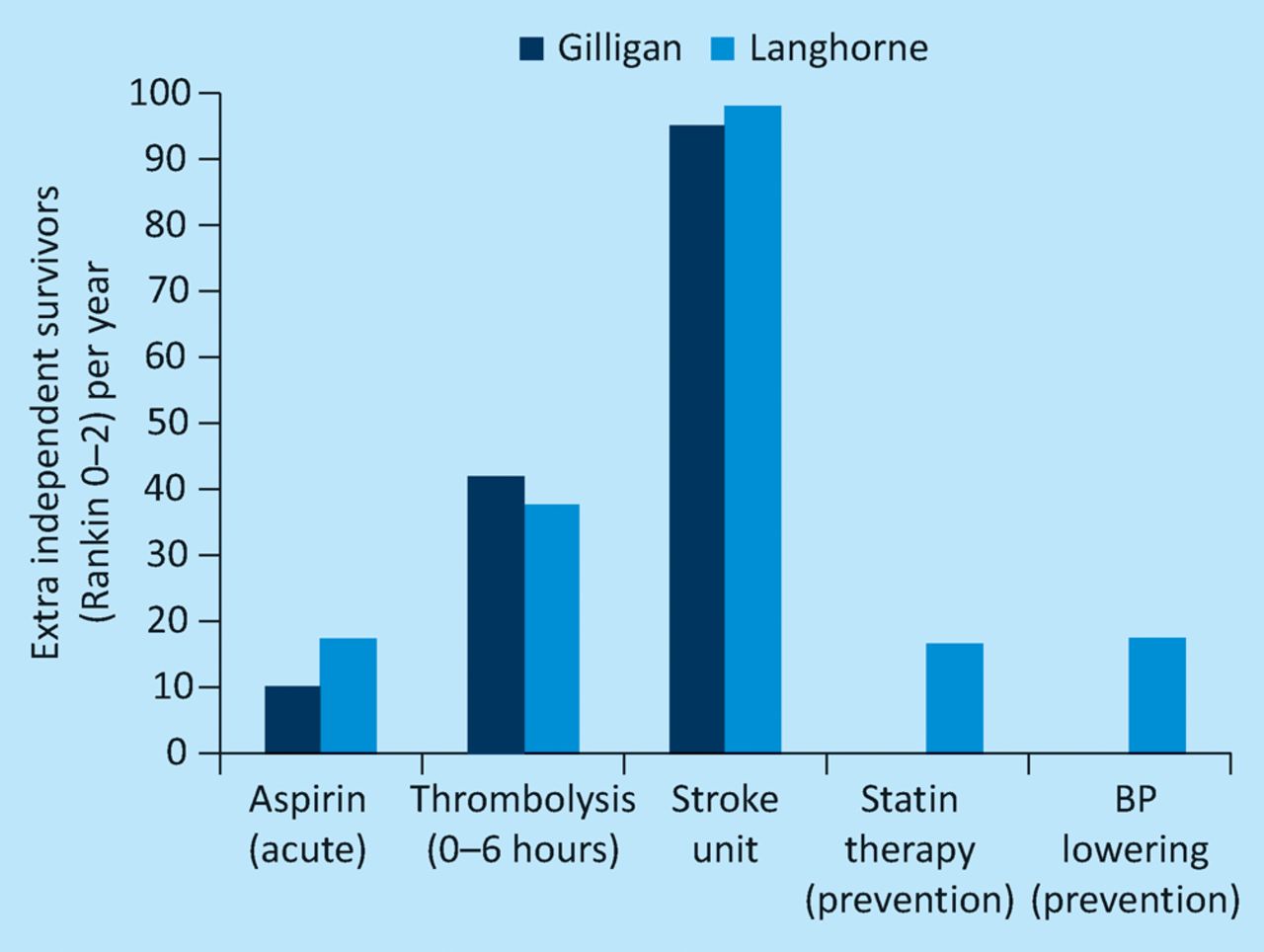
Peter Langhorne, professor of stroke care at the University of Glasgow, reminded us of the evidence around stroke units and how, when compared with thrombolysis, admission to a stroke unit almost doubles the number of independent survivors per year (Fig 2). Audit had demonstrated that although the structure of our units was good, the process (ie the delivery of care) was not always so good and there was room for improvement. A large cluster randomised controlled trial in 20113 had shown that the pointers to good care were:

adequate staffing
training and education of staff, especially nurses
team building
protocols for key aspects of care
research on implementation.
Prof Langhorne was also concerned lest future service developments undo the gains we have achieved.
Staffing and 24/7 care
Caroline Watkins reminded us that we have to provide high-quality stroke care 24/7. She introduced the Stroke Specific Education Framework (www.stroke-education.org.uk) and explained how recommendations on staffing levels had been calculated using a bottom-up approach. Tables could be used to compare local staffing levels with recommended figures. The website also lists training courses that have been endorsed by the UK Stroke Forum. Those setting up training should use this framework to look for good courses locally and to submit their own for approval.
- Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.