
Abstract
Chest pain can be a manifestation of aortic pathology and must be considered in any patient with a history of chest trauma, hypertension, atherosclerosis, connective tissue disorder and/or radiographically abnormal aortic contours. Acute intramural haematoma can resemble acute myocardial infarction and can be life-threatening if not correctly diagnosed. Electrocardiogram (ECG) must be carried out in all patients as it helps distinguish acute myocardial infarction (for which antiplatelets and anticoagulants may be life-saving) from intramural haematoma (for which these drugs may be detrimental). Other imaging modalities may be considered depending upon the clinical situation.
Lesson
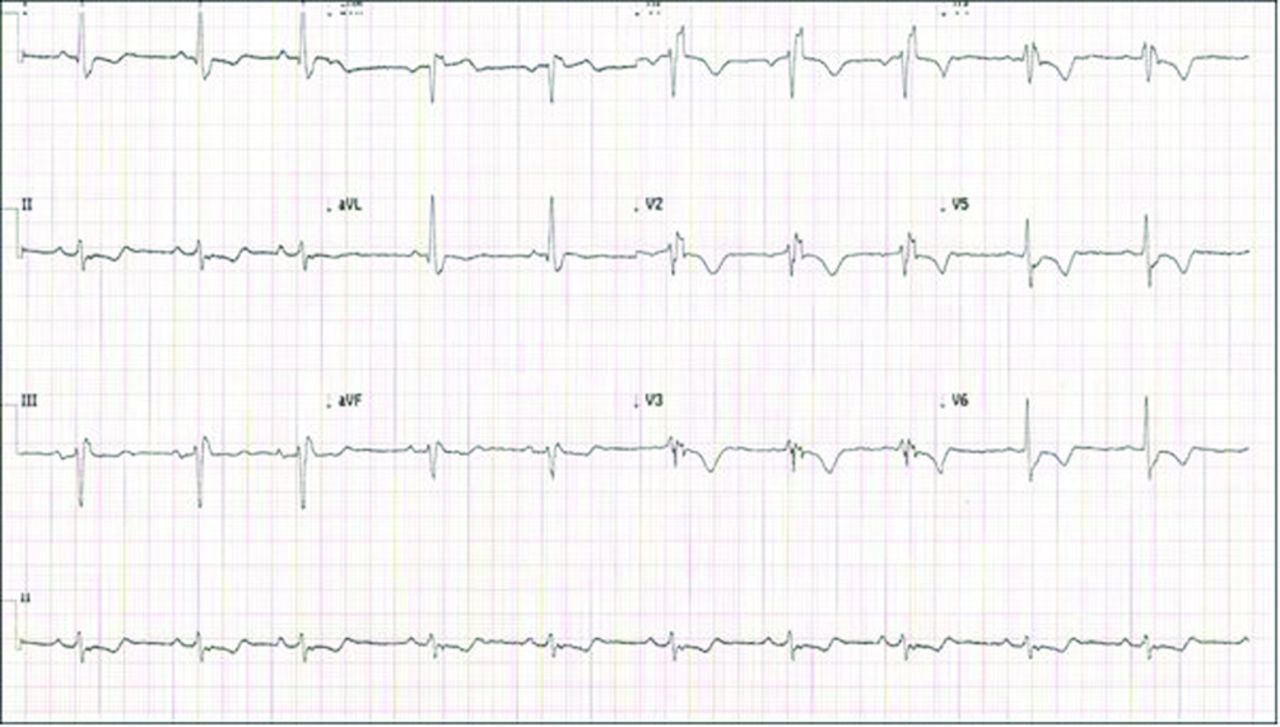
A previously fit and healthy 64-year-old woman presented with central chest pain and shortness of breath on exertion. She described the chest pain as being like someone pressing down on her chest, and it was associated with nausea. Her past medical history included a family history of premature ischaemic heart disease, hypertension and hyperlipidaemia. She was a smoker with a history of 50 pack-years. Her electrocardiogram (ECG) showed sinus rhythm, right bundle branch block and T-wave inversion in inferior and antero-lateral leads (Fig 1).
