
A 45-year old lady with Lynch Syndrome (also known as hereditary non-polyposis colorectal cancer) attended the endoscopy department for an upper and lower gastrointestinal endoscopy as part of her cancer surveillance programme. She had no previous history of intra- or extra-intestinal malignancies and her past medical history was otherwise unrevealing. The endoscopic investigations were uneventful and reported as normal.
The following day she re-attended the endoscopy department with a sudden history of dysphagia and odynophagia that had developed acutely in the early hours of the morning. On examination she was in distress but not dyspnoeic. Baseline observations were normal. A thorough examination of her neck revealed a 2 cm circular mass lateral to her trachea and above the left sternal insertion of the sternocleidomastoid muscle. The mass was neither pulsatile nor reducible but moved vertically with swallowing. No crepitus could be palpated in her neck. Pre-assessment blood investigations were normal including a clotting screen and a full blood count. A computed tomography (CT) scan of her neck and chest was promptly carried out.
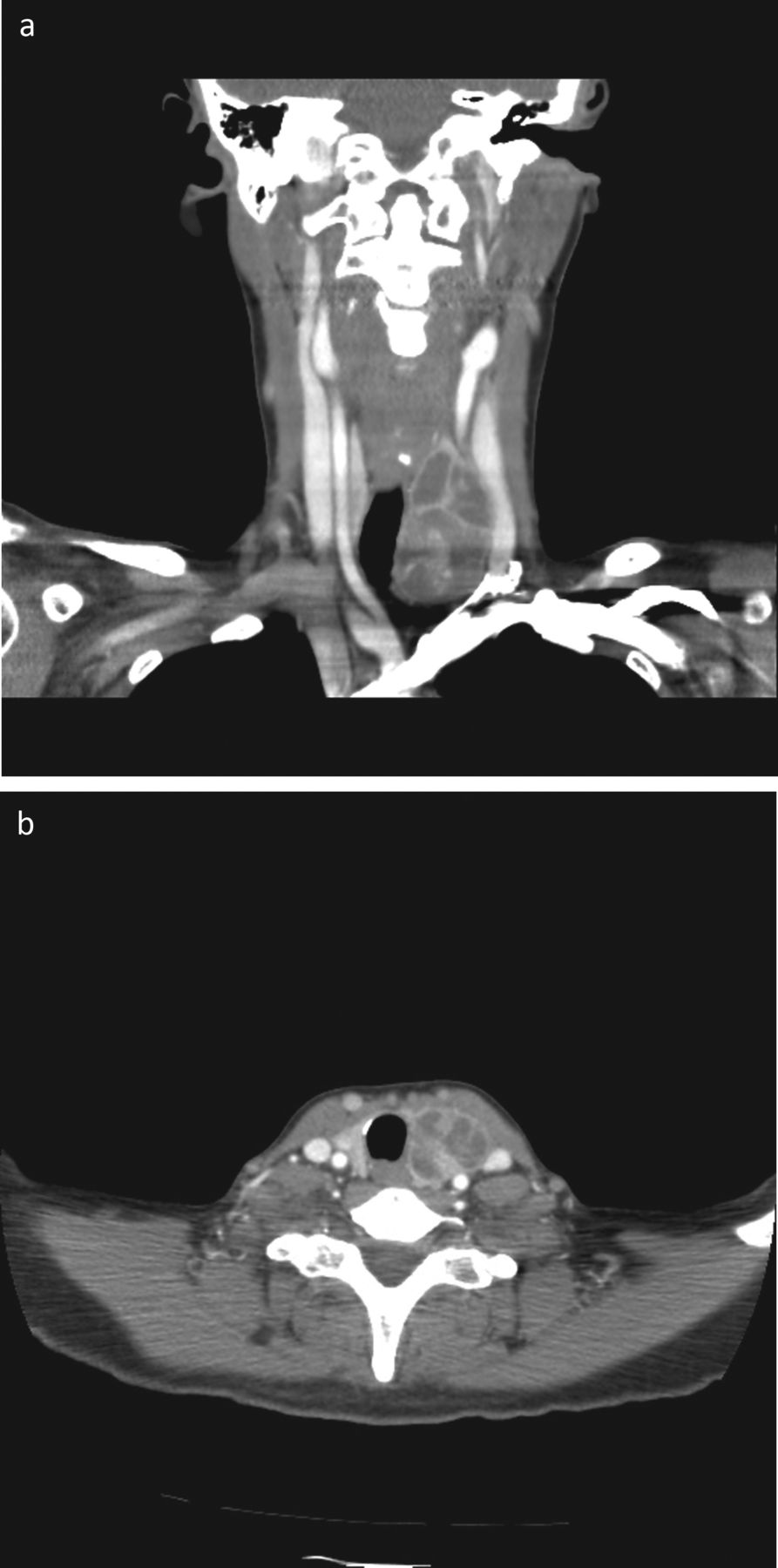
The images show a complex multicystic mass arising from the left lobe of the thyroid gland that is obstructing the proximal oesophagus and laterally displacing the suprasternal trachea. The inferior cyst shows a white homogenous discolouration signifying localised haemorrhage, probably caused by the endoscopic intubation. The patient was reviewed urgently by an otolaryngologist. Brown fluid, consistent with recent haemorrhage was aspirated by ultrasound-guided aspiration. Following this, the patient’s symptoms improved dramatically. She was managed conservatively with intravenous steroids and discharged uneventfully after 2 days.
