
Key points
Hypercalcaemia is most commonly caused by primary hyperparathyroidism or malignancy
Measuring parathyroid hormone levels is most important in deciphering the underlying diagnosis
Classical symptoms of hypercalcaemia become more apparent as serum calcium concentrations approach 3 mmol/l or if a rise occurs over a short duration
The first step in the management of severe hypercalcaemia is the restoration of euvolaemia
Subsequent treatment of hypercalcaemia is most effective if directed at the underlying pathology
Background
Mild hypercalcaemia is common and is often detected as a coincidental observation on blood testing for an unrelated reason. Severe hypercalcaemia, usually considered to be a serum calcium measurement of >3.5 mmol/l, is a medical emergency with life-threatening consequences. It is important for clinicians in primary, secondary and emergency care to be familiar with the diagnosis, management and underlying causes of hypercalcaemia. There is an initial ‘uniform’ approach to the treatment of acute severe hypercalcaemia (of all causes), but the underlying cause of the hypercalcaemia must be established to provide optimal longer-term management. A clear understanding of physiological calcium regulation along with a handful of associated and relevant blood test results allows determination of the underlying cause of hypercalcaemia in all but the most idiosyncratic cases.
Control of serum calcium
Maintenance of normal calcium levels is under tight regulation by parathyroid hormone (PTH) and vitamin D (Fig 1).1 PTH is secreted by the parathyroid glands and its overall effect is to increase serum calcium and activated vitamin D, and to lower phosphorus levels.1 The calcium-sensing receptor (CaSR) on parathyroid cells is activated by extracellular calcium to inhibit PTH release.2 Vitamin D is synthesised from cholesterol in the skin in response to sunlight and activated in the liver to 25 hydroxyvitamin D (25-OHD), and in the kidney to the active form 1,25 dihydroxyvitamin D (1,25-(OH)2 vitamin D).1 Calcitonin is produced by the C cells of the thyroid; it acts to inhibit osteoclast resorption and promotes calcium and phosphate excretion, but is of little relevance to hypercalcaemia clinically.
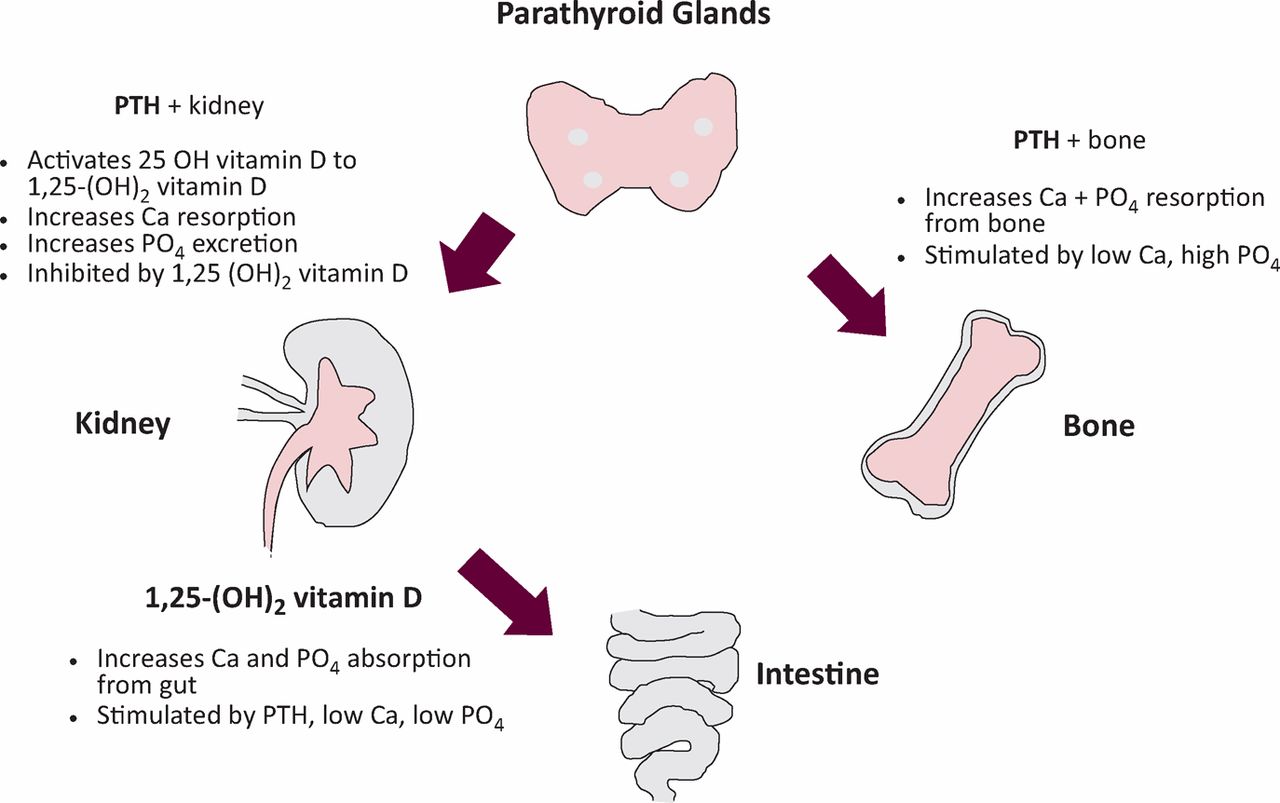
Calcium homeostasis. End organ effects of parathyroid hormone (PTH) and vitamin D (1,25 (OH)2 vitamin D). 1,25-(OH)2 D = active vitamin D; Ca = calcium; PO4 = phosphate; PTH = parathyroid hormone.
Clinical presentation of hypercalcaemia