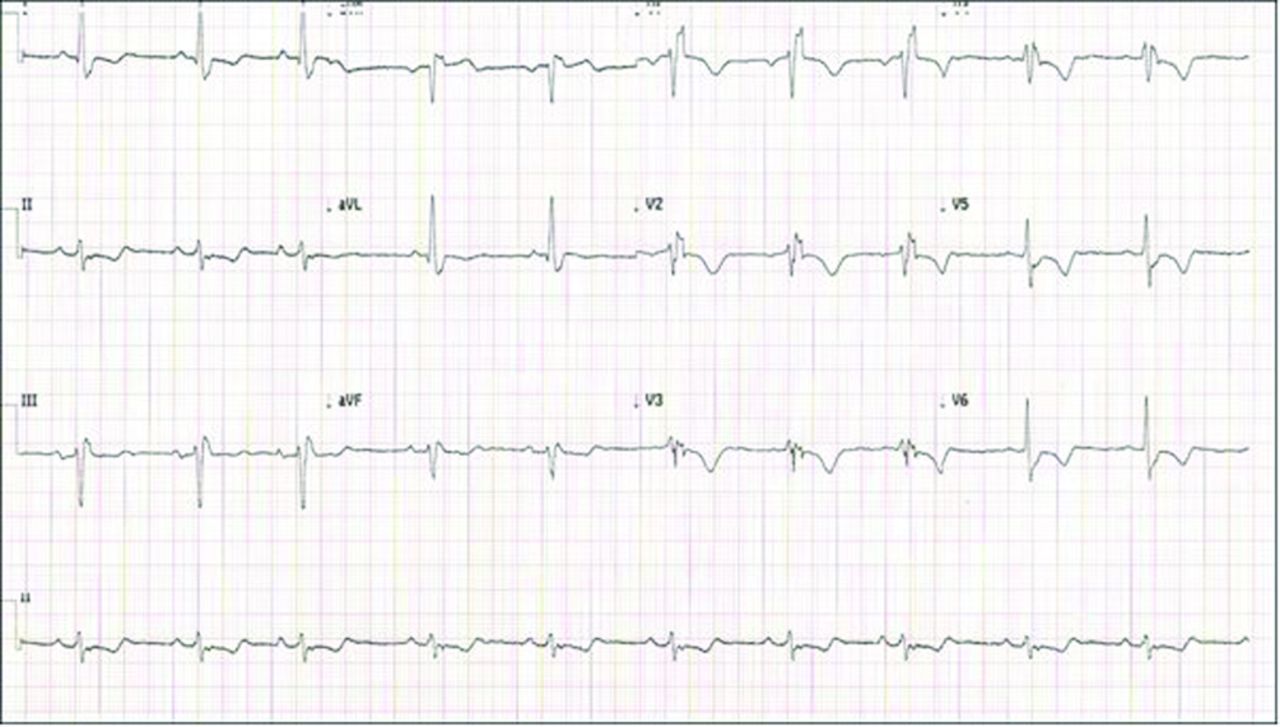
12-lead ECG showing right bundle branch block with T-wave inversion in inferior and antero-lateral leads. ECG = electrocardiogram.
On physical examination, she was anxious, with a blood pressure (BP) of 125/80 mmHg in both the arms and a regular pulse of 78 beats-per-minute. Oxygen saturation was 95% on 2 l of oxygen. Cardiac examination revealed normal S1 and S2 without any murmurs. Her chest was clear on auscultation and her abdomen was soft and non-tender, without organomegaly. Extremities were normal with bilateral symmetrical, palpable pulses.
Acute coronary syndrome (ACS) was suspected, so the patient was loaded with dual antiplatelet therapy and was transferred to the coronary care unit for further management. She continued to have chest pain and was therefore commenced on intravenous (IV) nitrate infusion.
Her blood tests showed haemoglobin 14.7 g/dl, white cell count 11 × 109/l, platelet count 242 × 109/l, sodium 141 mmol/l, potassium 4.2 mmol/l, urea 6.1 mmol/l and creatinine 57 μmol/l. Her troponin was negative. A trans-thoracic echocardiogram showed good left ventricular function with no regional wall motion abnormalities, mildly dilated proximal ascending aortic diameter at 3.9 cm and a trace aortic regurgitation.
