
ABSTRACT
The burden of cancer is increasing, with a significant increase in cancer-related emergencies and patients with known malignancy presenting to the acute medical unit (AMU). We performed a retrospective analysis at a university hospital in the north west of England in May 2011. We examined 300 consecutive admissions to determine the number of, and reason for, cancer patients presenting to the AMU. Patients with cancer had a statistically significantly longer average length of inpatient stay than patients without cancer (8.8 days vs 7.2 days, p<0.01). As the incidence and prevalence of cancer increases, the challenge of improving the experience, safety and outcomes of patients with cancer becomes more important. Development of successful acute oncology services with close working with acute physicians will be essential in order to achieve this.
Introduction
The burden of cancer is increasing, and with an ageing population and improved outcomes following oncology treatment the incidence of cancer is estimated to increase by 33% by 2020, with a significantly increased prevalence.1–3 As a result, there will significant increases, not only in the numbers of patients with cancer-related emergencies but also the numbers of those with known malignancy presenting to acute medical units (AMUs).
Patients with cancer account for about 15% of all acute inpatient hospital stays and half of all spending on patients with cancer is spent on delivering this care.4,5 In total, 40% of cancer admissions are non-elective and managed by acute medical teams.5 The National Chemotherapy Advisory Group (NCAG)'s report, published in 2009, therefore recommended that all hospitals with an emergency department develop an acute oncology service.5 This team was envisaged to manage patients with complications of cancer and cancer treatment and those presenting as emergencies with previously undiagnosed cancer.
We examined the burden of patients with cancer presenting to an AMU, analysing the reasons for presentation and the role of the acute physician in the management of this cohort.
Methods
A retrospective analysis performed at a university hospital in the north west of England in May 2011 examined 300 consecutive admissions to the AMU. The patient's age, sex, reason for admission, date of admission, previous medical history, presenting complaint and length of inpatient stay were collected using a pro forma. The reason for admission was then classified according to the following categories:
