
- Hyponatraemia
- plasma osmolality
- syndrome of inappropriate antidiuresis (SIAD)
- urine sodium concentration
- vasopressin
Key points
Hyponatraemia is present in 15–20% of non-selected emergency hospital admissions
Hyponatraemia is associated with increased mortality and morbidity in patients presenting with a range of underlying clinical problems
Whether the relationship between hyponatraemia and mortality reflects a causative role or the association of two variables, both linked to disease severity, is unclear
Hyponatraemia is often multifactorial
Management requires a systematic approach based on clinical presentation
Sodium is the major circulating cation and the concentration of sodium in serum is maintained within a tight physiological range. Two metrics are important in the description of hyponatraemia, both of which influence clinical presentation:
biochemical severity based on concentration of sodium in serum:
– mild: 130–135 mmol/l
– moderate: 125–129 mmol/l
– profound: <125 mmol/l
speed of development
– acute
– chronic.
Epidemiology
Incidence and impact on mortality
Hyponatraemia is a clinical feature in 15–20% of non-selected emergency admissions to hospital in the UK. It is associated with increased mortality, morbidity and length of hospital stay in patients who present with a range of conditions.1 A recent single-centre study demonstrated an adverse impact with hyponatraemia of 120–134 mmol/l, but not below this level. The relationship between the concentration of sodium in serum and mortality therefore is not simple. Large-scale prospective studies are needed to clarify whether the relationship reflects causative effect or simply the association of two variables that are each linked with disease severity.2
Emerging themes
Data link chronic hyponatraemia with gait instability and osteoporosis. Bone is a major reservoir for sodium, and bone loss may be an inevitable consequence of the physiological response to persistent hyponatraemia. The combination of increased risk of falls and bone fragility may be important when considering the health impact of hyponatraemia.3,4
Symptoms and signs of hyponatraemia
Symptoms and signs of hyponatraemia cover a broad range: from coma and seizures to normal or near-normal function. In isolation, they are non-specific. Hyponatraemia leads to a biphasic adaptation within the central nervous system (CNS). An initial efflux of inorganic osmolytes from glial cells into the extracellular space is followed by generation and efflux of organic osmolytes if hyponatraemia persists. Both serve to minimise brain swelling and preserve neuronal function. Hyponatraemia that exceeds the capacity of this adaptive response – or that develops at a rate that exceeds the rate of adaptation – leads to greater neuronal dysfunction and more severe symptoms (Fig 1).

Factors contributing to clinical status in hyponatraemia. Na+ = sodium.
Mechanisms and causes
The concentration of sodium in serum reflects sodium and water content, with each component reflecting the balance between intake, output and volume of distribution. Sodium balance, water balance and circulating volume are regulated through coordinated neurohumoral processes and are key players in the development and maintenance of hyponatraemia.
There are two routes to hyponatraemia:
dilutional
– high water intake in excess of normal water loss
– reduced renal water loss (antidiuresis) with normal water intake
solute (sodium) loss in excess of water loss.
Solute loss leads to reduced effective arterial blood volume, hypovolaemia-stimulated release of vasopressin (AVP) from the posterior pituitary and reduced renal water excretion. Solute loss thus produces hyponatraemia through two linked mechanisms.
This view facilitates an approach to the differential diagnosis of hyponatraemia based on urine osmolality and urine sodium concentration (Table 1).
Classification of hyponatraemia.
Pseudohyponatraemia and non-hypotonic hyponatraemia
Analysis of electrolytes in the routine clinical laboratory involves a dilution step that assumes a normal distribution of the aqueous and non-aqueous phases of venous blood. High levels of triglycerides, cholesterol and total protein disturb this distribution and can produce artefactual hyponatraemia (pseudohyponatraemia), even if ion-selective electrodes are used. As measurement of serum osmolality does not involve a dilution step, serum osmolality is normal. Sodium measurement by blood gas analyser (which uses direct potentiometry) is not affected in this way.5
Glucose, mannitol and glycine (used in perioperative irrigation fluid) increase serum osmolality, resulting in a shift in fluid from the intracellular to the extracellular compartment, which leads to dilutional hyponatraemia. Initially, there is no risk of cerebral oedema; however, as the additional osmolyte is removed, the osmotic drive for fluid shift reduces and the concentration of sodium in serum increases. In patients with diabetic ketoacidosis and hyperglycaemic hyperosmolar syndrome, a decrease in glucose in serum that exceeds the increase in concentrations of sodium in serum can reverse the initial fluid shift, leading to cerebral oedema.6 Causes of pseudohyponatraemia and non-hyponatraeimia are shown in Table 2.