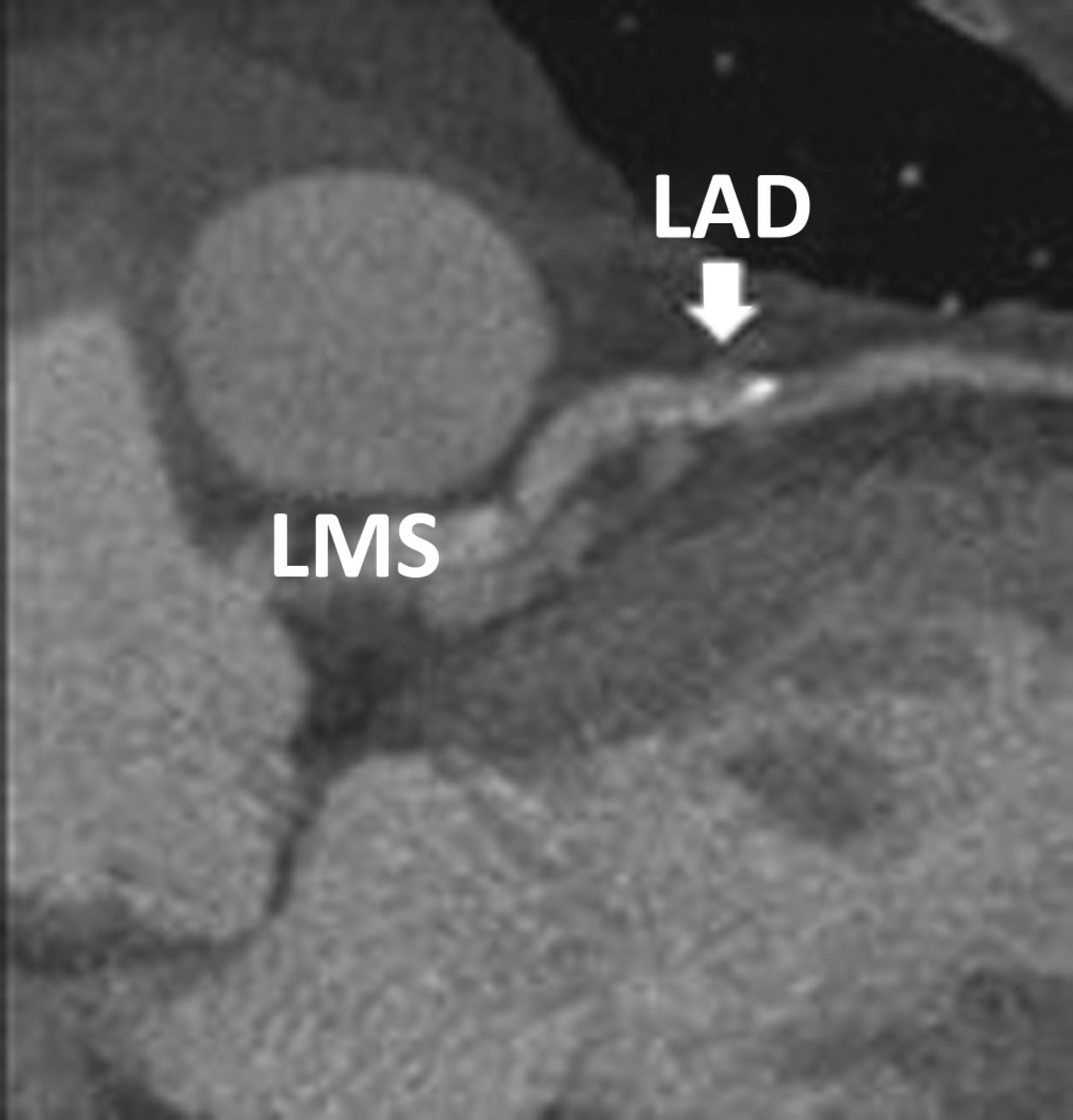
Her chest pain did not improve and therefore other differentials were considered. An urgent computed tomography (CT) aortic angiogram was carried out, which revealed an acute intramural haematoma of the thoracic aorta starting from just above the aortic valve, involving the whole of the ascending aorta, aortic arch and the descending thoracic aorta, and extending down to the diaphragmatic hiatus causing significant narrowing of the lumen-containing contrast (Fig 2). It also showed a significant disease of the left anterior descending (LAD) (Fig 3) and right coronary artery (RCA).