Patients known to have cancer:
-Presentation due to a direct complication of the cancer
-Presentation due to a complication of cancer therapy
-Presentation due to palliative care needs
-Presentation equivocally or not related to cancer.
Patients not known to have cancer:
-Cancer not diagnosed during admission
-Cancer diagnosed during admission
-Investigations ongoing at time of data analysis.
The presenting complaint was divided into one of 21 categories. These were the ‘top 20’ common presentations of the acute internal medicine (AIM) and general internal medicine (GIM) curricula, with ‘others’ representing presentations outside of these 21 categories.
Results
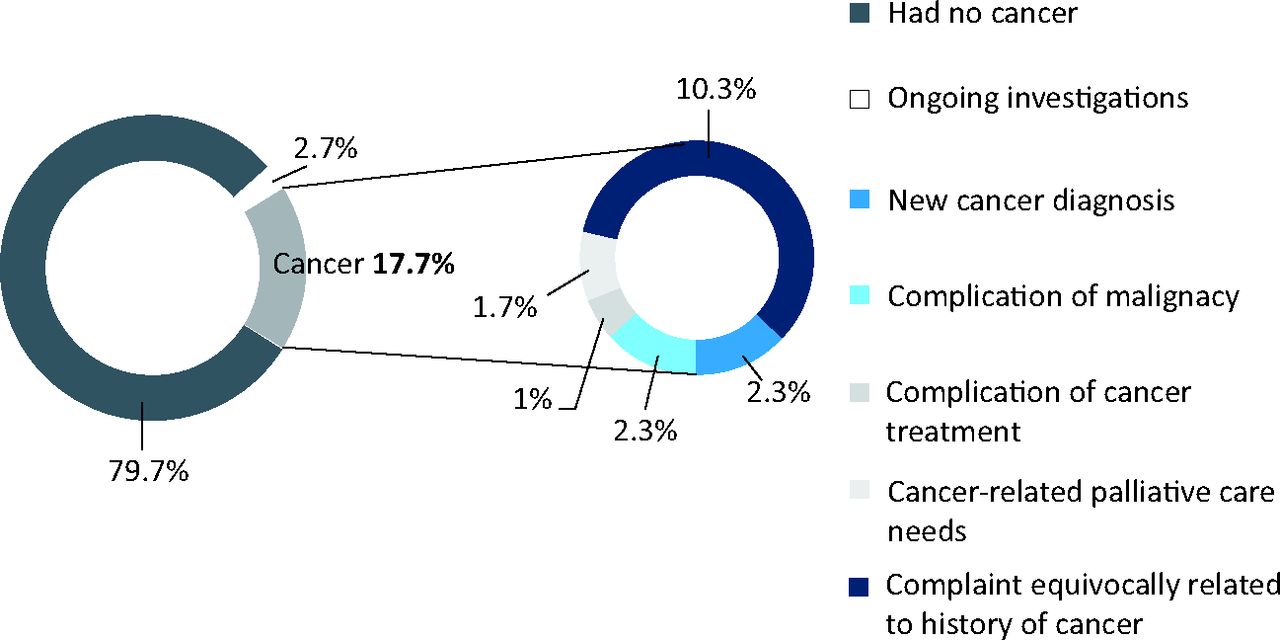
Of 300 consecutive patients admitted to the AMU, 137 (45.7%) were men and 163 (54.3%) were women. The median (range) age of the patients was 70 (16–98) years. Overall, 46 (15.3%) admitted patients had a history of cancer: seven (2.3%) had a new diagnosis of cancer made during the admission, 239 (79.7%) admissions were unrelated to cancer and eight (2.7%) patients were having ongoing investigations at the time of analysis (Fig 1).

Distribution of patients presenting to the acute medical unit according to whether their presentation was or was not related to cancer and their specific cancer status.
Of the 46 patients with known cancer, seven presented due to direct complications of the cancer, three due to complications of cancer treatment and five due to palliative care needs, with 31 presentations equivocally or not related to the cancer (Fig 2). The latter group included falls (22.6%), breathlessness (19.4%), limb swelling not caused by venous thromboembolism (16.1%), cardiac chest pain (9.7%) and headache (3.2%).
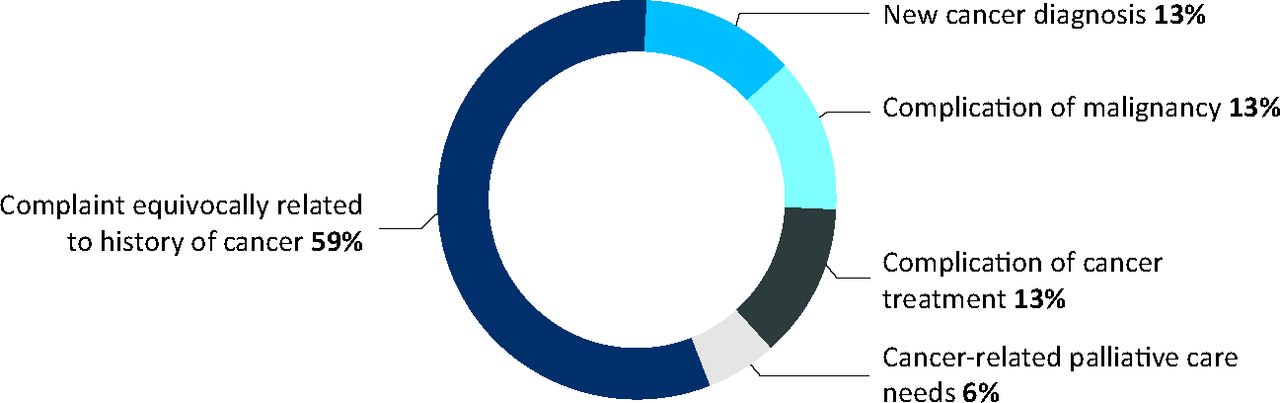
Distribution of patients with cancer presenting to the acute medical unit according to the underlying reason for their presentation.
Fig 3 compares the presenting complaints of patients with cancer with those without cancer. As a percentage of the admissions, limb pain and swelling, breathlessness, falls and abdominal pain were more common reasons for presentation in the patients with cancer.

Underlying reasons why patients with and without cancer presented to the acute medical unit.
