
Abstract
Granulomatosis with polyangiitis (GPA, formerly Wegener's granulomatosis) can present diagnostic difficulties for the clinician as there can be considerable overlap in features with tuberculosis (TB). Indeed, there are documented cases both of coexisting TB and GPA, and cases wrongly diagnosed as GPA when in fact TB was the underlying diagnosis. This lesson presents a case of GPA where TB was also considered as a differential and highlights the diagnostic and management difficulties when this is the case.
A 20-year-old male university student was referred by his GP with a 2-week history of dyspnoea, fever and productive cough. He later developed haemoptysis associated with night sweats, rigors and generalised arthralgia. He also reported sinusitis-type symptoms, but no recent epistaxis. The patient was treated by his GP with a course of amoxicillin and clarithromycin, but there was no improvement in symptoms.
He had no significant past medical history or family history. He had never smoked, but had travelled to Peru the previous year where he had had a tattoo.
On examination the patient had a low-grade fever, but other observations were normal. There were right-sided crackles on respiratory examination. The only other positive findings were mildly tender metacarpophalangeal (MCP) joints. Investigations showed raised inflammatory markers, but his blood tests were otherwise unremarkable. Urinalysis initially demonstrated haematuria and proteinuria, though this settled subsequently. A chest radiograph demonstrated numerous bilateral ill-defined nodular opacities (Fig 1). Sputum samples were sent for acid-fast bacillus (AFB) smear test and culture.

Chest X-ray showing numerous bilateral ill-defined nodular opacities.
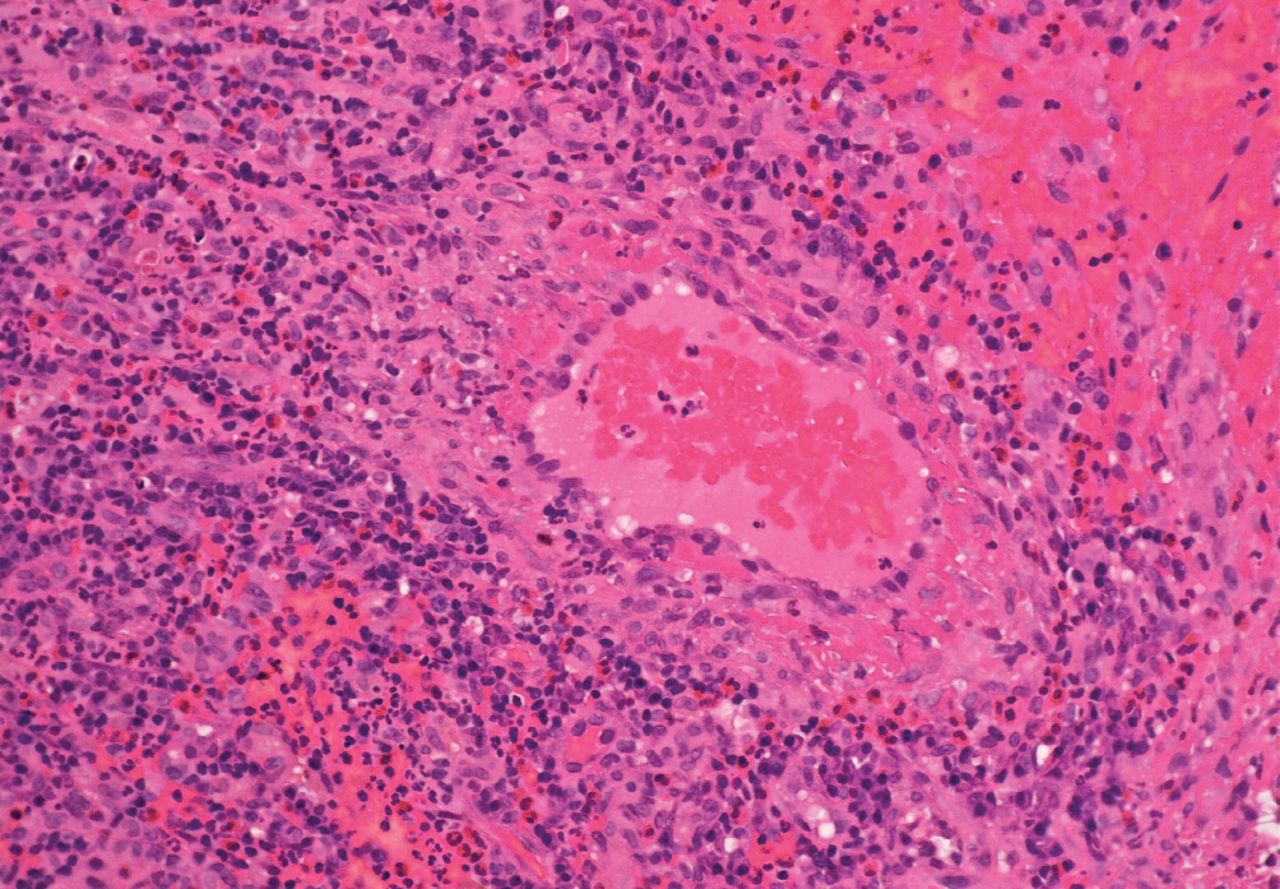
Due to his nasal symptoms, a nasendoscopy was performed, which demonstrated typical lesions for granulomatosis with polyangiitis (GPA). Biopsies were taken showing fibrinous areas with multi-nucleate giant cells, which were felt to be consistent with GPA (Fig 2). The autoimmune profile showed antinuclear antibody (ANA) and cytoplasmic antineutrophil cytoplasmic antibody (c-ANCA) positivity with anti-proteinase 3 positivity.