CT aortic angiogram showing an acute intramural haematoma of the thoracic aorta causing significant narrowing of the lumen containing contrast (shown by arrows). As aorta = ascending aorta; CT = computed tomography; Des aorta = descending aorta.
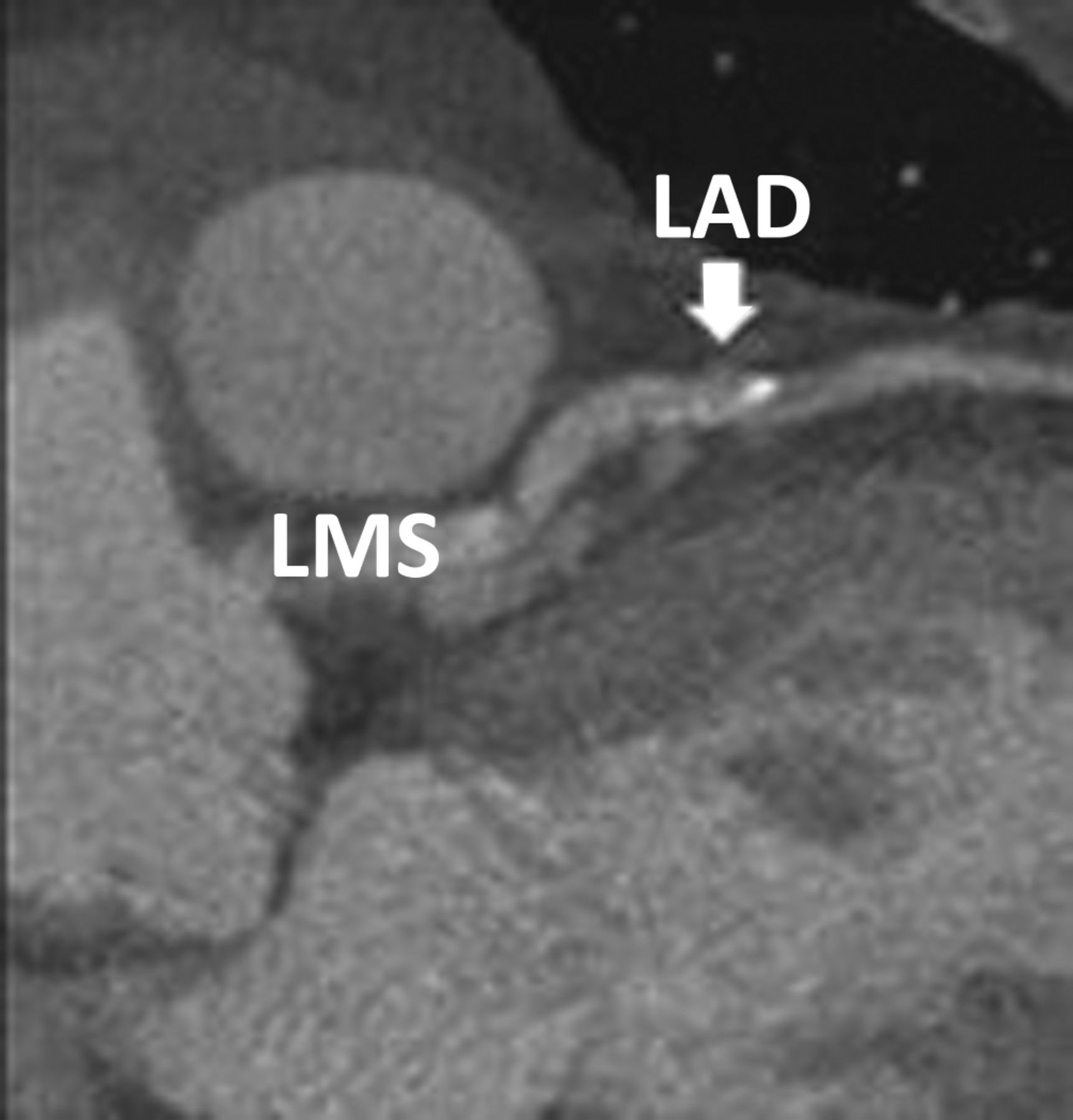
CT angiogram showing calcification and significant disease of the LAD artery (shown by arrow). CT = computed tomography; LAD = left anterior descending artery; LMS = left main stem.
