
Introduction
One percent of laboratory samples are rejected as ‘unsuitable for analysis’. The report may state ‘no sample received’, ‘unlabelled specimen’, ‘under-filled sample’, ‘leaking’ and ‘incorrect container’, necessitating a repeat sample. However, a proportion of ‘unsuitable’ laboratory samples are due to contamination or artefact. We present two cases in which the laboratory comment ‘unsuitable’ has diagnostic implications due to the underlying disease directly affecting serum. In each case, recognition of the pathology facilitated early directed treatment.
Case 1
A 21-year-old man was admitted with acute severe abdominal pain. He was obese (body mass index 33 kg/m2) and had poorly controlled type 2 diabetes mellitus (HbA1c 11.8%). Examination revealed hypovolaemia with central abdominal tenderness, capillary glucose of 22.0 mmol/l, and urine dipstick glucose 3+, ketones 4+ and protein 1+. Initial blood tests in the emergency department revealed a haemoglobin (Hb) of 16.3 g/dl, white cell count (WCC) of 15.4 × 109/l, platelet count (Plt) of 207 × 109/l and compensated metabolic acidosis on arterial blood gas analysis. Biochemistry tests – including urea, electrolytes and liver chemistry – were not processed and an automated laboratory comment of ‘unsuitable (haemolysed, icteric or lipaemic)’ was attached to the report. The tests were repeated and the results sodium (Na) 136 and potassium (K) 4.5mmol/l were returned with the comment ‘measured on Ilyte’. Serum amylase was 646 iu/l but urea (Ur), creatinine (Cr) and liver chemistry were again judged as ‘unsuitable’. This time a manual report also stated ‘specimen is haemolysed and grossly lipaemic’. A diagnosis of acute pancreatitis with diabetic ketoacidosis was made and intravenous analgesia, fluids, insulin and potassium replacement were administered. The triglyceride level was subsequently found to be significantly elevated at 78.2 mmol/l. Following treatment, the patient’s clinical state improved, with resolution of the abdominal pain, acidosis, hyperglycaemic state, and lowering of the triglyceride level.
Case 2
A 71-year-old man was admitted with abdominal pain. He had a history of significant alcohol intake and type 2 diabetes mellitus. On examination he was mildly confused, cachectic and demonstrated signs of mucosal bleeding. There was no hepatosplenomegaly. Initial blood tests in the emergency department revealed profound macrocytic anaemia, with a Hb of 5 g/dl, mean corpuscular volume (MCV) of 106.4 fl, Plt of 189 × 109/l, WCC of 12.8 × 109/l, 74% neutrophils, 21% lymphocytes 21% and international normalised ratio (INR) of 1.0. He was transfused with red blood cells while further investigations were arranged to evaluate the cause of his anaemia. A blood film demonstrated severe macrocytic anaemia with no specific features.
A comment of ‘unsuitable … sample fully clotted’ was returned for the initial and subsequent biochemistry samples sent to the laboratory. A hyperviscosity syndrome was presumed and the case discussed with the clinical biochemist and haematologist to elucidate the cause of excess clotting. Biochemistry samples were sent to an external laboratory for testing using a different analyser and demonstrated the following: Na 143, K 6.6, Ur 15.0 mmol/l, Cr 147, bilirubin 3 umol/l, alkaline phosphatase (ALP) 62u/l, total protein 120, globulin 82, IgM paraprotein 135 g/l, albumin 38 g/l, calcium (Ca) 2.67, phosphate (PO4) 3.1 mmol/l, serum B12 1100 ng/l, and serum folate 4.1 ug/l. There were no cryoglobulins in the blood. During the course of his admission he became progressively drowsy. Bone marrow aspiration and biopsy showed bone marrow lymphoid infiltration, the underlying diagnosis being non-Hodgkin’s lymphoma with elevated IgM paraprotein levels. He subsequently underwent three cycles of plasma exchange with consequent improvement in confusion and conscious level.