Histology slide showing multi-nucleate giant cells taken from patient's nasal biopsy.
A preliminary diagnosis of GPA was made based on the history and examination. High dose intravenous methylprednisolone was commenced. The smear results from his sputum were received demonstrating acid-fast bacilli.
He was isolated and commenced on quadruple therapy for TB. The smears were repeated and samples were sent to a tertiary centre for a repeat smear test and a polymerase chain reaction (PCR) test for TB. At this point he was being jointly managed between the respiratory, rheumatology and microbiology -departments.
A high resolution computed tomography (HRCT) scan was arranged, which showed numerous ill-defined opacities and possible early cavitation (Fig 3). The findings were more in keeping with GPA and were considered atypical of a diagnosis of TB.
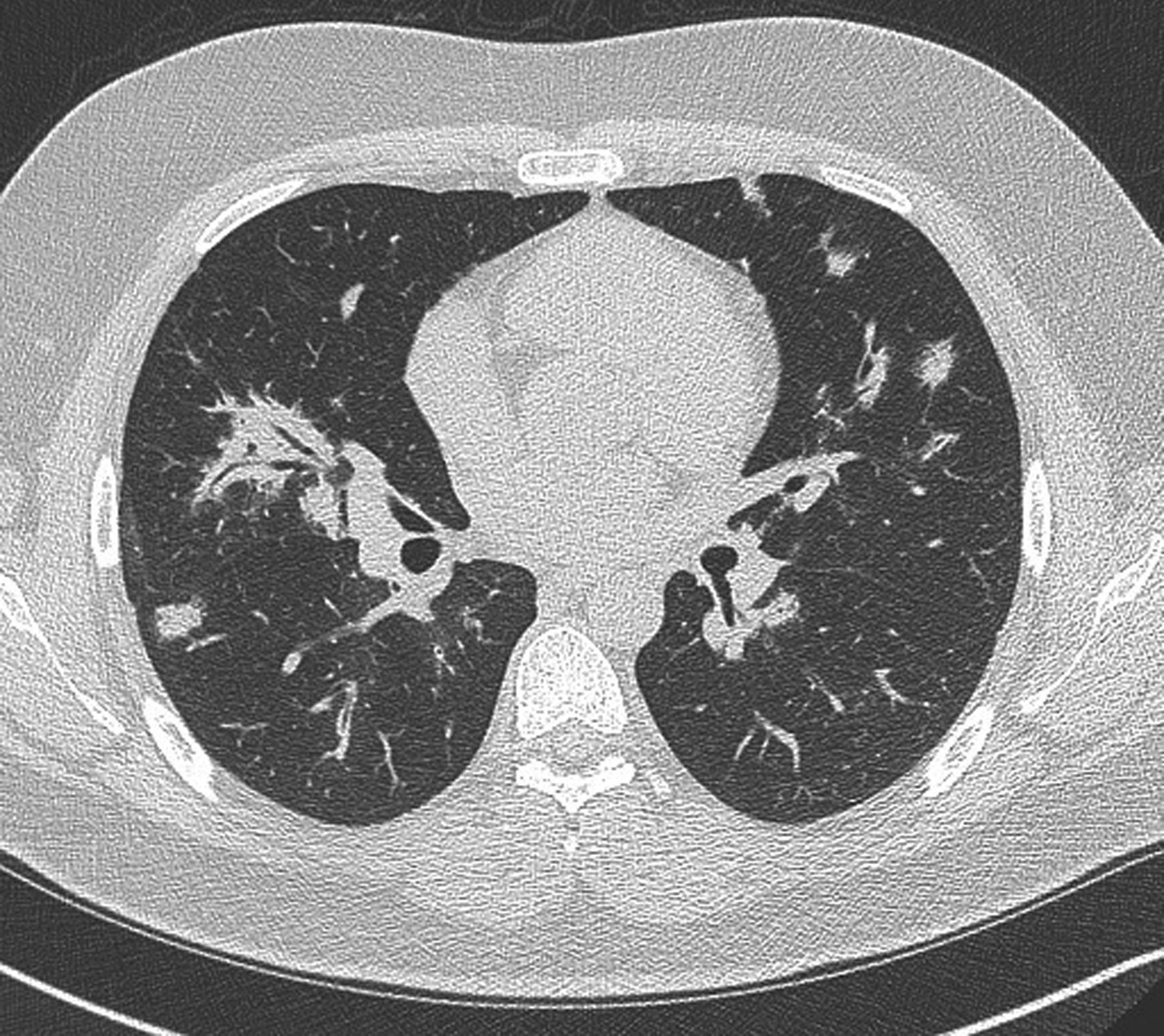
HRCT slice in which ill-defined opacities and possible early cavitation can be seen. HRCT = high resolution computed tomography.
Feeling that GPA was the more likely diagnosis, the patient was commenced on rituximab to induce remission. Unfortunately, the following day the patient became unwell, febrile and hypotensive, with an increase in his inflammatory markers and renewed haematuria. A repeat chest radiograph showed some progression in the opacities when compared with the previous film. At this time PCR testing was negative for TB; however his antibiotics were continued until culture proved negative at 6 weeks.
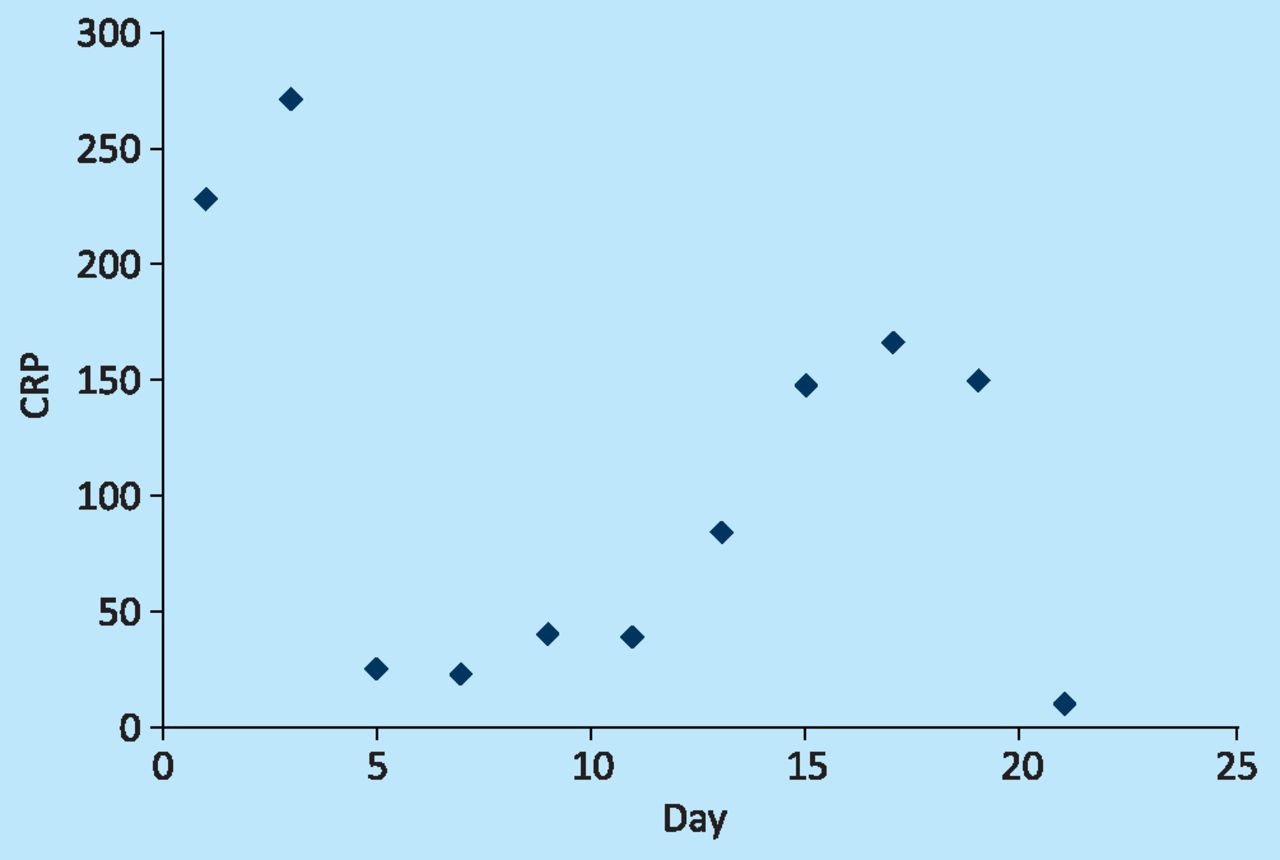
Due to deterioration in symptoms and possible renal involvement, he was taken to the intensive care unit (ITU) where he received five plasma exchanges over 5 consecutive days. The patient responded well to this, with a dramatic drop in his inflammatory markers (Fig 4) and with much symptomatic improvement. He was later discharged home under follow up as an outpatient.