Milder degrees of hypercalcaemia (<3.0 mmol/l) are usually not associated with symptoms if the rate of rise has been slow. Polyuria and polydipsia represent nephrogenic diabetes insipidus,3 while neurological and muscular manifestations of hypercalcaemia are due to increased depolarisation thresholds in cell membranes. Mild tiredness through to obtundation and coma represent the spectrum of neurological manifestations of hypercalcaemia. Owing to the lack of specificity of presenting clinical features of hypercalcaemia, it is necessary to have a high index of clinical suspicion and to request a measurement of serum (or ionised) calcium to establish the diagnosis.
Total serum calcium results should be adjusted for serum albumin:4
Adjusted calcium (mmol/l)
= serum calcium
+ [(40 – plasma albumin in g) × 0.02].
Worked example: for calcium 2.60 mmol/l and albumin 34 g:
adjusted calcium = 2.6 + [(40 − 34 = 6) × 0.02]
= 2.72 mmol/l.
It is not necessary to use adjustment if ionised calcium can be measured, but this is not available in all centres. Measurement of ionised calcium should be considered for patients with high calcium levels who are known to have circulating paraproteins, such as those with myeloma, because paraproteins interfere with calcium measurement.4
Determining the cause of hypercalcaemia
Primary hyperparathyroidism and malignancy account for around 90% of cases of hypercalcaemia (Box 1). With this in mind, the first investigation in hypercalcaemia is measurement of PTH, which will distinguish between these two most common causes. There might be specific clinical features that help to distinguish benign and malignant causes of hypercalcaemia before a PTH result is available (Table 2).
Symptoms and signs associated with hypercalcaemia.
Clinical features of primary hyperparathyroidism compared to malignancy-associated hypercalcaemia.
Hypercalcaemia with elevated PTH
In primary hyperparathyroidism, PTH is either frankly elevated or inappropriately normal (in up to 30%)7 in the setting of hypercalcaemia.8 There are two other disorders in which hypercalcaemia is associated with elevated or normal PTH – tertiary hyperparathyroidism and familial hypocalciuric hypercalcaemia (FHH).
Tertiary hyperparathyroidism occurs when PTH increases to maintain normocalcaemia in the setting of vitamin D deficiency; eventually parathyroid hyperplasia occurs and PTH secretion becomes independent of calcium levels. This is commonly seen in chronic kidney disease.
FHH is a disorder caused by mutations in the calcium – sensing receptor gene.6 A 24-hour urinary calcium or a calcium:creatinine excretion ratio can help identify these patients–calcium excretion is low in FHH. Genetic testing to detect mutations directly in CaSR is also now available.9 It is important to distinguish FHH from primary hyperparathyroidism as FHH does not require surgical intervention.
