
Case presentation
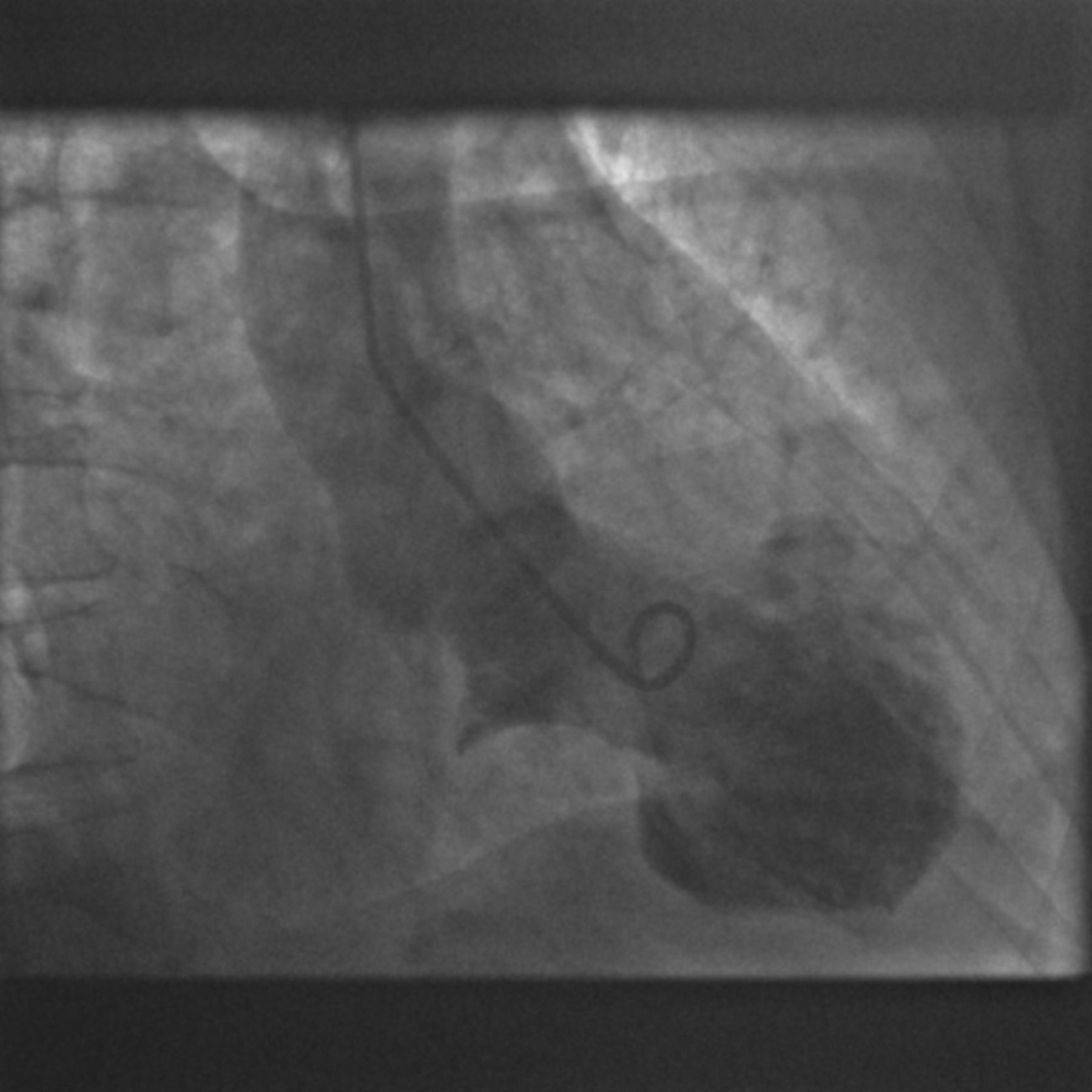
A 69-year-old female presented to the emergency department with acute left sided chest pain and dyspnoea, which started after an argument. She had no significant medical history or regular medication. Electrocardiogram (ECG) showed right bundle branch block and ST elevation in the anterolateral leads. A diagnosis of ST elevation myocardial infarction was made. She received appropriate treatment and was transferred for primary angioplasty. Subsequent left ventriculogram showed apical ballooning and hyper-contractile basal segments (Fig 2).

Coronary angiography showed no significant culprit lesion.