Causes of pseudo- and non-hypotonic hyponatraemia.
Excess hypotonic fluid intake
Absorption of hypotonic fluids at a rate that exceeds renal excretion of free water will inevitably result in hyponatraemia. This can be seen with oral fluid intake (primary polydipsia), intravenous fluid therapy, and absorption of hypotonic irrigating fluids following surgery to the lower renal tract or colonoscopy.
Intravascular volume depletion
Long-term diuretic use can produce significant hyponatraemia by promoting solute loss. As hyponatraemia may develop slowly, there may be few symptoms. Inhibitors of renin–angiotensin system (RAS) can also cause hyponatraemia by reducing effective circulating volume.
Portal hypertension, congestive cardiac failure and hypoalbuminaemia also result in reduced effective arterial volume and produce hyponatraemia through the action of volume-stimulated AVP. Drugs used in the treatment of these conditions may exacerbate hyponatraemia.
Syndrome of inappropriate antidiuresis
In syndrome of inappropriate antidiuresis (SIAD) there is a failure to suppress secretion of AVP as plasma osmolality falls below the normal osmotic threshold for its release.7 As patients continue to drink, persistent antidiuresis produces dilutional hyponatraemia. Box 1 outlines the diagnostic criteria for SIAD. Most patients with SIAD are clinically euvolaemic. The concentration of sodium in urine is often higher than 60–80 mmol/l. Although SIAD results in a negative sodium balance, absolute concentrations of sodium in urine vary with sodium intake. Many drugs cause SIAD, so drug histories are an important part of the clinical assessment (Table 3).
Drugs commonly associated with SIAD.
Diagnostic criteria for SIAD.
Exercise-associated hyponatraemia
Extreme endurance exercise produces significant non-osmoregulated release of AVP and reduced renal blood flow. If an athlete’s fluid intake exceeds water loss, dilutional hyponatraemia will ensue. The risk of developing hyponatraemia increases with the length of time taken to complete an event. Occasional runners should be advised to follow their thirst as they run and to avoid rigid, time-based fluid intake.8
Nephrogenic SIAD