Most patients with primary hyperparathyroidism are diagnosed when hypercalcaemia is identified during blood tests for unrelated clinical indications.10 It is now rare for primary hyperparathyroidism to present with ‘classical’ symptoms and quantitatively severe hypercalcaemia (serum calcium >3.5 mmol/l).10
Hypercalcaemia with suppressed PTH
In malignancy-associated hypercalcaemia, PTH is suppressed. Hypercalcaemia of malignancy occurs in about 25% of cancer patients and can be caused by a number of different mechanisms outlined in Box 1.5
Granulomas express the 1α-hydroxlase enzyme that activates vitamin D, causing excessive calcium absorption, which in turn appropriately suppresses PTH secretion. When the origin of hypercalcaemia is unclear, measurement of 1,25-(OH)2 vitamin D can help to identify increased conversion of 25-OH vitamin D to 1,25-(OH)2 vitamin D. There is no other clinically useful application for measuring 1,25-(OH)2 vitamin D .
Treatment of hypercalcaemia
There are a number of considerations when making treatment decisions (Box 2).
Emergency management of hypercalcaemia
The first intervention in severe hypercalcaemia (>3.5 mmol) or in symptomatic individuals is always restoration of euvolaemia. Intravenous normal saline at rates of up to 500 ml/h can be required and the patient’s underlying co-morbidities should be considered when prescribing the rate of infusion.4 Less than 30% of patients achieve normocalcaemia with fluids alone.5 Bisphosphonates are considered after fluid replacement (see section on excess bone resorption below). It is important to make sure blood has been tested for PTH level before giving bisphosphonates as they can alter serum PTH levels and give misleading PTH results. Subcutaneous or intramuscular calcitonin can achieve a rapid lowering of serum calcium through increased renal excretion, but beware of rebound hypercalcaemia. Life-threatening hypercalcaemia is an indication that haemodialysis should be considered.5 Early or semi-urgent parathyroidectomy might be performed in severe primary hyperparathyroidism or even in the second trimester of pregnancy if indicated.12
Primary hyperparathyroidism
Parathyroidectomy is the only definitive treatment for primary hyperparathyroidism.10 All symptomatic patients should be considered for surgery. Asymptomatic patients should be considered for surgery if serum calcium is ≥0.25 mmol above the upper limit of the reference range, if glomerular filtration rate (GFR) is <60 ml/min, if the T score is <–2.5 at any DXA scan site, if the patient has a history of previous fragility fracture, or if the patient age is <50 years of age.10 Some patients are unsuitable for or fail surgery; cinacalcet is licensed for these patients in the UK. Cinacalcet reduces PTH levels by acting on the CaSR. It is effective in lowering hypercalcaemia to <2.57 mmol/l in 75% of patients with sustained effects over 5 years of treatment, but there is little evidence to date regarding end organ effects.8
Causes of hypercalcaemia.
Approach to management of hypercalcaemia.
Hypercalcaemia secondary to excess bone resorption
This group includes patients with malignancy-associated hypercalcaemia resulting from PTH-related protein secretion or osteolysis.4 Bisphosphonates are effective in hypercalcaemia secondary to bone resorption.5 A number of intravenous bisphosphonate preparations are licensed in the UK for hypercalcaemia of malignancy. Zolendronic acid might have a lower rate of relapse than other bisphosphonates.13 Denosumab is a biological anti-resorptive agent that is licensed for the prevention, but not treatment, of skeletal-related events including hypercalcaemia in solid tumours.5,14
1,25-(OH)2 vitamin D-induced hypercalcaemia
Hypercalcaemia that is caused by this mechanism results from increased absorption of calcium from the gut, thus bisphosphonates are not useful. Tumours or granulomas that produce 1α-hydroxylase might respond to steroid therapy.4
Summary
The management of patients with hypercalcaemia should be informed by the patient’s symptoms and signs, by the degree of elevation of calcium, by the underlying mechanism by which calcium has been elevated and by the disease process underlying the presentation. Regardless of diagnosis, all significantly hypercalcaemic patients should be rendered euvolaemic before any further and more specific treatment is considered. Highly symptomatic patients and those with a calcium level of >3.5 mmol represent a medical emergency that requires inpatient treatment.
- © 2013 Royal College of Physicians
References








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.