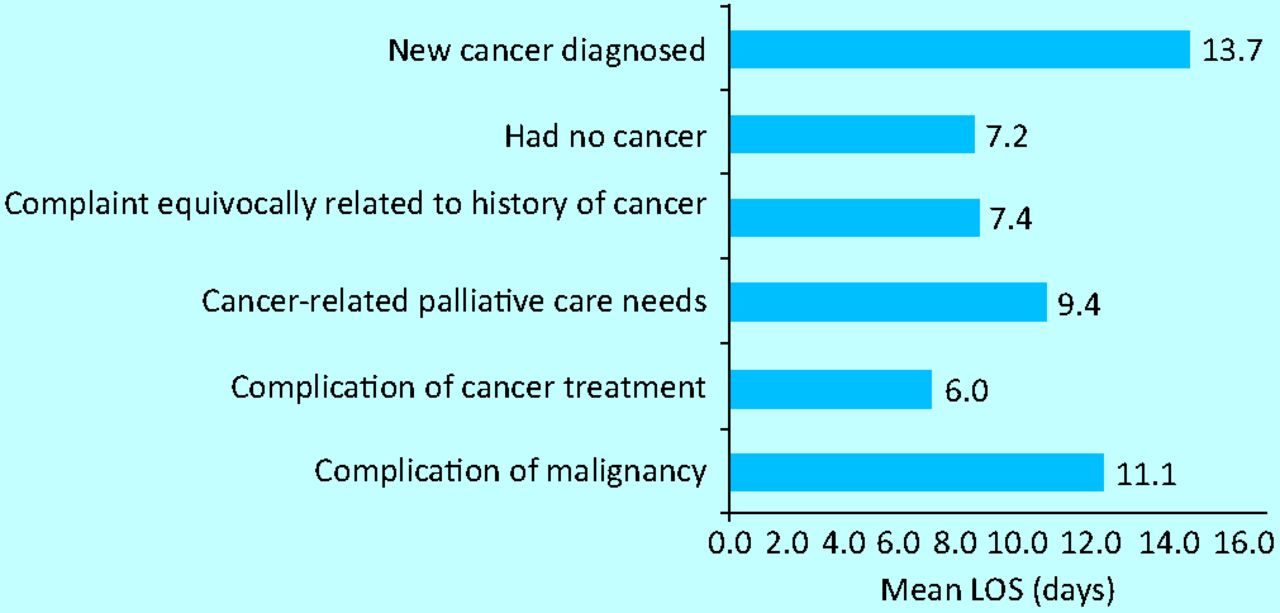
Patients with cancer had a statistically significantly longer average length of inpatient stay than patients without cancer (8.8 days vs 7.2 days, p<0.01) (Fig 4). Fig 5 shows the subgroup analysis of the length of stay based on the relation to cancer for admission. Patients with complications of cancer treatments had a shorter average length of inpatient stay, which was longest for patients with direct complications of cancer and a new diagnosis of cancer.
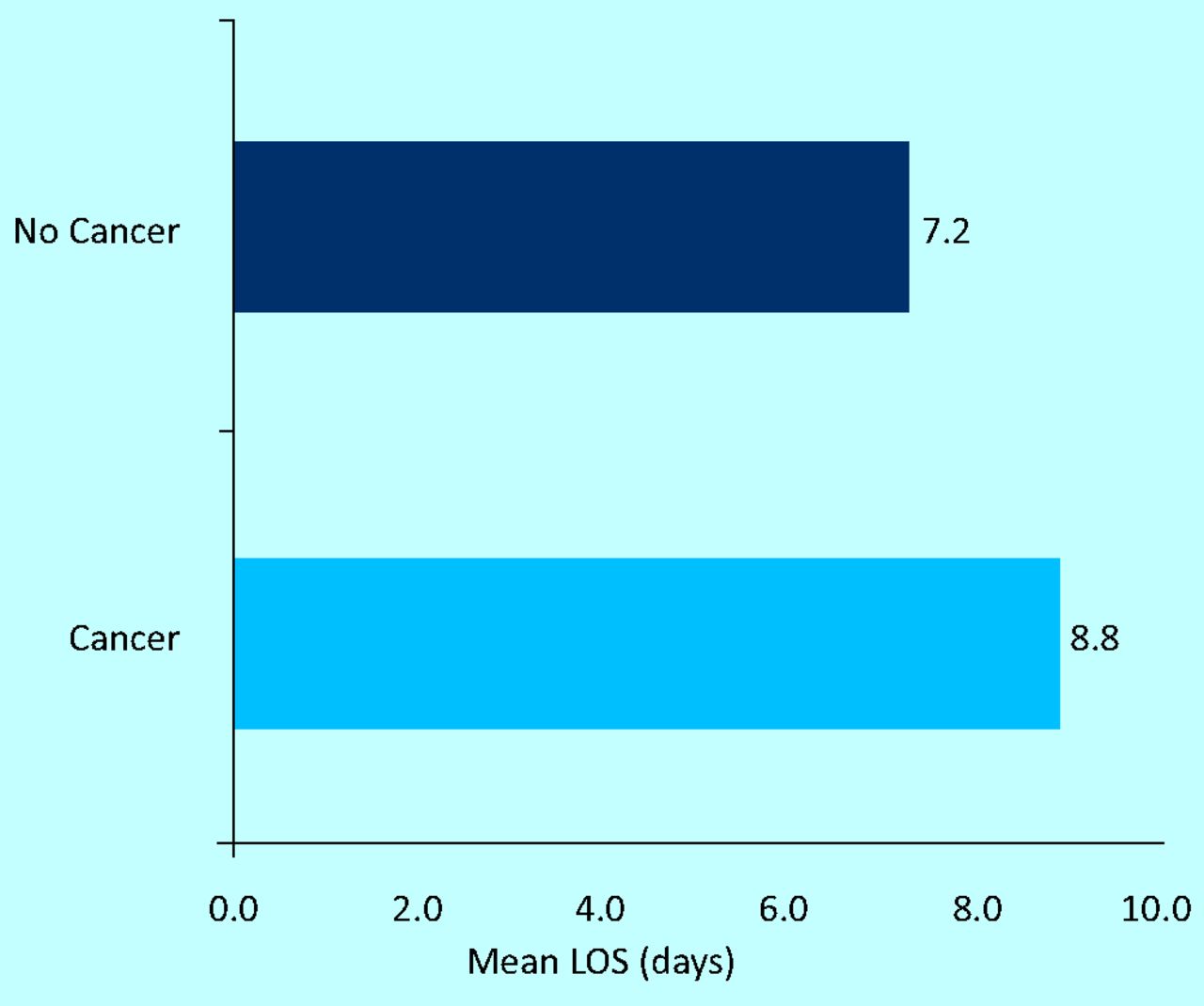
Average length of stay of patients with and without cancer who presented to the acute medical unit. LOS = length of stay.

Average length of stay of patients with cancer who presented to the acute medical unit according to the underlying reason for their presentation. LOS = length of stay.
Discussion
The development of acute oncology services is envisaged to improve the management of patients with cancer who present as emergencies. It is anticipated that care of these patients will be streamlined due to decreased length of inpatient stay and earlier specialist input to assist in the development of an appropriate management plan.1,4,5
Patients admitted with progression of cancer or initially presenting with symptoms suggestive of advanced malignancy often have a poor performance status and a significant proportion die during the admission.6 The National Cancer Intelligence Network (NCIN) reported that 23% of new diagnoses of cancer presented as emergency admissions and that this cohort had a significantly worse 1-year survival rate.7 These patients can receive multiple futile investigations, but early input from oncology could help reduce this, facilitate discussion with the patient and their families, and enable early involvement of palliative care.
It is proposed that acute oncology services should help in the management of three groups of patients: those with complications of cancer, those with complications of cancer treatment and those who present as emergencies due to a new diagnosis of cancer. Our data show that most patients with cancer who present to the AMU have symptoms that are equivocally or not related to their malignancy. These patients also have longer inpatient stays, and they may benefit from optimisation of their cancer management plan, particularly if they have a further diagnosis that will affect their performance status. It is important that acute physicians consider this aspect of their care and liase closely with oncology services.
NHS Improvement described four ‘winning principles’ for the inpatient care of patients with cancer,7 including assessing patients with cancer before a formal decision to admit. This role is likely to be performed predominantly by acute physicians in AMUs, facilitated by liaison with the acute oncology service.
Conclusion
Patients with cancer account for a significant percentage of admissions to the AMU and have longer inpatient stays. As the incidence and prevalence of cancer increases, the challenge of improving the experience of patients with cancer, as well as safety and outcomes, becomes more important. Development of successful acute oncology services with close working relations with acute physicians will be essential to achieve this.
- © 2013 Royal College of Physicians








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}