The patient was immediately transferred to the cardiothoracic surgical centre. The intramural haematoma was removed and the ascending aorta was replaced with an interposition aortic root graft. She also underwent coronary artery bypass grafting including a vein graft to the LAD and a vein graft to the posterior descending artery (PDA). She seemed to have recovered well when reviewed at 6-week follow up.
Background
Intramural haematoma (IMH) is an uncommon, but potentially lethal, form of acute aortic syndrome (AAS). Acute IMH represents a novel variant of dissection characterised by the absence of an entrance tear.1–2 IMH may be the result of ruptured vasa vasorum, which at first appears normal. Ruptured vasa vasorum are not supported by the surrounding aortic media or the result of rupture of diseased vasa vasorum.3 As a dissection, the haematoma can extend along the aorta.
Acute IMH accounts for 5–20% of all AAS cases, with regression in 10%, progression to classic aortic dissection in 28–47% and a risk of rupture in 20–45%.4 Two-thirds of cases are located in the descending aorta and are typically associated with hypertension.4 Patients with IMH are typically somewhat older than those with classic dissection, supporting the notion that degenerative changes in the media are of particular importance in the evolution of this pathology.5
Evangelista et al studied 1,010 patients with acute aortic syndromes who were enrolled in the International Registry of Aortic Dissections (IRAD) between 1 January 1 1996, and 19 November 2001 and found that 58 (5.7%) patients had IMH.6 This cohort tended to be older (68.7 vs 61.7 years, p<0.001) and more likely to have distal involvement (60.3% vs 35.3%, p<0.0001).
Arterial hypertension is the most frequent predisposing factor for IMH and is present in 84% of the patient cohort. Similarly there is a 67% incidence reported in a post mortem study of 161 cases of dissection.7 Other predisposing factors are shown in Box 1.
Predisposing factors of aortic dissection.

Although clinical manifestations of IMH are similar to acute aortic dissection, IMH tends to be more of a segmental process. Therefore radiation to head or legs is less common. Chest and back pain is reportedly even more severe with IMH.6 Chest pain is more common with ascending (proximal – type A) IMH and upper or lower back pain is more common with descending (distal – type B) lesions.8 However, malperfusion and pulse deficit are decidedly rare in IMH.5
Diagnosis
An ECG must be carried out in all patients as it helps to distinguish acute myocardial infarction (AMI) from IMH. Both conditions may co-exist as the dissecting membrane may extend into a coronary ostium causing acute myocardial ischaemia. About 20% of patients with type A dissection have ECG evidence of acute ischaemia or AMI.9 Patients with suspected aortic disease and ECG evidence of ischaemia must undergo diagnostic imaging before thrombolytic therapy is administered.
Chest radiography may show widening of the aorta with intramural haematoma. About 10–20% of patients will have completely normal chest X-ray. Because of the limited sensitivity, additional imaging studies are required in almost all patients (98% in IRAD patients).10
Transthoracic echocardiography (TTE) can be used as a screening tool for the diagnosis of IMH of proximal aorta. This is useful in rapid evaluation of aortic insufficiency, pericardial tamponade, arch vessel involvement and left ventricular systolic function.