Benign multicystic thyroid disease has not been described as an extraintestinal manifestation of Lynch syndrome, but thyroid malignancies have been occassionally reported.1 Haemorrhage is a potential complication of thyroid cysts and this can lead to life-threatening respiratory distress or dysphagia.2 Management strategies range from conservative measures including cyst aspiration, as illustrated in this case, to emergency partial thyroidectomy3 to secure haemostasis. Haemorrhage can be spontaneous,2 following blunt trauma4 or after penetrating injuries.5 This complication has been described after endotracheal intubation,3 but this is the first report where haemorrhage in a thyroid cyst has been described after an uneventful upper gastrointestinal endoscopy.
This is a potential complication in patients with thyroid cystic disease undergoing pharyngeal intubation. The patients would be more at risk if receiving anticoagulant or antiplatelet therapy. Physicians should be vigilant of such a potential complication.
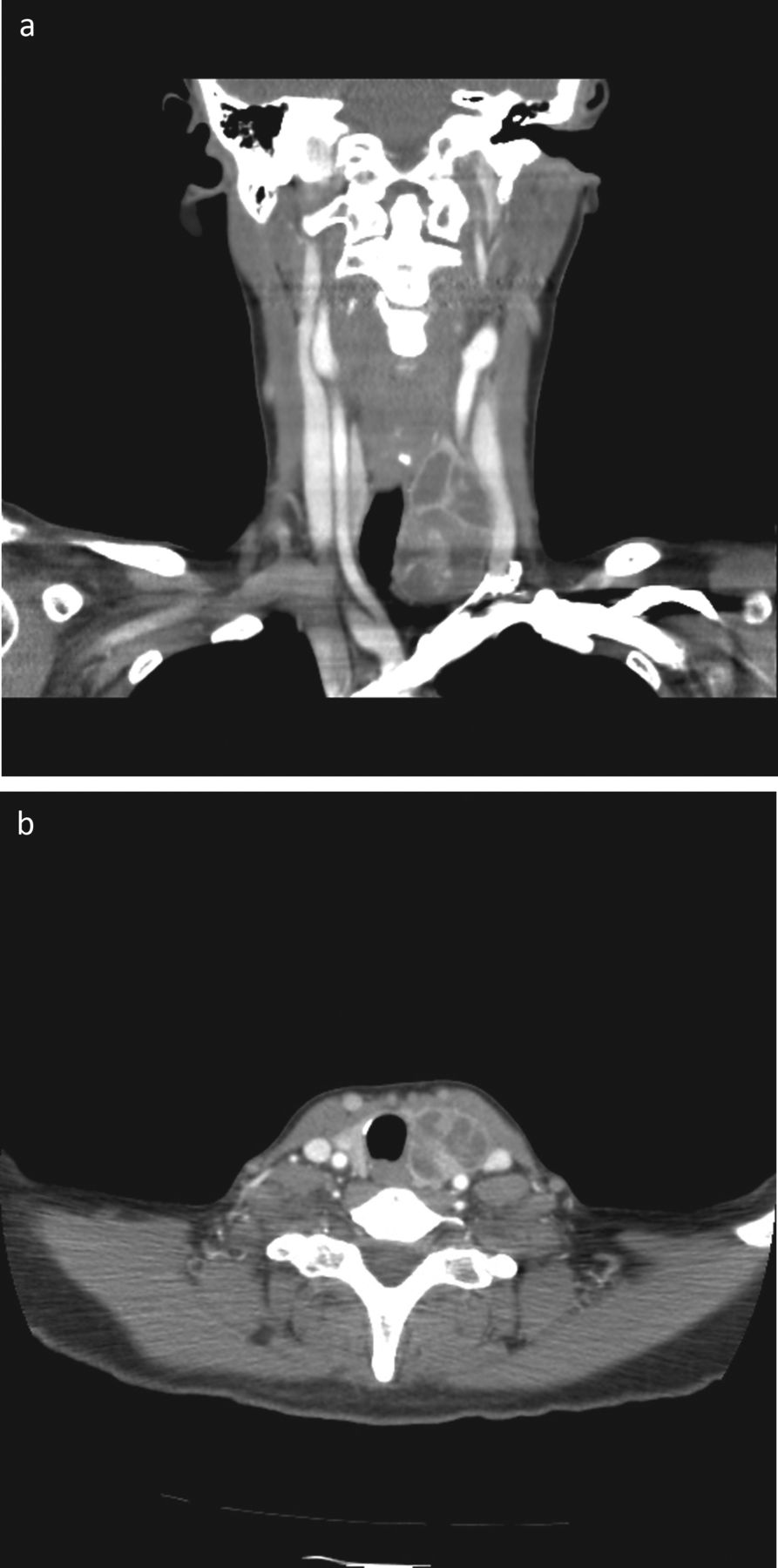
Sagittal (a) and coronal (b) computed tomography (CT) scan images of the patient’s neck and upper thoracic region showing a complex multicystic thyroid gland. The inferior cyst shows a white homogenous discolouration signifying recent haemorrhage.
Acknowledgements
K Pontoppidan drafted the manuscript. RP Mathew and GW Moran identified the case and critically appraised the manuscript. There are no conflicts of interest to declare.
- Royal College of Physicians








{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.