The action of AVP on renal water excretion is mediated by the type 2 AVP receptor (V2-R). Gain-of-function mutations lead to constitutive activation of the V2-R and antidiuresis (with ensuing hyponatraemia) in the absence of AVP, described as nephrogenic syndrome of inappropriate antidiuresis (NSIAD). The clinical characteristics can be variable, with presentation in childhood or adult life.9
Central salt wasting
Central salt wasting (CSW) is a rare cause of hyponatraemia characterised by primary natriuresis and subsequent hypovolaemia. It has been described in a range of neurosurgical conditions and in brain injury. The underlying mechanism(s) may involve increased release of natriuretic peptides and/or reduced sympathetic drive. Syndrome of inappropriate antidiuresis can occur in the same group of patients and it is critical to make the correct diagnosis.10
Investigation and differential diagnosis
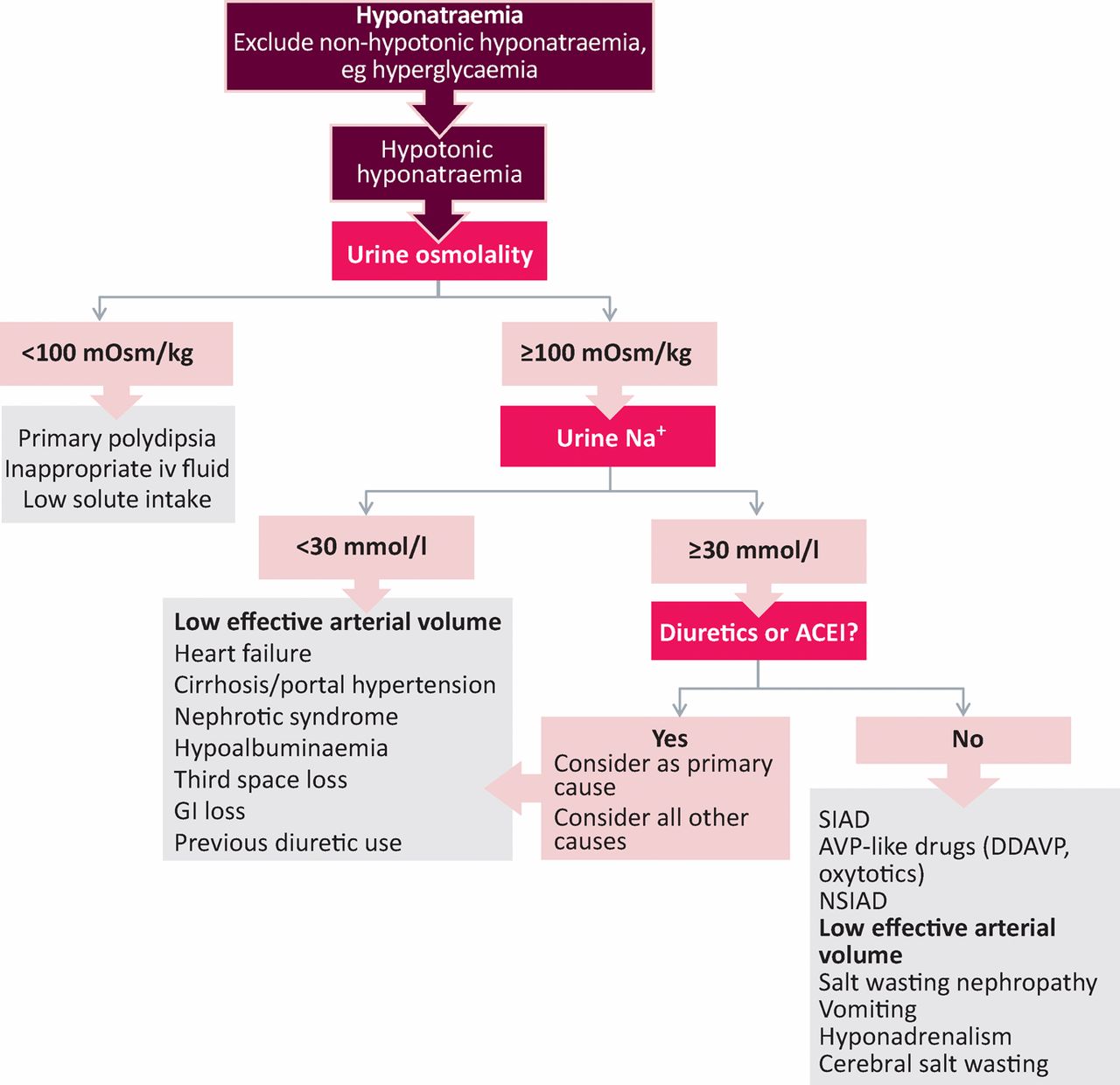
The differential diagnosis of hyponatraemia can be challenging. Several factors may be contributing to aetiology. Comorbidities are common. The clinical situation may be dynamic and supportive information may not be available when needed. Diagnostic approaches that prioritise urine osmolality and urine sodium concentration above clinical assessment of volume status (which is often inaccurate) can be useful.11 A cut-off concentration of sodium in urine above which hypovolaemia is excluded is key. The diagnostic utility of sodium concentration in urine is reduced in patients taking diuretics (Fig 2).

Diagnostic algorithm for patients presenting with hyponatraemia. ACEI = ACE inhibitor; AVP = vasopressin; DDAVP = desmopressin; GI = gastrointestinal; Na+ = sodium; NSIAD = nephrogenic syndrome of inappropriate antidiuresis; SIAD = syndrome of inappropriate antidiuresis.
Approaches to treatment
Although hyponatraemia can be life threatening, chronic hyponatraemia can be tolerated very well, even when profound. Rapid correction of hyponatraemia to which the brain has adapted risks significant neuronal osmolar stress and life-threatening osmotic demyelination within the CNS. A stratified approach is needed: balancing the severity of the clinical situation, the efficacy and potential adverse effects of intervention, and the impact of persisting hyponatraemia.