Trans-oesophageal echocardiography (TOE) is highly sensitive and specific in diagnosing thoracic aortic pathologies. The diagnosis of an IMH is characterised by crescentic aortic wall thickening, the absence of intimal flap and a lack of false lumen colour flow typical of dissection. The primary limiting factor in the use of TOE is the requirement for a skilled echocardiographer to be immediately available to perform and interpret results in an emergency situation.11
CT scan is necessary for the diagnosis and treatment in patients with IMH. Nienaber et al demonstrated that the sensitivity of a thorax CT scan was nearly 100%.2 The multi-detector CT (MDCT) has been found to play an important role in the diagnosis of IMH.12 According to this report, the accuracy provided distinguished a chronic clot from an acute clot in the aortic wall.
Magnetic resonance imaging (MRI) may be superior to CT as it can differentiate IMH from atherosclerotic plaque.13 This is crucial as the two findings have completely different prognosis and the methods of treatment are different. Although MRI has the highest sensitivity and specificity for the detection of all forms of aortic pathology and provides superior anatomic detail when compared to other imaging modalities, it is limited by availability, expense and patient restrictions, such as pacemaker, aneurysm clips or other metal devices.
Management
The greatest challenge in managing IMH is to suspect, and thus diagnose, the disease as early as possible. Other differential diagnoses need to be considered (Box 2) and one also needs to be aware of less common presentations of this condition (Box 3).
Differential diagnoses of acute aortic dissection.

Common presenting signs and symptoms of acute aortic dissection.

Similar to type A and B aortic dissection, surgery is advocated in patients with type A IMH and initial medical therapy in patients with type B IMH. A meta-analysis of 143 patients found that patients with lesions of the ascending aorta had a lower mortality with surgery than with medical treatment. Thus, the cardiology and surgical communities have generally recommended that acute IMH involving the ascending aorta should be managed surgically due to unacceptably high mortality with medical treatment.8,14
According to one study15 on morbidity and mortality for 168 patients with IMH, ascending aortic IMH led to aortic dissection in 25%, aortic rupture in 28% and stabilisation in 28% of IMH patients. In comparison, descending IMH led to aortic dissection in 13%, aortic rupture in 9% and stabilisation in 76% of patients. In this study, the 30-day mortality was 18% with surgical repair of proximal IMH and 33% with surgery to distal IMH. In comparison, 30-day mortality was 60% and 8% with medical therapy of type A and type B IMH, respectively.15
The presence of IMH in the ascending aorta is commonly considered as an independent factor of progression to aortic aneurysm formation, aortic rupture and/or dissection.16 However, type A or proximal IMH is no longer related to early death when surgical intervention is performed.16 Alternatively, IMH of the descending aorta (type B or distal) may be treated conservatively or through endovascular intervention as elective cases.16,17
According to records, age and the use of β-blockers are factors contributing to the progression of IMH. In a report, only 7% of patients with late progression IMH were treated with β-blockers, compared to 49% of IMH patients without late progression.18 β-blockers work by reducing aortic wall stress and systolic arterial blood pressure (BP).15 One predictor of late progression IMH is younger age (<49 years)2 and medication without β-blockers.19
Persistent and/or recurrent pain despite medical treatment, or repetitive pleural effusion, is an important indicator of disease progression20 as it represents a blatant indication for surgical or interventional handling.17
Follow up
Close follow up in patients with IMH by a specialised team includes the assessment of aortic expansion, aneurysm formation, signs of leakage at anastomoses/stent site and malperfusion. The single most important factor is excellent BP control (<135/80 mmHg). After discharge, regular outpatient visits at 1, 3, 6 and 12 months, and thereafter every year, are recommended.
To follow up patients after medically or surgically treated IMH, MRI appears to be the technique of choice, followed by CT and TOE.
Conclusions
Physicians attending a patient with chest pain should be aware of a wider spectrum of conditions so that fatal conditions like intramural haematoma may not be missed. A timely diagnosis is the key in managing patients with this condition as mortality significantly increases within hours. Close teamworking and immediate liaison with the cardiothoracic centre helps in reaching a successful outcome.
Acknowledgements
We would like to thank the echocardiography and radiology departments of Southend University Hospital NHS Foundation Trust for providing the images for this case.
- © 2013 Royal College of Physicians
References








{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.