CRP of the patient during the course of admission. Five plasma exchanges were given over 5 consecutive days the patient stayed in ITU. The patient was transferred to ITU on day 17, and plasma exchange was started. CRP = C-reactive protein. ITU = intensive care unit.
Discussion
Granulomatosis with polyangiitis (GPA) was first described in 1936 by Dr Friedreric Wegener as a necrotising granulomatous disease involving the upper and lower respiratory tract.1 It wasn't until 1954 that the ‘Wegener's triad’ of necrotising glomerulonephritis, necrotising granulomatous inflammation of the respiratory tract and necrotising systemic angiitis were described by Churg and Goodman.1 The disease is rare with a peak incidence in the fourth or fifth decade. Males and females are equally affected and 80–97% of those with the disease are Caucasian. It presents as a systemic vasculitis predominantly affecting the small arteries, with lesions involving the upper respiratory tract, lungs and kidneys. Patients report haemoptysis, rhinnorrhoea and epistaxis, and can develop a vasculitic rash. Non-specific symptoms such as rash, arthralgia and malaise can also occur. Renal involvement tends to occur later in the disease lifespan and, due to progressive deterioration, often results in a need for dialysis. Classically, cytoplasmic antineutrophil cytoplasmic antibodies (c-ANCA) and anti-proteinase-3 positivity aid diagnosis, which is confirmed by biopsy findings of vascular/perivascular granulomatous inflammation.