Left ventriculogram.
Based on these findings, a diagnosis of takotsubu cardiomyopathy (TC) was made. Biochemical investigations showed an elevated troponin, while cardiac magnetic resonance imaging (MRI) demonstrated akinetic apical segments and hyper-contractile basal segments. Overall left ventricle (LV) systolic function was severely impaired. However, late gadolinium imaging showed no late enhancement; proving viable cardiomyocytes.
The patient was commenced on standard heart failure therapy and discharged home after an uncomplicated 5-day admission. At follow up she remained well and a repeat cardiac MRI scan after 2 months showed complete LV recovery.
Lesson
Takotsubu cardiomyopathy was first described in 19911 and termed takotsubo by the Japanese in reference to the fishing pots used to catch octopi, which resemble the left ventricular apical ballooning due to akinetic myocardium and the hypercontractile cardiac base seen on ventriculogram during systole.2,3 TC has several pseudonyms including ‘stress cardiomyopathy’, and ‘broken heart syndrome’.3
The presentation of TC mimics acute coronary syndrome (ACS),2 but without significant coronary artery stenosis seen on angiogram.2 The majority of patients are post-menopausal women, and men account for as little as 10% of cases.2 The true prevalence is unknown, but is estimated at 1–2%, and may account for up to 2% of all ACS presentations.2 Individuals may describe recent intense emotional or physical stress prior to the onset of symptoms and the majority of patients report a physical stressor as the precipitating event. However, up to one-third of TC patients are unable to identify any preceding stressful event.2
Clinical presentation
Diagnostic criteria for TC4 are shown in Box 1. All criteria must be met to diagnose TC. The most common presenting symptom is cardiac chest pain (70–90%) followed by dyspnoea (20%). Severe cases may be complicated by pulmonary oedema, arrhythmias and cardiogenic shock.5
Modified Mayo Clinic diagnostic criteria. (Reproduced with permission of Prasad et al, 2008).4

Electrocardiogram abnormalities are transient, with anterior lead ST elevation most frequently encountered.5 ST elevation prompts rapid angiography and thus coronary patency is visualised leading to ACS exclusion.5 Deep T wave inversion is commonly seen a few days following initial presentation.3
Patients diagnosed with TC present with mildly raised troponin I levels,2,3 which peak at around 24 h post chest pain onset.4,5 Levels are not as elevated as those found in ACS and normalise quickly, unlike myocardial infarction.4–6
Left ventricular wall ballooning predominantly affects the apex (82%) and mid-ventricular myocardium, with relative sparing of the base.2 There are exceptions and patients may have apical sparing, or indeed biventricular akinetic dysfunction, the latter having a poorer prognosis.2,3 Cardiac function and left ventricular wall motion typically return to normal within days to weeks.4
Pathophysiology
Takotsubu cardiomyopathy is idiopathic,2,5 but the most favoured hypothesis is over-activation of the sympathetic nervous system and subsequently increased catecholamine release, especially adrenaline.4 Plasma catecholamine concentration is elevated in TC when compared to ACS. But not all TC patients describe a preceding stressful event, thus levels of catecholamines may not have been elevated.2
Several theories exist regarding TC aetiology, including:
Raised catecholamines cause epicardial coronary vasospasm.4
Catecholamines affect endothelial cell function reducing myocardial blood supply.3
Transient ischaemia secondary to a transient thrombosis in an extended left anterior descending coronary artery (LAD) occurs. The extended LAD hypothesis states that because the ventricular wall motion abnormalities seen in TC do not correspond to a single coronary artery territory, an extended LAD is present, which correlates to the area of akinetic left ventricle.7
However, these hypothetical aetiologies are either rarely seen,3 discredited via angiography5 or not well supported in current literature.2 No genetic link has been found.5
Complications and treatment
The mainstay of management involves supportive treatment. Haemodynamically stable patients are treated with angiotensin converting enzyme inhibitors (ACEi), beta-blockers and diuretics.4 Haemodynamically unstable patients may require intra-aortic balloon pumps.3
Left ventricular outflow tract obstruction may arise due to the abnormal hyperkinetic myocardial base and pressure changes between the left ventricle and the adjacent left atrium. These pressure changes cause medial deviation of the mitral valve towards the ventricular septum.7 Outflow tract obstruction ensues, manifesting as profound hypotension.4 Beta-blockers may reduce the contractility of myocytes within the cardiac base, alleviating some of the outflow obstruction.4,7
Judicious use of intravenous fluid is recommended as this may increase blood pressure and thus stroke volume. Likewise, it may exacerbate congestive cardiac failure (CCF).4 CCF is the most common complication and is more common in those presenting with right ventricular akinesis/hypokinesis (20%) and may manifest as pulmonary oedema (22%),5 warranting diuretics.4
Left ventricle thrombi may form in the akinetic ventricle.8 Prophylactic anticoagulation in those with apical hypo-/akinesis is indicated.3 Cardiac rupture is rare and most commonly affects the left ventricular wall. Beta-blockers may reduce intraventricular pressure and load, thus reducing possible rupture.9 Several arrhythmias have been described but these are uncommon.4
Prognosis
Prognosis of TC is favourable, with a low rate of recurrence (1–11%).3 One study showed that 4-year survival was no different to an age- and sex-matched population.3 However, as this is a relatively new condition, sufficient long-term data is not available. Ejection fraction and cardiac function, by definition, return to pre-morbid levels,2,4 as long as no other simultaneous cardiac insult has occurred. Cardiology follow up is advised to ensure complete recovery.4 Mortality is rare (1–2%)4,5 and mostly due to ventricular fibrillation2 or cardiac rupture.9
Conclusion
Heightened awareness of TC will improve diagnostic sensitivity and should also lead to more appropriate treatment. TC is not always preceded by a notable stressful event. Biventricular involvement should alert the clinician to potentially greater morbidity.
- © 2013 Royal College of Physicians








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.