Hyponatraemia with significant coma or seizures
Hypertonic sodium chloride
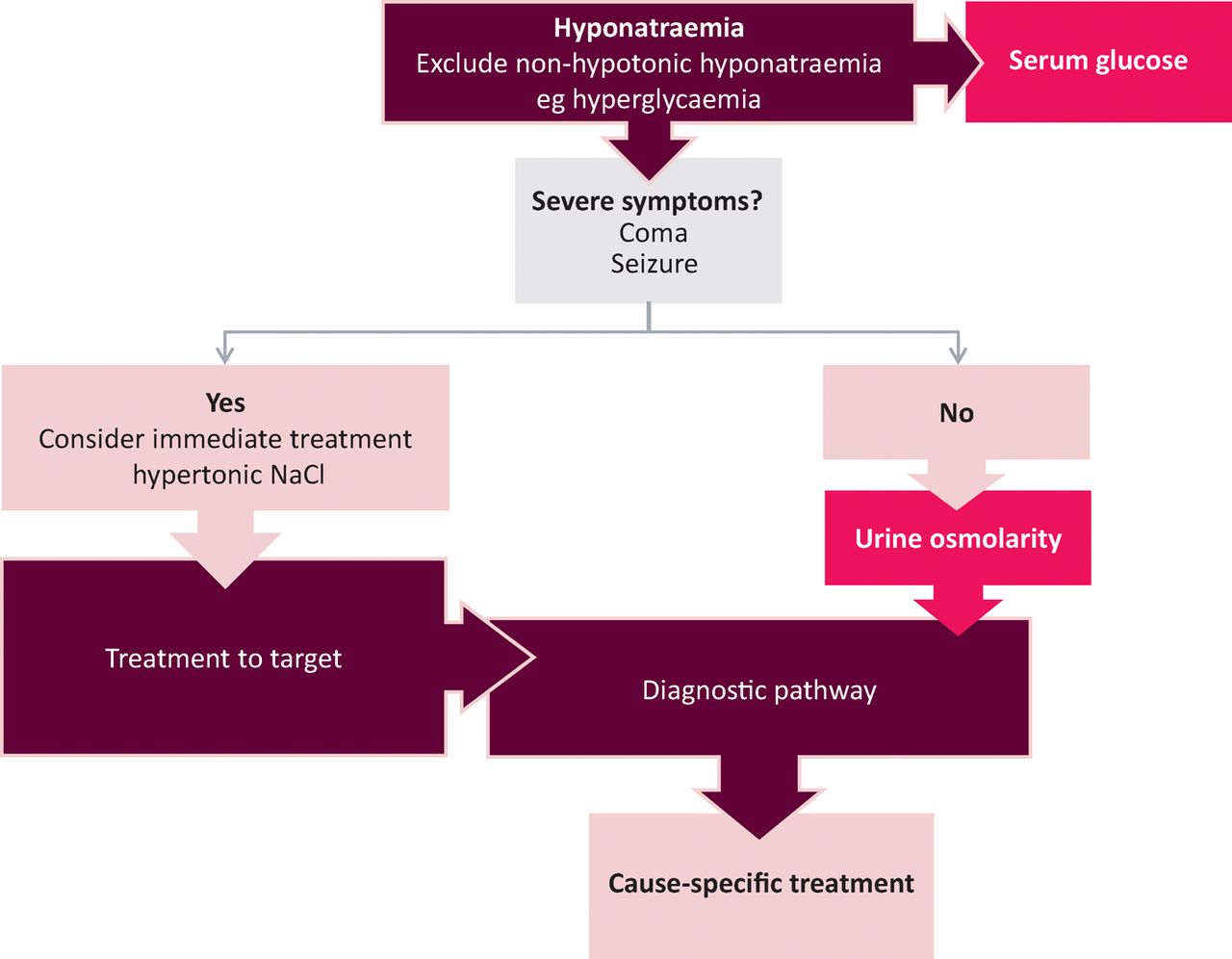
Severe symptomatic hyponatraemia is a medical emergency. It requires prompt treatment with 3% intravenous hypertonic sodium chloride solution (3% NaCl).12 Models to estimate total body water excess or total body sodium deficit can help guide target rates and volumes.13 The rate of increase in concentration of sodium in serum must be controlled carefully (Box 2). Although there is no clear consensus on the clinical or biochemical targets, there is general agreement that 3% NaCl should be stopped when clinical drivers (eg seizures) have been addressed. This is generally achieved when the concentration of sodium in serum is below the normal range. Diagnostic tests aimed at establishing aetiology should not delay treatment. Cause-specific management should be introduced as soon as it is practical (Fig 3).
Sodium chloride (3%) solution in treatment of hyponatraemia.