Trying to differentiate GPA from TB can be challenging due to the overlap in presentations between the two. This can lead to misdiagnosis and subsequently inappropriate management. Lesions can be radiologically similar on lung imaging2 and autoantibodies classically used to diagnose GPA can also be positive in TB.3,4 Therefore, caution should be applied in interpreting results, especially where TB is a possibility.
If an inappropriate diagnosis of GPA is made, the immunosuppression will result in worsening of underlying TB. There are reports of this occurring with resultant miliary TB.5 Conversely, a delayed diagnosis of GPA has significant risks to long-term dialysis-free survival.
Further complicating matters are reports, albeit rare, of GPA co-existing with TB.6 In some cases it may be necessary to treat the patient for both conditions. It was felt to be highly unlikely that this patient had both conditions. However, his history and the AFB-positivity of the smear test left little choice but to also cover him with antituberculous treatment. In this case the AFB result turned out to be spurious and contamination of samples from tap water in the laboratory with non-tuberculous mycobacteria proved to be a recognised complication.7
GPA can be a straightforward diagnosis to make if a patient presents in a ‘textbook’ fashion but our case illustrates that there are many features that can overlap with TB, creating uncertainty around diagnosis and management. Furthermore, test results can also overlap between the two, or samples, albeit rarely, can become contaminated with bacteria, complicating the diagnosis. A high index of suspicion is necessary to ensure that the correct diagnosis is made and that TB is always considered as a possible differential or as a coexisting pathology.
- © 2013 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.