Discussion
In both of these cases the initial ‘unsuitable for analysis’ laboratory report was diagnostically useful as it was the direct effect of the underlying pathology on the serum which rendered it unsuitable. In the first case, early identification of the lipaemic serum as the cause of this unsuitability provided a clue that severely elevated triglyceride levels (78.2 mmol/l) were the principal cause for the patient’s pancreatitis. Although fluid resuscitation remains the mainstay of pancreatitis management, there are differences in treatment of the varied causes such as use of endoscopic retrograde cholangiopancreatography (ERCP) for gallstones. As well as hypertriglyceridaemic pancreatitis, an important feature of management is that large quantities of intravenous insulin are often required to reduce the triglyceride levels and acidosis. Lipaemic samples should alert the clinician to a variety of disorders including diabetes, alcoholism, pancreatitis and hypothyroidism.
In the second case, the hyperviscous ‘unsuitable’ biochemistry sample meant that repeated testing would not have provided further diagnostic information. It was crucial to establish the specimen’s hyperviscosity in order to identify the patient’s haematological malignancy and allow directed therapy with plasma exchange and chemotherapy.
In both cases, liaising with the biochemist and haematologist was useful. They are an often under-used resource of expertise in sampling problems. Clinicians should be alert to the causes of diagnostically useful ‘unsuitable’ or spurious results, which they may encounter due to analyser artefact (Table 1). In such situations, results should be interpreted with caution, but not dismissed without regard for a possible underlying cause.
Serum abnormalities in which clinicians may encounter ‘unsuitable for analysis’ laboratory reports.
This topic of evaluating ‘unsuitable for analysis’ samples has clear clinical governance ramifications and solutions to otherwise missed diagnostic opportunities may be:
to increase awareness of analyser artefact amongst primary care physicians and hospital doctors
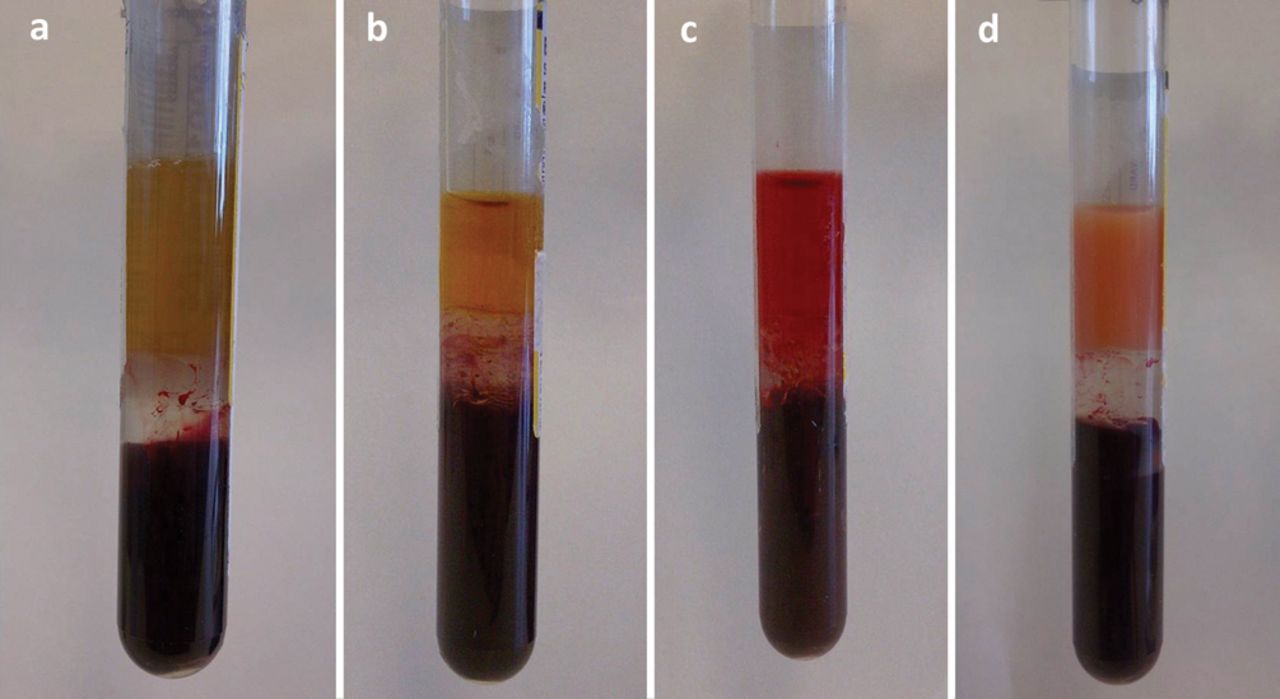
to provide more specific laboratory comments where appropriate eg there is a visual difference between lipaemic and normal centrifuged serum (Fig 1)
to provide general troubleshooting comments or extended laboratory advice where no visual difference exists.