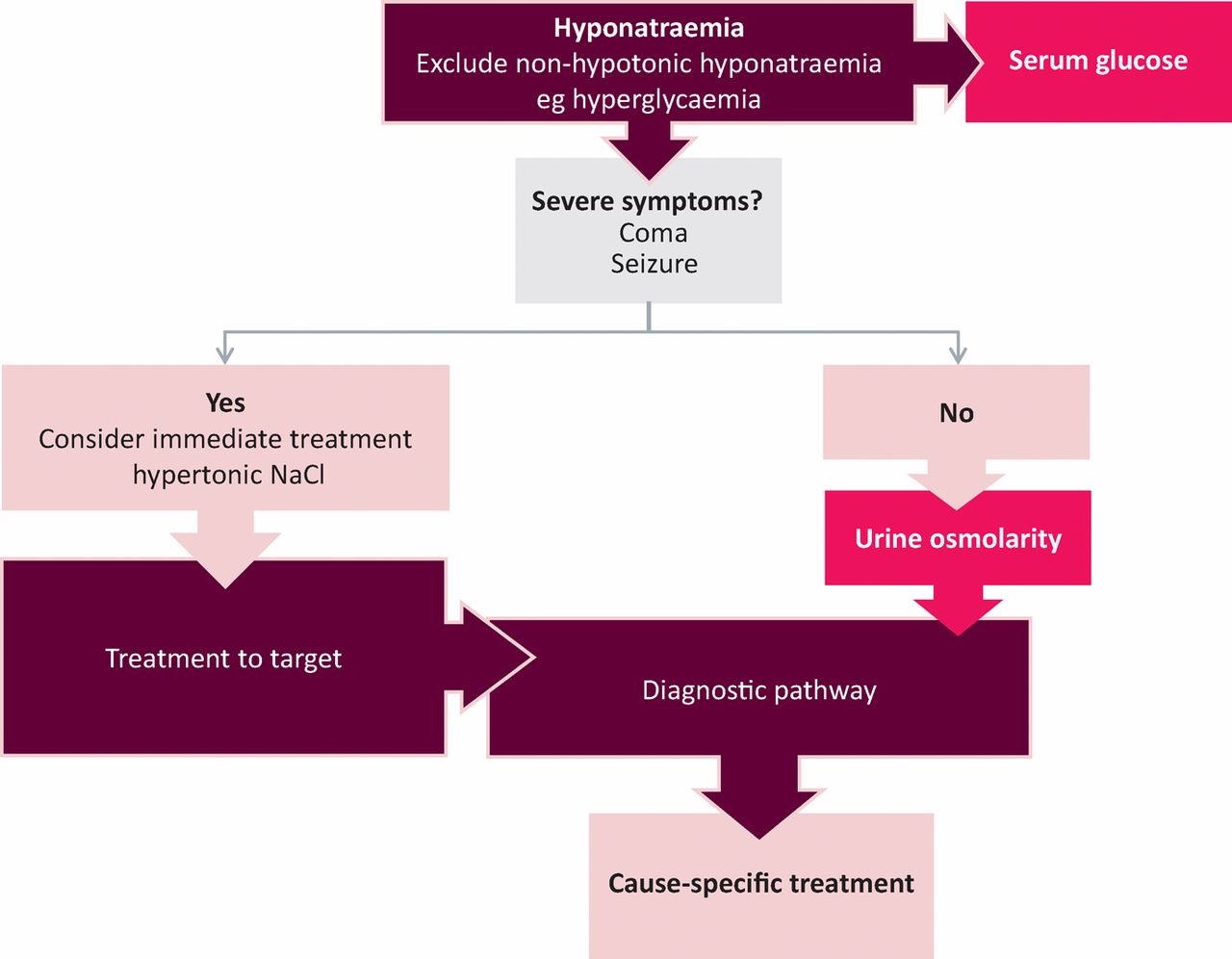
Management algorithm for the treatment of hyponatraemia. NaCl = sodium chloride.
Overcorrection of hyponatraemia when giving hypertonic fluids
Increases in the concentration of sodium in serum at rates in excess of target (overcorrection) should trigger active management to avoid osmotic demyelination14 (Box 3).
Management of overcorrection of concentration of sodium in serum during treatment with 3% sodium chloride solution.

Cause-specific treatment of hyponatraemia presenting with mild symptoms
Hypovolaemia should be corrected with 0.9% normal saline. When practical, culprit medications should be withdrawn (Table 4). The rate of change of the concentration of sodium in serum should not exceed 8–10 mmol/l in the first 24 hours and 18 mmol/l in the first 48 hours. Sodium may increase faster than 2 mmol/l/h during ‘autocorrection’ of hyponatraemia when an underlying cause has been removed. Osmotic demyelination can still occur in these circumstances. Overcorrection should be managed with fluids to slow the rate of increase or to reduce the concentration of sodium in serum.
Cause-specific treatments for hyponatraemia
If hyponatraemia fails to resolve, it is important that the differential diagnosis is reviewed and the basis for intervention reconsidered. Clinical decisions must balance the benefits and potential adverse effects of further intervention against tolerating mild, persisting hyponatraemia. In patients with SIAD, urea can be effective as an adjunct to water restriction. The response to demeclocycline is variable and the drug has a significant adverse effect profile. The AVP antagonists (vaptans) are a rational alternative, but their optimal place in management is still to be clarified.15 In the absence of symptoms, intervention aimed simply at improving mild biochemical hyponatraemia may not be required.
- © 2013 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.