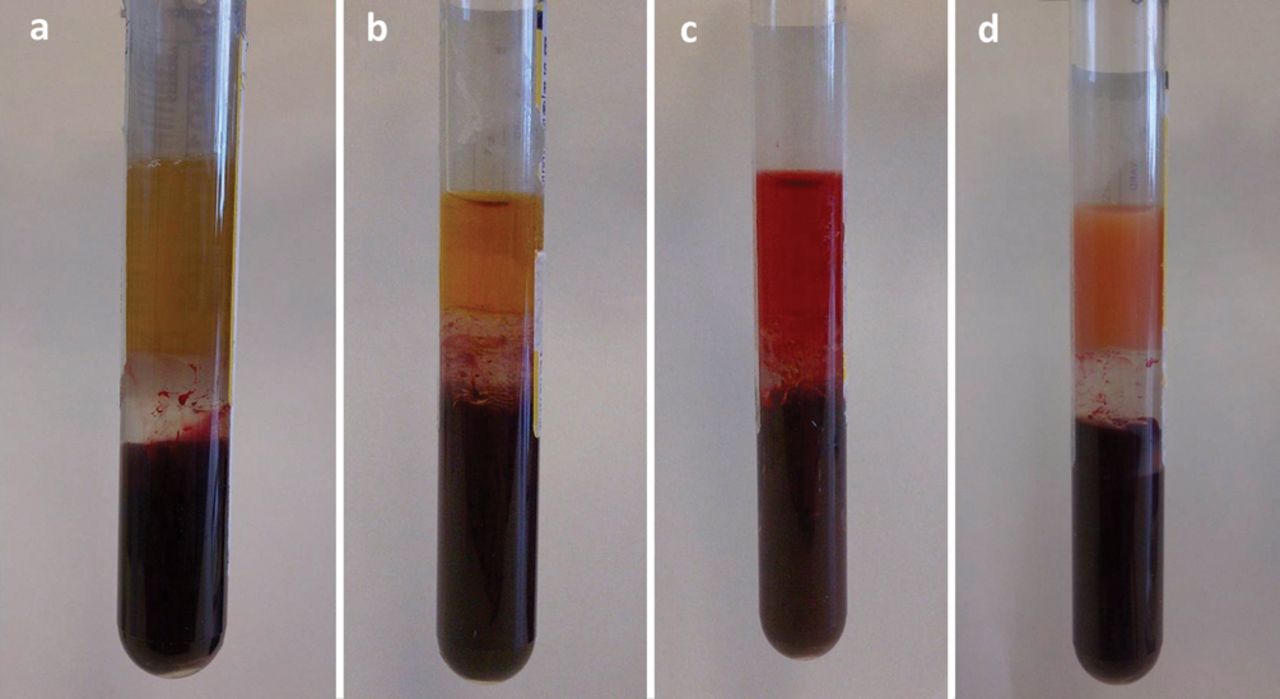
Clinical photographs of centrifuged whole blood showing three layers; in ascending order: red cell layer, white cell buffy layer and serum which is (a) normal, (b) icteric, (c) haemolysed and (d) lipaemic.
Early recognition of artefactually incorrect results and identification of the reason for ‘unsuitable for analysis’ samples can reduce unnecessary investigations, potentially avoid dangerous treatments6 and lead to early correct diagnosis of the underlying condition with institution of appropriate targeted therapy.
- © 2013 Royal College of Physicians








{kind=link}
Related Articles
Cited By...
- No citing articles found.